
Abstract
Practical relevance:
Comprehensive examination of the feline fundus should be in every clinician’s arsenal. It is an integral part of both the physical and ophthalmic examination, especially in senior cats and in the presence of intraocular inflammation and visual impairment. Fundoscopy provides critical insight into a wide range of systemic diseases, often leading to quicker diagnoses and better treatment outcomes.
Clinical challenges:
Practice is needed to become proficient and take high-quality photos of the retina. Distinguishing between normal variants and pathological findings can be challenging initially.
Evidence base:
This review includes information from published references of common retinal pathologies in cats, as well as the authors’ extensive experience on performing fundoscopy.
Equipment:
The essential tools for fundoscopy include a direct and indirect ophthalmoscope, condensing lens and a focal light source. High-quality images of the fundus can be achieved with any smartphone.
Audience:
This review is aimed at veterinary clinicians and outlines all the steps and equipment needed to confidently perform fundoscopy. It also provides tips on how to capture photos of the fundus using a smartphone. Common findings are discussed in relation to different retinal pathologies.
Introduction
Fundoscopy is vital for diagnosing conditions such as retinal degeneration, hypertensive retinopathy and infectious diseases such as feline infectious peritonitis (FIP), while also enabling ongoing monitoring of disease progression and treatment response. With the advent of smartphone fundoscopy, capturing and sharing high-quality fundic images has become more accessible, enabling general practitioners to consult with specialists and enhance diagnostic accuracy.Integrating routine fundoscopy into clinical practice can lead to earlier diagnoses, better treatment outcomes and improved patient care.
Tools and techniques for performing fundoscopy
The two main techniques for examining the fundus are direct and indirect ophthalmoscopy. Each has its own advantages and disadvantages and they are complementary to each other. For example, if a lesion is identified with indirect ophthalmoscopy, direct ophthalmoscopy should be used to examine that lesion more closely. For information on the pros and cons of each technique, see Table 1 later.
Regardless of the technique used, it is important to follow a systematic approach when examining the fundus to avoid missing lesions. Key areas to assess are the optic disc (colour and size), the retinal vasculature (calibre, tortuosity and length), the tapetal fundus (reflectivity, pigment changes, haemorrhages, detachments) and non-tapetal fundus (pigment changes).
Direct ophthalmoscopy
The direct ophthalmoscope is readily available in all practices and provides an upright, magnified view of the fundus. To visualise the fundus, the lens dial should be set to zero. Clinicians who wear glasses should remove them and adjust the diopters according to their prescription using the lens dials. The light intensity should be kept low to avoid causing discomfort to the cat.


Equipment needed for fundoscopy. From left to right: Finoff transilluminator, direct ophthalmoscope and condensing lens. A pen torch, smartphone flashlight or strong otoscope light can also be used as a light source

The silver side of a Volk condensing lens rim should be facing the eye
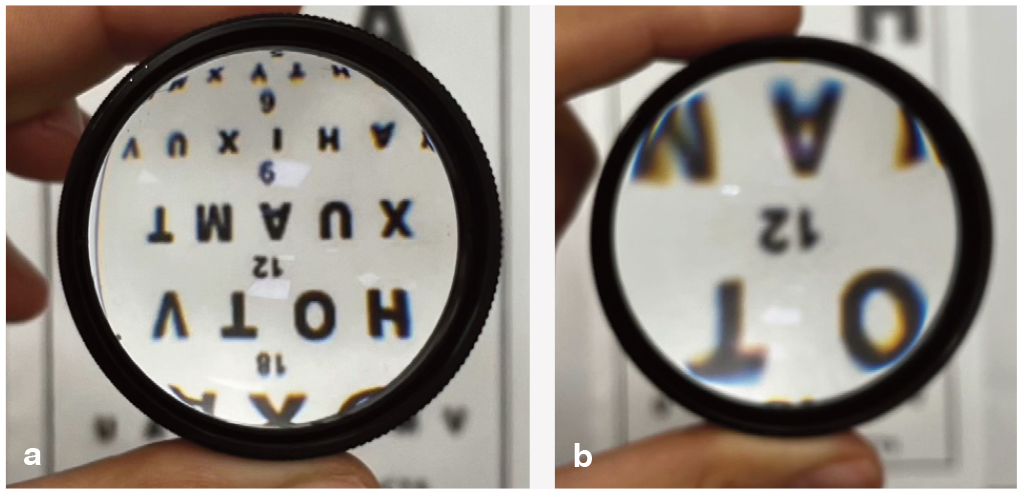
View with a (a) 30D lens compared with a (b) 18D lens

The Pan-Retinal 2.2 lens is considered the most versatile lens for the general practitioner
To examine the fundus, the ophthalmoscope should be rested on the clinician’s brow while visualising the tapetal reflex (otherwise known as the ‘tapetal reflection’), beginning at arm’s length. Once the tapetal reflex is visible, the clinician should gradually move closer until positioned 2-3 cm from the eye (Figure 5a). A systematic approach is recommended, starting with the optic disc and retinal vasculature, followed by the tapetal and non-tapetal fundus (see ‘Normal cat fundus’ box later).

(a) Direct fundoscopy. After finding the tapetal reflex from a distance, the clinician is moving closer to the eye to get to a position 2-3 cm away. (b) Indirect fundoscopy. The light source is held close to the clinician’s temple to achieve good alignment between the light, lens and pupil

Assessing the fundus in quadrants helps ensure no lesions are missed. If the view is lost, stepping back to locate the tapetal reflex before resuming the examination is advised.
Any lesions identified can be compared with the size of the optic disc. If a lesion is blurry at 0D but clear at positive diopters (eg, +2D), it means the lesion is elevated. Similarly, a lesion is depressed if it is in focus at negative diopters (eg, -2D).
Monocular indirect ophthalmoscopy
To obtain a clear view of the fundus, the light source should be positioned against the clinician’s temple. The condensing lens should be held between the thumb and index finger, with the silver side facing the eye, and stabilised on the cat’s head using one or two fingers. Once the tapetal reflex is visible, the lens should be positioned 2-4 cm from the eye (Figure 5b). If the image is lost due to head movement, removing the lens and repositioning is recommended.
This technique provides an inverted and reversed view of the fundus. Maintaining lens stability while adjusting position allows for a comprehensive examination of the entire fundus. More tips on indirect fundoscopy can be found in the box above.
The PanOptic ophthalmoscope is another tool for monocular indirect ophthalmoscopy, providing a real image with magnification that falls between direct and indirect ophthalmoscopy.
Table 1 compares direct and indirect ophthalmoscopy.
Pros and cons of direct vs indirect fundoscopy

Smartphone fundus photography: a practical, cost-effective tool for every clinician
Fundus photography is a powerful clinical tool for disease monitoring but also seeking specialist advice. While specialised fundic cameras can produce high-quality photos of the fundus, they are expensive. Smartphone fundoscopy offers a simple and cost-effective alternative.
This technique follows the same principles as indirect fundoscopy but uses the smart-phone camera as an indirect ophthalmoscope. The phone’s flash acts as the light source and the camera display screen replaces the examiner’s eye.
As with traditional fundoscopy, pupil dilation is necessary and the examination should be conducted in a darkened room to minimise glare from the environment. An assistant is again needed to restrain the cat and hold the eyelids open.
Capturing video and saving the best screen-shots is preferred over taking still photos, as it can be challenging to capture a well-focused image due to the cat’s eye and head movements.


Six layers of micropore tape were applied to reduce the intensity of the flash of this phone
Common issues and troubleshooting for smartphone fundus photography

Fundic findings
Congenital abnormalities
Congenital abnormalities are rarely reported in cats and they are usually associated with eyelid agenesis. Fundoscopic signs include coloboma of the optic nerve, retina and choroid. 6 Retinal dysplasia in the form of hyporeflective retinal folds may also be present.
Retinal dysplasia
Inherited eye disorders are relatively rare in cats. Retinal dysplasia has been described in certain breeds such as the Somali, 7 Persian and Norwegian Forest Cat. 8 A link to intrauterine or early neonatal viral infection with feline leukaemia virus (FeLV) has also been documented. 9
The hallmark of retinal dysplasia is the presence of retinal folds or rosettes, resulting from abnormal retinal development. These appear as hyporeflective linear or oval lesions at the tapetal fundus (Figure 9).
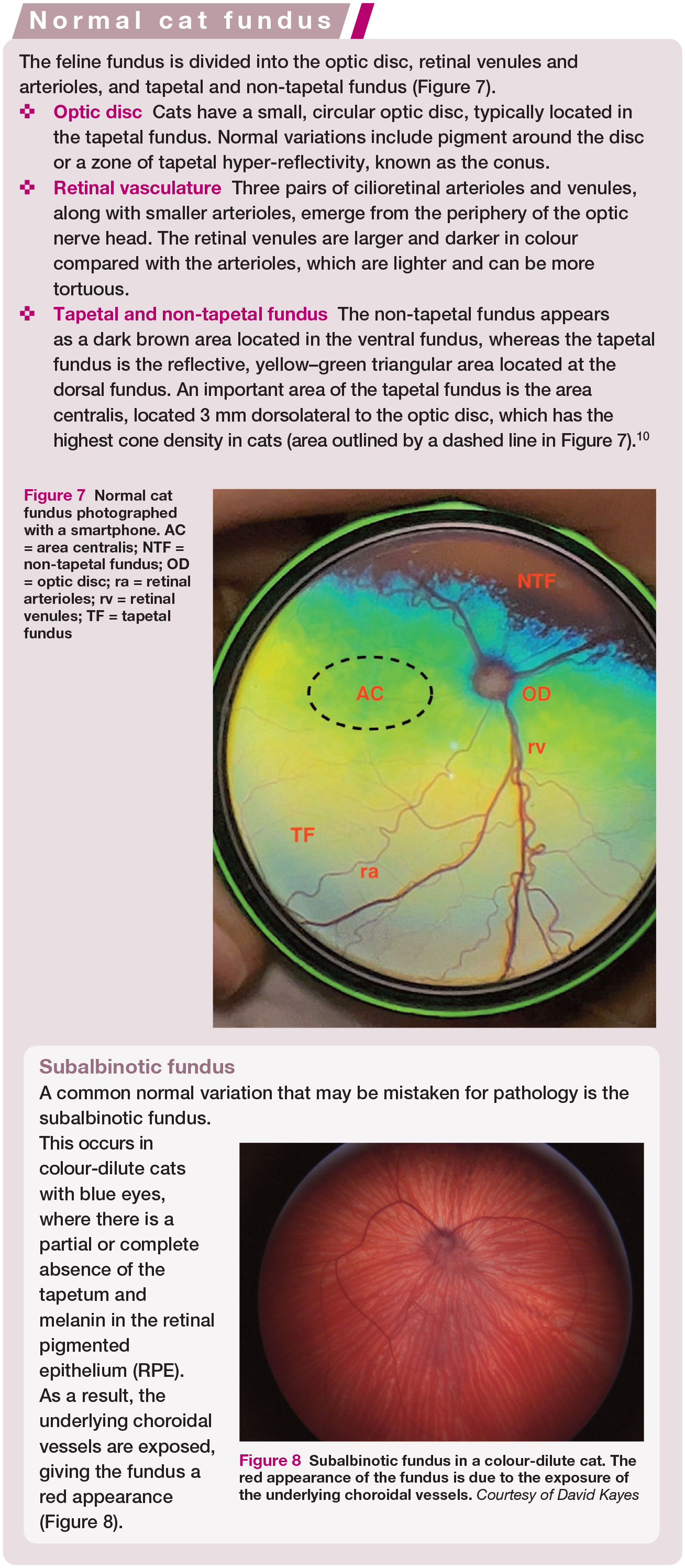

Normal cat fundus photographed with a smartphone. AC = area centralis; NTF = non-tapetal fundus; OD = optic disc; ra = retinal arterioles; rv = retinal venules; TF = tapetal fundus

Subalbinotic fundus in a colour-dilute cat. The red appearance of the fundus is due to the exposure of the underlying choroidal vessels. Courtesy of David Kayes

(a,b) Presence of retinal folds in a cat suspected to have retinal dysplasia
Retinal degeneration
Progressive retinal atrophy and inherited retinal diseases, such as rod-cone dysplasia and rod-cone dystrophy, are infrequently reported in purebred breeds such as the Bengal, Abyssinian and Somali.11,12 Other causes of retinal degeneration include taurine deficiency and enrofloxacin toxicity.
On fundoscopy, there are various degrees of tapetal hyper-reflectivity due to retinal thinning, in addition to retinal vascular attenuation (Figure 10a). In advanced cases, the retinal vasculature is entirely absent and the optic disc appears small and dark, indicating atrophy (Figure 10b).

(a) Early stage of retinal degeneration with focal tapetal hyper-reflectivity (asterisk) and retinal blood vessel attenuation. (b) Advanced retinal degeneration with absence of retinal vasculature, diffusely hyper-reflective tapetal fundus and a small dark optic disc. Note the red appearance of the non-tapetal fundus (subalbinotic variation). Images courtesy of David Kayes
Feline central retinal degeneration (FCRD)
FCRD is caused by a deficiency of taurine, which is an essential amino acid for retinal and cardiac function. 13 Cats have a limited ability to synthesise taurine and require dietary supplementation. While deficiency has become less common due to commercial cat foods enriched with taurine, it can still occur in cats fed non-commercial diets 14 or those with impaired taurine absorption.
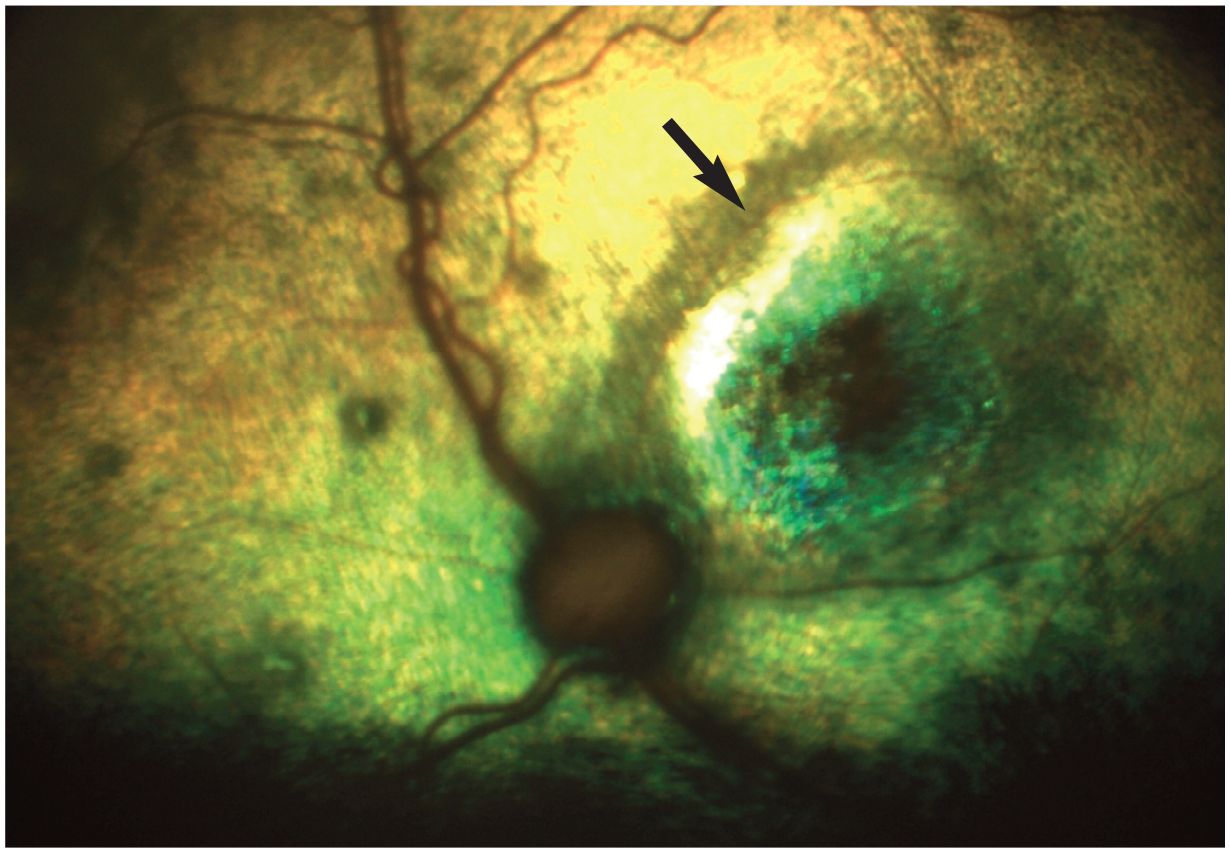
The lesions on fundoscopy are bilaterally symmetrical and initially affect the area centralis. Early clinical signs include granularity of the tapetum at the area centralis, followed by the appearance of an ellipsoid hyper-reflective lesion lateral to the optic disc (Figure 11). As the deficiency progresses, a second similar lesion appears medial to the optic disc and the two lesions eventually coalesce. Generalised retinal degeneration with diffuse tapetal hyper-reflectivity and attenuation of the retinal blood vessels follows. 15

Characteristic oval-shaped hyper-reflective lesion (arrow) in the area centralis secondary to taurine deficiency
Tapetal changes typically develop within 3 to 7 months, with complete retinal degeneration occurring by 9 months of deficiency. 16 Although vision and retinal function may improve after taurine supplementation, the fundic lesions are permanent. 17 Detection of these lesions should prompt measurement of taurine plasma levels and also cardiac evaluation as FCRD can be linked with dilated cardiomyopathy. 18
FCRD is usually an incidental finding, unless the disease is advanced. In such cases, dietary history should be reviewed, and taurine plasma levels should be assessed.
Enrofloxacin-related retinal toxicity
Enrofloxacin has been historically associated with acute and severe retinal degeneration in cats due to a defect in a transport protein in the blood-retinal barrier, which allows accumulation of photoreactive fluoroquinolones and causes retinal damage. 19
Risk factors include older cats with compromised renal/hepatic function, high doses (over 2.5 mg/kg q12h) and intravenous administration. 20 The onset of the toxicity is rapid, with retinal degeneration evident within days after administration and even after a single dose.
On fundoscopy, there is severe and diffuse tapetal hyper-reflectivity, in addition to marked retinal blood vessel attenuation. The retinal changes and blindness are permanent, even after discontinuing the drug.
To prevent such outcomes, fluoroquinolone use in cats should be avoided whenever possible, opting for safer alternatives. If the use of a fluoroquinolone is deemed necessary, the lowest effective dose should be used for the shortest possible duration. While pradofloxacin has shown no retinal toxicity in young, healthy cats, 20 all fluoroquinolones should be regarded as potentially retinotoxic. 21
Changes due to systemic hypertension (SHP)
SHP in cats is defined as a persistent systolic blood pressure above 160 mmHg on repeated measurements taken on more than two occasions. 22 It is most commonly associated with chronic kidney disease and hyperthyroidism. A systolic blood pressure above 180 mmHg is linked to target organ damage 23 and the eye is susceptible to damage from SHP due to its small-calibre blood vessels. SHP is frequently seen in cats over 10 years of age, with acute-onset blindness being the most common clinical presentation (Figure 12), 24 which then prompts blood pressure measurement.
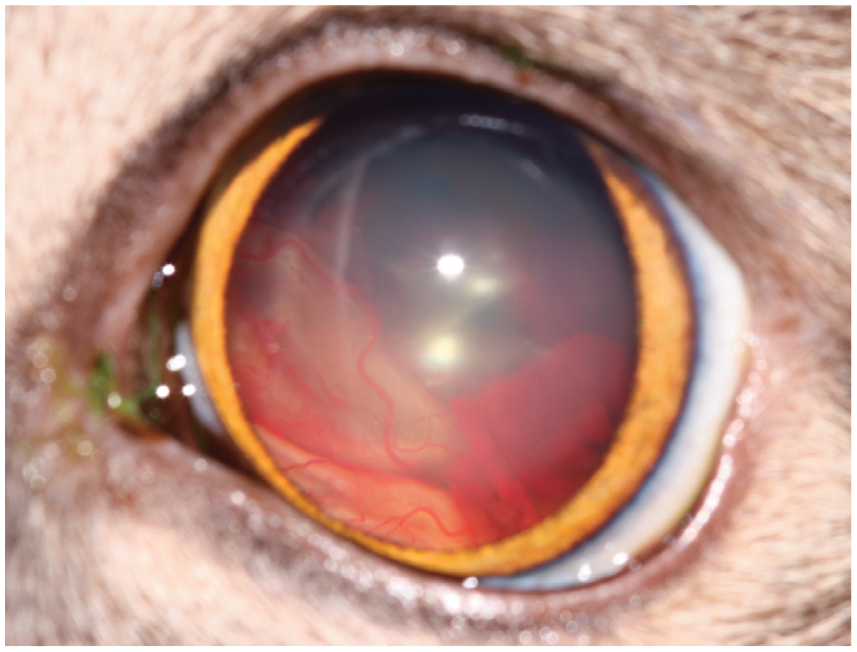
Photo of a cat that presented with acute-onset blindness. Retinal detachment and vitreal haemorrhage are visible
SHP affects the retina through three mechanisms:23,25
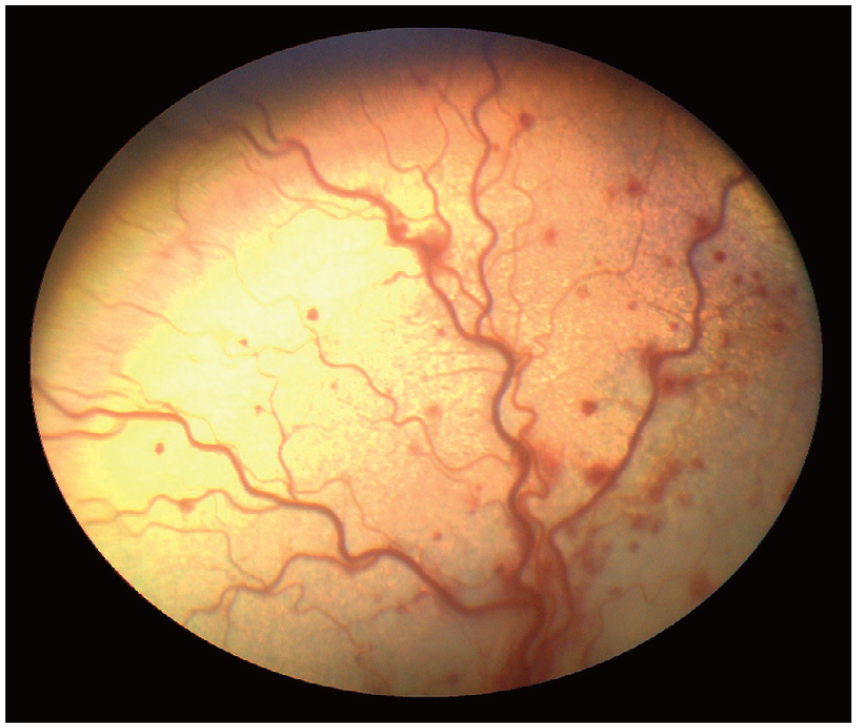
✜ Retinal arteriole constriction due to autoregulatory responses leads to ischemic necrosis, vessel wall rupture and increased permeability, causing leakage of blood. On fundoscopy, this manifests as retinal arteriole narrowing (beading), increased tortuosity, retinal oedema, haemorrhages and macroaneurysms (Figures 13 and 14). This condition is termed hypertensive retinopathy.
Retinal blood vessel tortuosity and retinal haemorrhages in the tapetal fundus of a cat with hypertensive retinopathy

A macroaneurysm (arrow) is visible on a retinal arteriole in the fundus of a cat with hypertensive retinopathy
✜ Choroidal vascular changes lead to accumulation of subretinal fluid and partial or complete retinal detachment. This appears as single or multiple bullous retinal detachments, sometimes involving the entire retina, along with degenerative lesions in the RPE. This is termed hypertensive choroidopathy (Figure 15).
✜ Ischaemia of the optic nerve leads to papilloedema and ultimately to optic atrophy.

Multiple bullous retinal detachments in a cat with hypertensive choroidopathy

This is termed hypertensive optic neuropathy and it is a less common fundic manifestation of SHP.
Early detection of fundic lesions associated with SHP is crucial to prevent blindness, as cats with milder fundic abnormalities at diagnosis have a better long-term prognosis for vision. Fundoscopy should therefore be part of the routine health screening of older cats.
Cats with severe fundic abnormalities may show initial improvement with retinal reattachment and absorption of haemorrhages; however, long-term prognosis for vision is poor due to secondary retinal degeneration (Figure 16). Fundoscopy should be performed alongside blood pressure measurement at rechecks, after initiation of antihypertensive therapy.

Multifocal retinal degeneration with areas of tapetal hyper-reflectivity (arrows) at the sites of previous bullous detachments
Chorioretinitis
Systemic diseases often manifest in the feline fundus in the form of chorioretinitis, which results from inflammation in the choriocapillaris and disruption of the blood-retinal barrier.
Understanding the distinction between active and inactive chorioretinitis lesions is crucial in diagnosis and disease progression assessment. The key differences between active and inactive chorioretinitis lesions are outlined in the box.
Common systemic diseases with fundic manifestations include viral, fungal, protozoal and bacterial diseases.


Active chorioretinitis with retinal haemorrhages, inflammatory infiltrates (black asterisk) and retinal detachment (white asterisk). Courtesy of David Kayes
Inactive chorioretinitis with focal areas of tapetal hyper-reflectivity and pigment disturbances (arrow)
Viral chorioretinitis
Feline infectious peritonitis
FIP is the most common cause of viral chorioretinitis in cats, and ocular signs are sometimes the first clinical indication of the disease. 26 Ocular lesions are more frequently observed with the non-effusive (dry) form of FIP. 27
Bilateral chorioretinitis with perivascular cuffing is the most common finding on fundoscopy. Perivascular cuffing appears as pyogranulomatous exudates surrounding the retinal blood vessels. 28 It is caused by the deposition of macrophages containing the FIP virus in the endothelium of small blood vessels, leading to inflammation and damage to vascular structures. The resulting vasculitis leads to bullous partial retinal detachments. Optic neuritis has also been reported in cases where the central nervous system (CNS) is affected, seen as a swollen, hyperaemic optic disc with blurred margins. 29
Early identification of fundic abnormalities can help lead to a timely diagnosis and management of FIP.
Feline leukaemia virus and feline immunodeficiency virus (FIV)
Retinal abnormalities are uncommon in cats with FeLV and FIV. FeLV has been reported to cause retinal haemorrhages secondarily to severe anaemia in both the tapetal and non-tapetal fundus. 30 FIV has been associated with chorioretinitis lesions due coinfections with other pathogens such as Toxoplasma gondii.
Protozoal chorioretinitis
Toxoplasmosis
T gondii is one of the most commonly implicated pathogens in feline chorioretinitis. Inflammation and tissue damage are caused by both the protozoa and the host inflammatory response.
Granulomatous chorioretinitis and optic neuritis are the most common fundic lesions. Active lesions often appear as multifocal hyporeflective lesions in the tapetal fundus with white fluffy infiltrates in the non-tapetal fundus. 31
Since T gondii is suspected in most cases of feline chorioretinitis, T gondii-specific IgM and IgG titres are routinely performed to confirm diagnosis in the presence of chorioretinitis lesions.
Mycobacterial chorioretinitis
Mycobacterial infections in cats are increasingly recognised, particularly those caused by Mycobacterium bovis and Mycobacterium microti. 32 A notable recent outbreak was linked to contaminated commercial raw diets. 33
Ocular manifestations of systemic mycobacterial disease are seen in 6% of affected cats. 32 Ocular clinical signs are typically unilateral but can also be bilateral.
Fundoscopy findings include granulomatous to pyogranulomatous chorioretinitis, with or without retinal detachment and optic neuritis. 34
Ocular mycobacteriosis can occur without systemic signs, making fundoscopic examination critical in suspect cases.
Mycotic chorioretinitis
Cryptococcosis is the most common systemic mycosis in cats, 35 but other systemic mycoses like blastomycosis, histoplasmosis and coccidioidomycosis may also be encountered, depending on the geographical location.
Fundoscopy findings include granuloma formation in the tapetal or non-tapetal fundus, retinal detachments and optic neuritis if the central nervous system is involved. 35
All cats exhibiting signs suspicious of fungal disease, such as nasal and facial swelling, deep non-healing nasal wounds or nasal polyps should undergo fundoscopic examination to check for retinal lesions.
Neoplastic disease
Primary retinal neoplasia in cats is rare, while secondary neoplasia is more common. One of the most characteristic metastatic retinal lesions in the feline retina are due to carcinomas of the lung and mammary tissue.36,37
The fundic lesions appear as wedge-shaped, tan-to-grey areas radiating from the optic disc in the tapetal fundus. The underlying pathogenesis is thought to involve neoplastic embolisation of the short posterior ciliary arteries, leading to necrosis of the retina and choroid. Intraretinal haemorrhages may also be present.
Optic nerve head lesions
Optic neuritis
Optic neuritis appears to be uncommon in the cat. Inflammation of the optic nerve can be caused by a variety of systemic diseases previously discussed, such as FIP, toxoplasmosis and cryptococcosis. On fundoscopy, the optic disc appears swollen and hyperaemic with blurred margins.
Optic atrophy
Optic atrophy is a common sequela of retinal degeneration but also glaucoma, chronic optic neuritis or trauma (stretching due to proptosis or enucleation of the contralateral globe). The optic disc appears small and dark.

Key Points
✜ The two key methods for examining the fundus are direct and indirect ophthalmoscopy, which are complementary. Indirect ophthalmoscopy is ideal for obtaining a general overview of the fundus, while direct ophthalmoscopy allows for a more detailed inspection of specific lesions.
✜ A thorough, systematic approach is essential to avoid missing lesions. The examination should include assessment of the optic disc, retinal vasculature, tapetal fundus and non-tapetal fundus.
✜ Smartphone fundoscopy is a cost-effective alternative to specialised fundic cameras and it uses video recording to capture clear images. Proper alignment between the camera, condensing lens and pupil is necessary to obtain good images of the fundus.
✜ Systemic diseases such as systemic hypertension and FIP have characteristic fundoscopic lesions. Prompt intervention in such cases can lead to favourable outcomes, both visually and systemically.
Footnotes
Acknowledgements
The authors would like to thank David Kayes, Kris Houston, Kelly Cadman and Lyndsay Kennedy for their assistance obtaining photos for this article.
Supplementary material
The following file is available as supplementary material:
Video 1: Example of a video captured when performing smartphone fundus photography.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors of this commissioned Clinical Spotlight review received an honorarium; as for all JFMS articles, this Clinical Spotlight article went through peer review.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people individually identifiable within this publication, informed consent (verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.