
Abstract
Introduction
To investigate the levels of nicotinamide
Materials and Methods
This prospective pilot study involved 152 adults without history of atrial fibrillation who underwent first
Results
Fifty-one patients (33.6%) experienced in-hospital POAF. NOX2 concentration in serum and pericardial drainage samples was increased after surgery, reached its peak at 12 h, and gradually declined thereafter toward the baseline levels by 24 h. At 12 h, patients with POAF had higher levels of serum NOX2 than those without (3.96 ± 0.35 vs. 3.70 ± 0.75 μg/mL, respectively, p = 0.004). There were no discernible differences in pericardial NOX2 between the 2 groups. Multivariate analysis revealed that serum NOX2 at 12 h post operation was the strongest independent predictor of POAF (odds ratio: 2.179, 95% confidence interval: 1.084–4.377). The area under the ROC curve of the POAF predictive model was 0.732 (95% confidence interval: 0.654–0.801).
Conclusion
Serum NOX2 may be useful in the identification of POAF. Larger studies are warranted to substantiate these findings.
Keywords
Introduction
Coronary artery bypass grafting (CABG) surgery has been widely adopted for myocardial revascularization (Glineur et al., 2016). However, despite its benefits, CABG is associated with the development of cardiac
The studies performed thus far have not investigated the role of NOX2 in the onset of POAF after isolated CABG or the dynamic changes in its levels within 24 h after surgery. Interestingly, there is documented divergence between the incidence rates of POAF following cardiac
Materials and Methods
Design and Study Population
The study was performed in accordance with the principles of the Declaration of Helsinki. This investigation was approved (approval code: Z2019SY26) by the ethics review board of Capital Medical University. All patients provided written informed consent for their participation.
This prospective observational pilot study was conducted at the Department of Cardiac Surgery of Anzhen Hospital, a tertiary referral hospital in Beijing, China. Adult patients (age: ≥18 years) with sinus rhythm who were admitted to the department from March 2021 to January 2022 and underwent first-time elective isolated CABG were consecutively recruited. The exclusion criteria were: history of AF or other atrial arrhythmias and inflammatory disorders; occurrence of myocardial infarction and cardiac surgery within the previous 6 months; combination with other cardiac surgery (e.g., valve repair/replacement, or emergent CABG); repeated exploratory thoracotomy, severe heart failure (New York Heart Association Classification Ⅳ); terminal malignancy; and treatment with immunosuppressive and antioxidant medications. Patients with hepatic disease (i.e., more than 3
Data Collection
Data including preoperative, intraoperative, and postoperative factors were prospectively recorded by 2 trained investigators. Regular checks of data for missing values or incorrect entries were carried out.
Sample Collection
Preoperative venous blood samples were collected in vacutainer tubes after induction of anesthesia. Baseline pericardial fluid samples were obtained immediately after opening the pericardium using a sterile syringe without a needle. All surgical procedures were performed by a single professional surgical team. Blood samples were maintained at room temperature for 60 min. Samples of serum and pericardial drainage were centrifuged at 3000 r/min for 15 min at 4°C (Centrifuge 5804R, Eppendorf, Germany). Subsequently, the supernatants were collected and frozen at −80°C until analysis. NOX2 levels were determined using an enzyme-linked immunosorbent assay kit (Yanyu Trading Co., Ltd., Shanghai, China) with intra- and inter-assay variability <10% and the lowest detection limit of 0.625 μg/mL. All assays were performed according to the instructions provided by the manufacturers, and the results were analyzed by 2 laboratory technicians who were unaware of the clinical status of patients. The test results became available to the investigators only at the end of the study. Extra blood and pericardial drainage samples were simultaneously obtained from all patients at 4, 12, and 24 h after the operation. To ensure accuracy, the postoperative pericardial drainage tube was maintained empty for at least 1 h prior to sample collection. In almost all patients, the pericardial drainage tubes were removed by 48 h. The pericardial drainage tube was withdrawn when the cumulated volume was <200 mL/24 h.
POAF Monitoring
The primary endpoint was the incidence of POAF, defined as any episode of characteristic AF rhythm (Hindricks et al., 2021) lasting >30 s or requiring medical intervention. Postoperatively, the heart rhythm of patients was continuously monitored using a wearable Holter monitor (RhythmWatchTM; MicroPort Medical Co., Ltd., Shanghai, China) until discharge from hospital. The accuracy of this equipment for the detection of AF is equivalent to that of a 12
Statistical Analysis
Data are expressed as mean ± standard deviation or median (interquartile range) and percentage of the total (%). The distribution of parameters was examined using the Kolmogorov–Smirnov test. Differences between groups were assessed using Student’s t
Sample Size Estimation
The sample size was calculated through the logistic regression method using the PASS 15 (NCSS, LLC, Kaysville, UT, USA) software. Previous trials reported that NOX is an independent predictor of AF, with an odds ratio (OR) ranging 1.01–2.41 (Liu et al., 2015; Kim et al., 2008). An OR of 1.90 was adopted in this study to gain a conservative sample size. It was estimated that 121 patients would provide a 2
Results
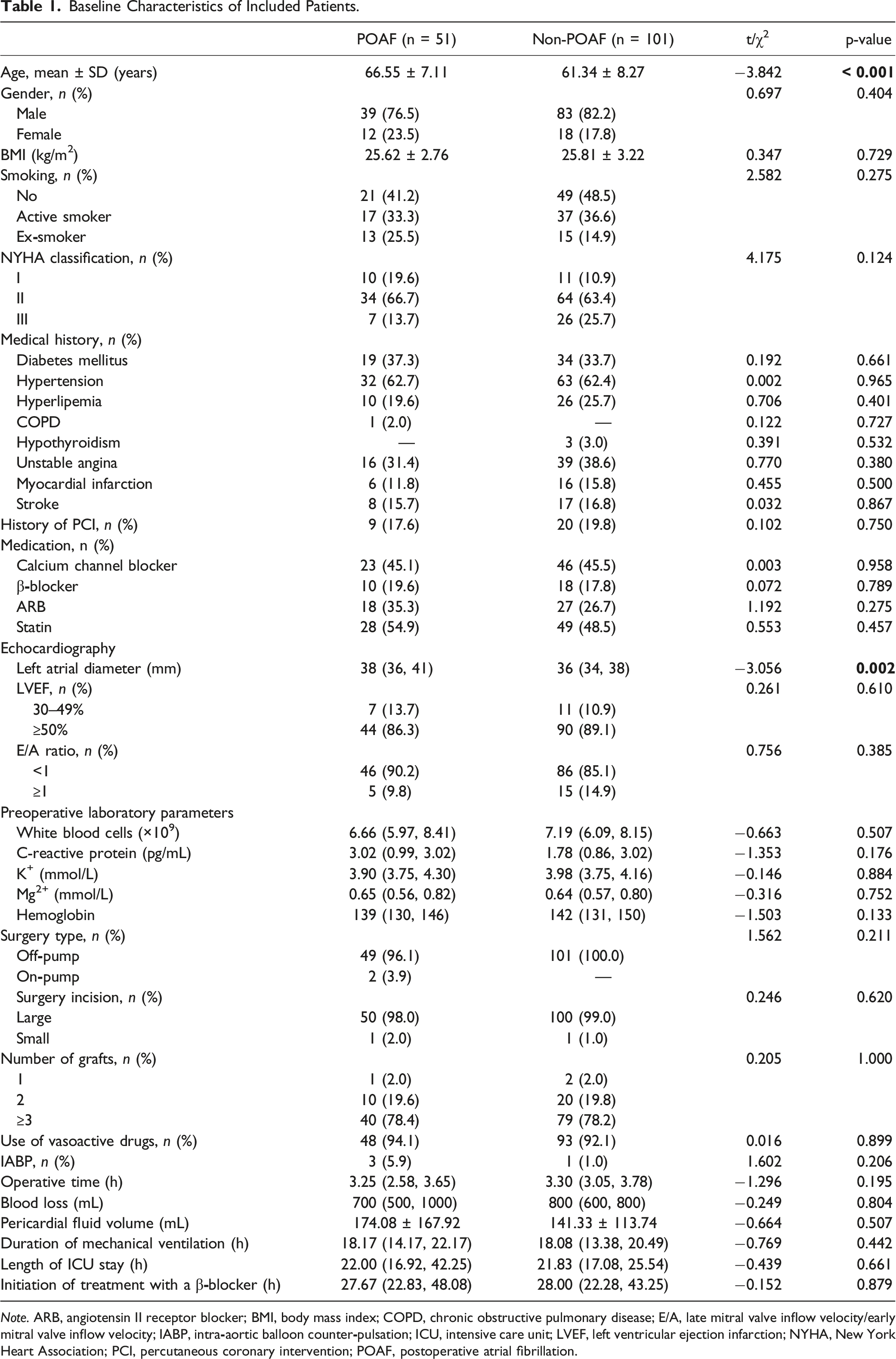
A total of 152 patients were included in this study; Figure 1 shows the flowchart of patient enrollment. Overall, 51 patients (33.6%) developed in-hospital POAF; in 78.4% (n = 40) of those, POAF occurred within 48–72 h post operation. The demographic and clinical characteristics of the patients are summarized in Table 1. The mean age of the patients was 63.09 ± 8.25 years (80.3% males; 19.7% females). The 2 groups were similar in terms of cardiovascular risk factors, comorbidities, echocardiographic parameters, operative time, laboratory examinations, and numbers of grafts. Nevertheless, patients who developed POAF were older and had larger left atrial diameter than those who remained in sinus rhythm after CABG. Flowchart of patient enrollment. POAF, postoperative atrial fibrillation. Baseline Characteristics of Included Patients. Note. ARB, angiotensin II receptor blocker; BMI, body mass index; COPD, chronic obstructive pulmonary disease; E/A, late mitral valve inflow velocity/early mitral valve inflow velocity; IABP, intra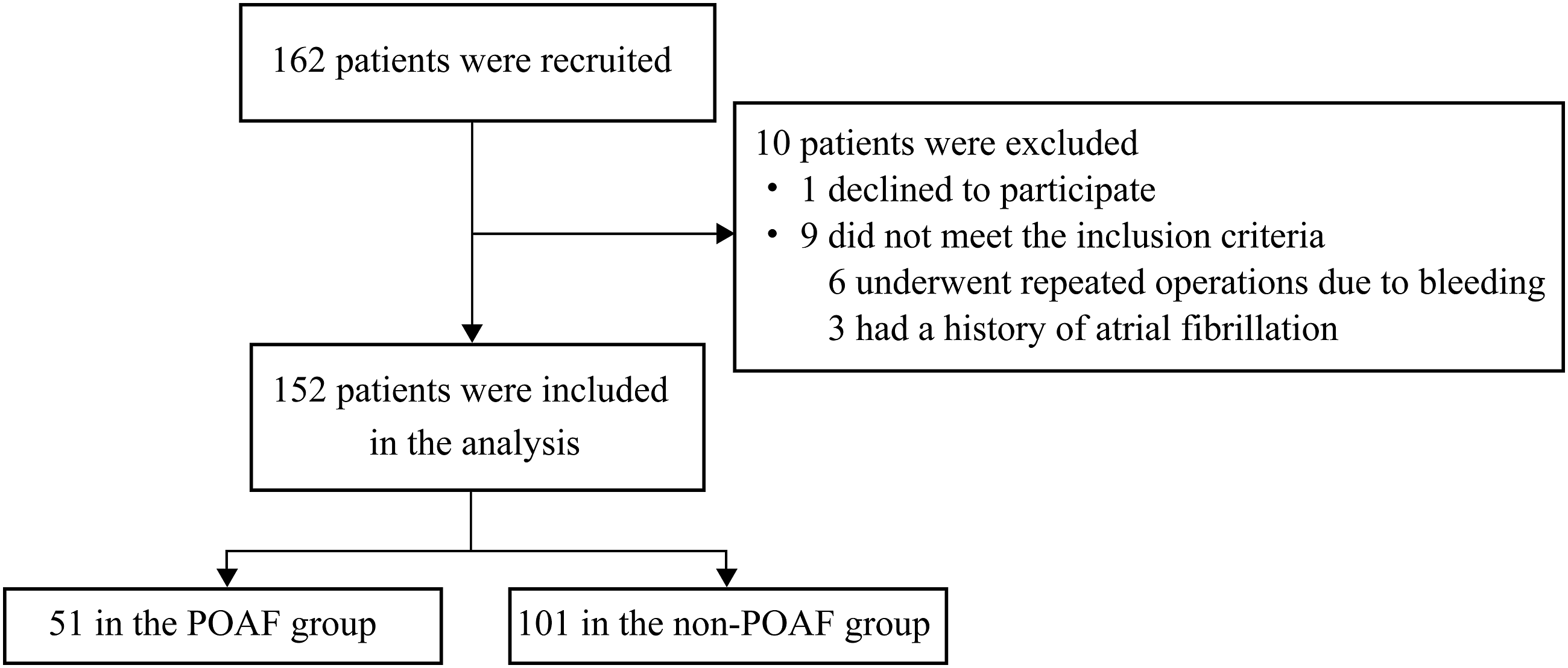
Trends of NOX2 Levels During the Early Postoperative Stage
In all patients undergoing CABG, the concentration of NOX2 in both serum and pericardial drainage samples was continuously increased post operation, reached its peak at 12 h, and gradually declined thereafter toward the baseline levels by 24 h. NOX2 activity was apparently elevated in the serum compared with pericardial drainage samples at the corresponding time points (Figure 2). Trends of NOX2 levels measured in serum and PD samples within 24 h post operation in patients who underwent CABG. CABG, coronary artery bypass grafting; NOX2, nicotinamide-adenine dinucleotide phosphate oxidase 2; PD, pericardial drainage.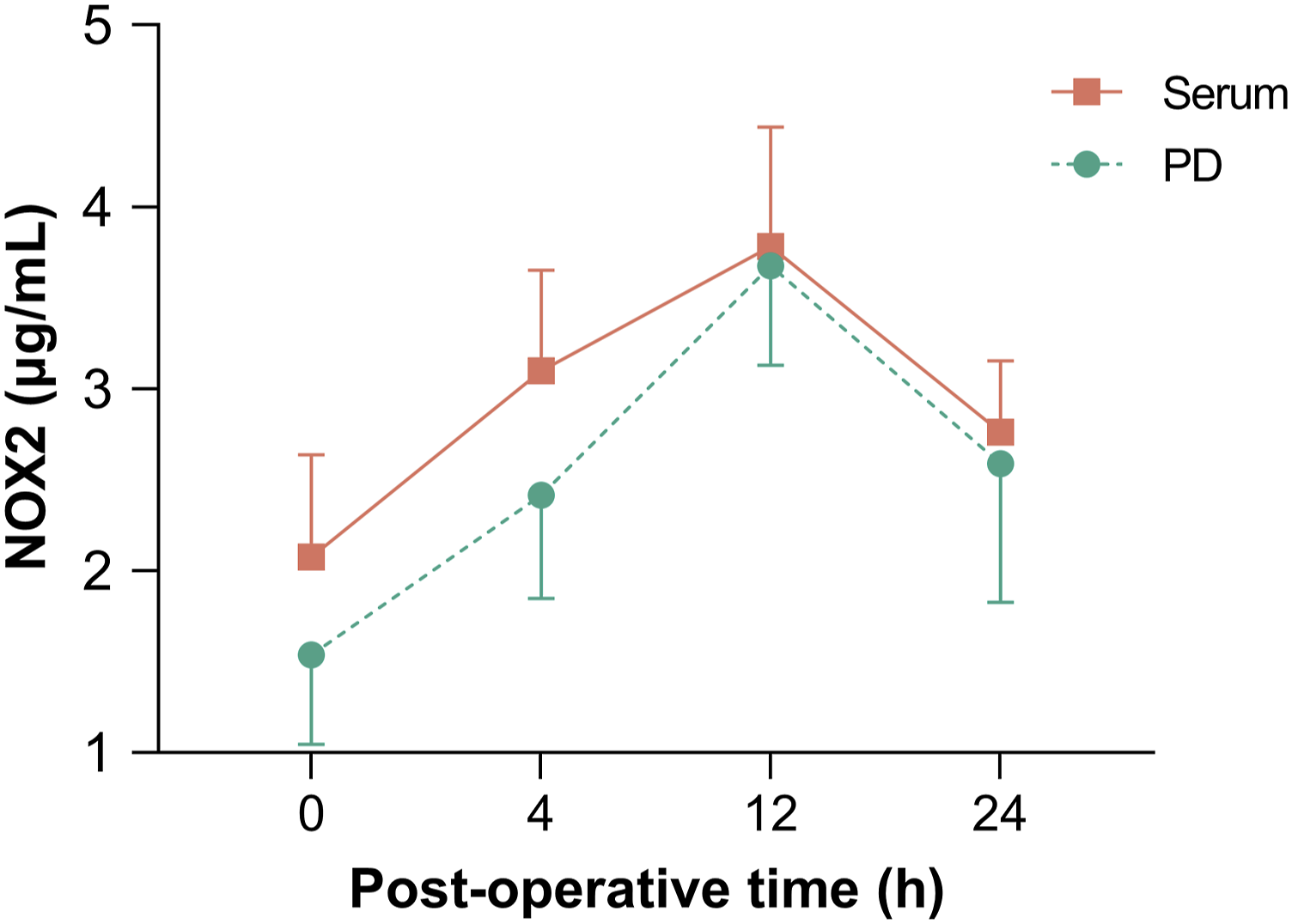
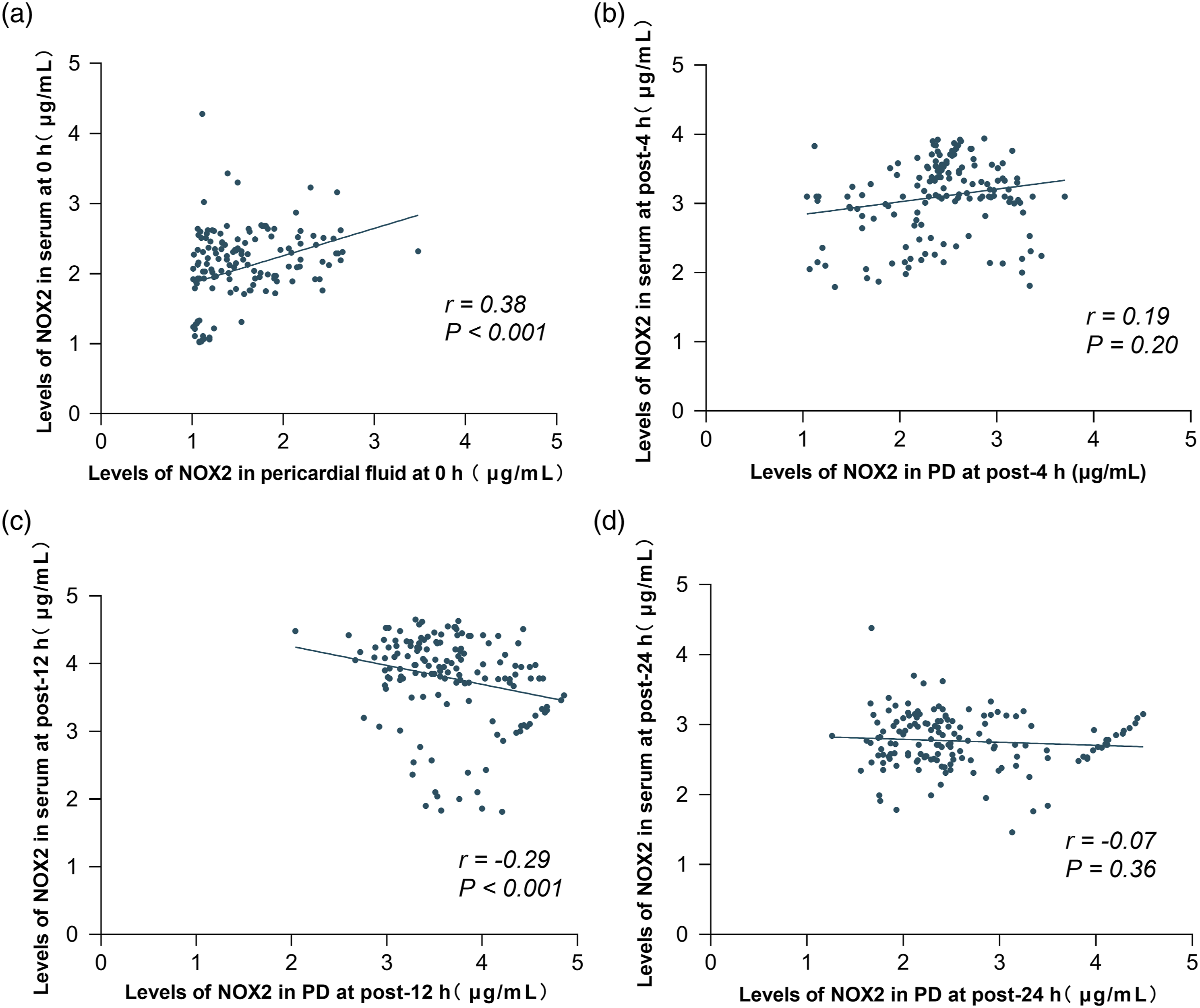
Comparison of NOX2 Activity in Serum and Pericardial Drainage Samples After CABG in Patients With and Without POAF
Repeated analyses of variance revealed significant differences in between Comparison of NOX2 levels in serum and PD samples obtained from patients with and without POAF at different time points. ( Correlation analyses of NOX2 levels between serum and pericardial drainage samples at different time points. (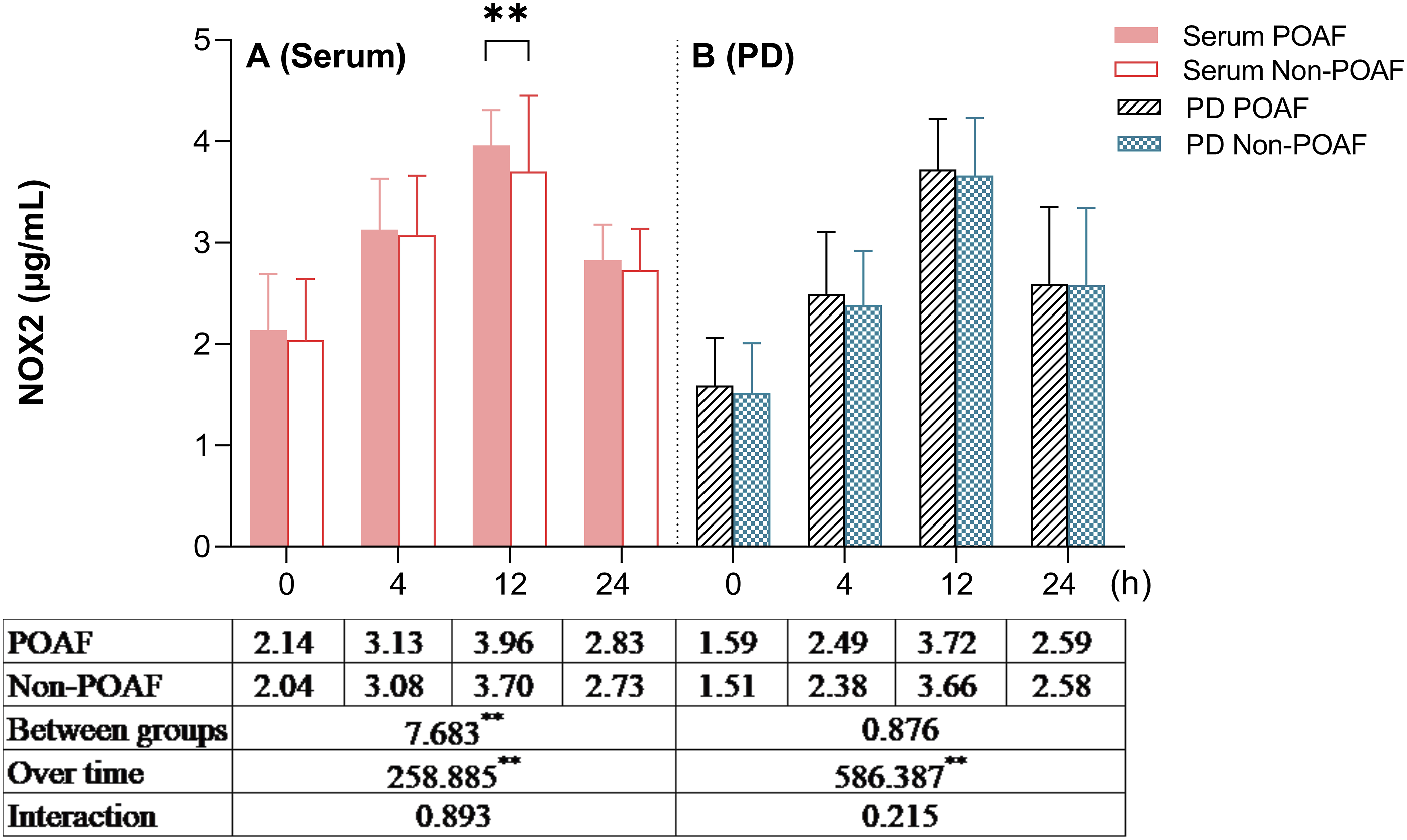
NOX2 was an Independent Risk Factor for POAF
Results of Logistic Regression Analyses.
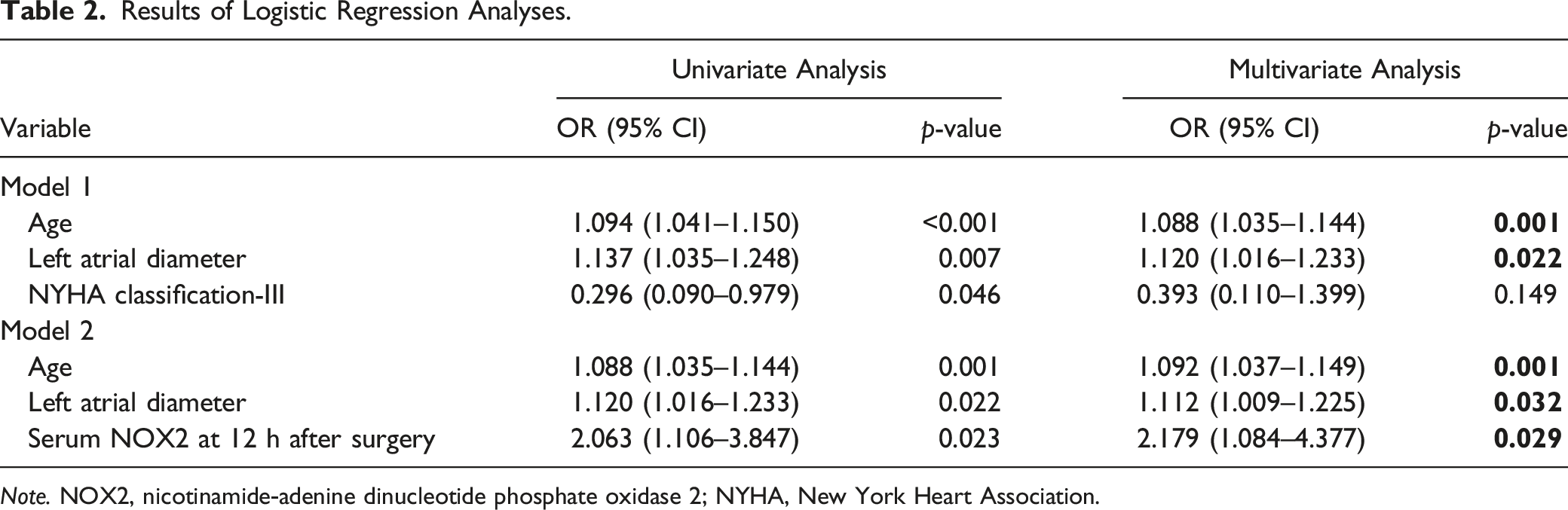
Note. NOX2, nicotinamide‑adenine dinucleotide phosphate oxidase 2; NYHA, New York Heart Association.
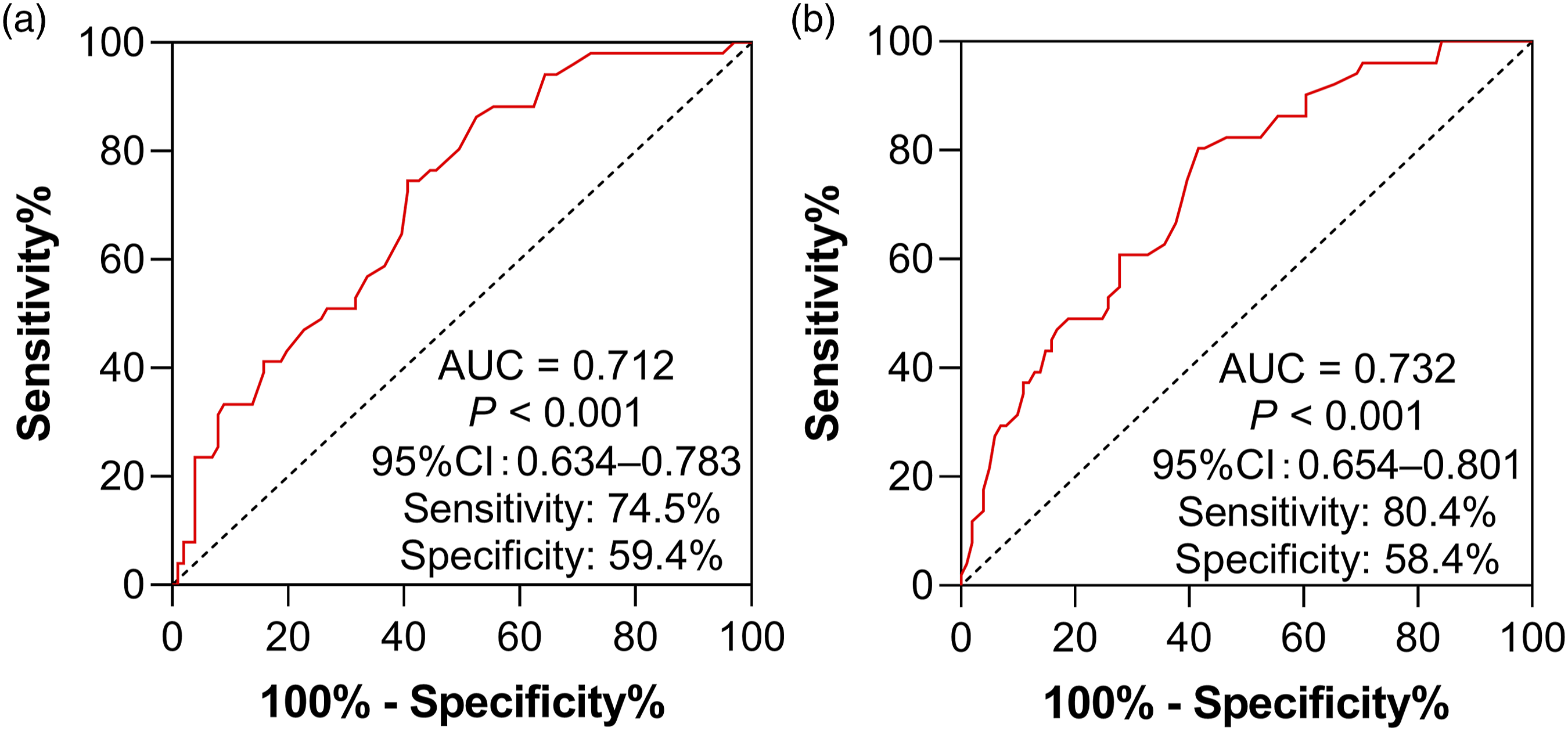
ROC curve analysis for the predictive models of POAF. (
Discussion
We uncovered that NOX2 activity measured in serum and pericardial drainage samples was dynamically altered in the early postoperative stage. Moreover, the levels of NOX2 were higher in patients who developed POAF after first-time elective isolated CABG compared with those who did not, implying that oxidative stress was immediately involved following surgery. Our preliminary data further suggests that the concentration of serum NOX2 at 12 h after surgery is an independent predictor of POAF.
Emerging evidence proposed the role of oxidative stress in the onset of POAF (Jayaram et al., 2022; Anderson et al., 2014). To the best of our knowledge, this is the first study investigating the association of NOX2 activity in serum and pericardial drainage samples with the occurrence of AF after isolated CABG surgery, particularly focusing on time-dependent changes. Experimental and clinical studies have shown that increased NOX2 activity is strongly linked to AF. More recently, researchers verified that transgenic mice with NOX2 overexpression displayed a 2
The time at which NOX2 levels reached their peak in our study, reflecting the strongest degree of oxidative stress, was consistent with that reported in a previous investigation (Kramer et al., 2015). Specifically, the concentration of NOX2 in serum at 12 h post operation was identified as a predictive factor for POAF, suggesting that NOX2 plays a functional role in the early initiation of POAF. This hypothesis has been supported by several previous studies (Reilly et al., 2011; Cangemi et al., 2012; Kim et al., 2008). Reilly et al. (2011) reported that the duration of AF varies depending on the source of ROS. In that study, the levels of NOX2 were significantly increased in goats after 14 days of AF and in right atrial tissue obtained from patients who developed POAF. However, these findings cannot account for the changes in atrial ROS noted in patients with longstanding AF. Moreover, the association between NOX2 and stages of AF was further explained and extended by subsequent data indicating that the levels of serum NOX2 were increased only in paroxysmal/persistent AF; statistically significant changes were not observed in patients with permanent AF and controls (Cangemi et al., 2012). Consistent with the current results, NOX2-generated superoxide from the human right atrial appendage at the time of cardiac surgery has been independently associated with the development of POAF (Kim et al., 2008). In the present study, there was no statistically significant difference between the AUC models (0.732 vs. 0.712, DeLong test; p = 0.33); while these data continue to indicate an improved discriminatory ability (ΔAUC = 0.020).
We were unable to recognize the influence of local NOX2 on the occurrence of POAF. Nevertheless, patients who developed POAF had numerically higher levels of pericardial NOX2 at measured points compared with those who did not.
In this study, the concentration of NOX2 at all time points after surgery was lower in pericardial drainage than in serum samples. A possible reason for this observation may be that local NOX2 was released from recruited leukocytes. Evidence has shown that oxidative stress in the postoperative pericardial space is largely attributed to the migration of inflammatory cells, particularly neutrophils and monocytes (St-Onge et al., 2018; Gaudino et al., 2022). These 2 types of leukocytes are primed for oxidative burst through activation of NOX2, followed by the release of hydrogen peroxide into this milieu (Kramer et al., 2015; St-Onge et al., 2018). As observed in Figure. 2, NOX2 levels in pericardial drainage samples were low under basal conditions; however, NOX2 activity gradually increased over time. Physiologically, NOX2 is mainly expressed in endothelial cells and cardiomyocytes (Bendall et al., 2002). Nevertheless, in the setting of CABG, activation of systemic NOX2 may be more relevant to the course of POAF versus activation in the pericardial environment. Although this hypothesis warrants further investigation, it may explain the lower concentration of NOX2 detected in the pericardial drainage versus serum samples. In agreement with previous data, patients who developed POAF were older and had longer left atrial diameter compared with those who did not. These characteristics are perceived as the basis of atrial fibrosis, possibly reflecting a preexisting susceptible atrial substrate that is indispensable for the generation of POAF (Corradi et al., 2020; Axtell et al., 2020; Akintoye et al., 2018; Yang et al., 2022).
Limitations
Due to the limitations of this study, the present findings should be interpreted with caution. Firstly, this study included a relatively small population. However, the total number of patients who were enrolled in the present study with 90% power was sufficient for the evaluation of differences between the 2 groups. Secondly, sample collection was terminated by 24 h after CABG based on the practical reality that the overwhelming majority of pericardial drainage tubes are removed by 48 h post-surgery. However, NOX2 exhibited predictive value for POAF as early as 12 h post-surgery. Thirdly, approximately 99% of patients underwent off
Conclusion
This preliminary evidence suggests a possible role of serum NOX2 in the predication of POAF. Studies with larger samples are needed to evaluate these results further.
Supplemental Material
Supplemental Material - Association Between Serum Levels of Nicotinamide-Adenine Dinucleotide Phosphate Oxidase 2 and the Development of Atrial Fibrillation After Isolated Coronary Artery Bypass Grafting: A Prospective Pilot Study
Supplemental Material for Association Between Serum Levels of Nicotinamide-Adenine Dinucleotide Phosphate Oxidase 2 and the Development of Atrial Fibrillation After Isolated Coronary Artery Bypass Grafting: A Prospective Pilot Study by Hui Yan, JiaYing Zhang, Fang Qin Wu, and Gui Fang Du in Biological Research For Nursing
Data Availability Statement
The data underlying this study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgments
The authors thank all participants and the clinical staff involved in this study for their valuable support.
Author Contribution
Hui Yan: conceptualization, design; acquisition, analysis, and interpretation of data; drafting and critical revision of the manuscript. Jia-Ying Zhang: design; acquisition of data; drafting of the manuscript. Fang-Qin Wu: conceptualization, design; analysis and interpretation of data; critical revision of the manuscript. Gui-Fang Du: design, acquisition of data; critical revision of the manuscript. All authors approved the final version of the manuscript and agree to be accountable for all aspects of work in terms of data integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (grant number 81970279).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.