
Abstract
Objectives
Onychectomized cats (Felis catus) with inappropriate elimination behaviors or aggression may be responding to painful paw pathology, even several years after the initial onychectomy. The objectives of this study were to evaluate the onychectomized toes of this population of cats for pain (thorough physical examination and/or buprenorphine trial), pathological changes (using high-resolution radiographs) and response to tenectomy in those with hyperflexion of the proximal interphalangeal joint.
Methods
Cats in this study were previously onychectomized and exhibited inappropriate behaviors (inappropriate elimination, biting), exhibited pain associated with the onychectomy site or had behavioral improvements when put on a 2-week buprenorphine trial. A detailed history was obtained, including verification of proper litter box placement and management. Physical examinations included a close analysis of the onychectomized digits for resistance to extension and pain on palpation. Only cats with a normal urinalysis were included in the study. High-resolution radiographic imaging was performed on all study cats. A total flexor tenectomy was performed on cats with hyperflexion of the proximal interphalangeal joints.
Results
All 42 cats included in the study benefited from total flexor tenectomy surgery. Two cats remained biters, even after a long course of analgesic medication. All cats walked more comfortably post-tenectomy surgery.
Conclusions and relevance
Onychectomy can lead to pain, inappropriate elimination and aggressive behavior. The presented salvage tenectomy procedure can alleviate or eliminate inappropriate behaviors by reducing the pain from the original onychectomy.
Introduction
Cats have become very popular pets; in the USA, they outnumber dogs. 1 For some owners, the cat’s natural scratching behavior is objectionable, and onychectomy appeared to be a quick fix. The first mention of feline onychectomy was in 1952 in a letter to the editor of the Journal of the American Veterinary Medical Association (JAVMA), which stated that the procedure saved a cat’s life. 2 There was also a live television demonstration of the declaw procedure. 3 In 1961, another letter to the editor of JAVMA noted in more detail the declaw procedure. 4 Currently, onychectomies have become a common feline elective surgical procedure. To our knowledge, no peer-reviewed postoperative study was ever presented in the veterinary literature to prove that third phalanx (P3) amputation was safe in the short or long term. An appreciation for the normal mechanics of the cat’s digits explains the resultant pathological changes that occur when the clawed P3 is removed. In the wild, cats need their claws to capture prey to survive. Unique, off-center distal interphalangeal (DIP) joint (claw joint) surfaces allow the P3 to slide to the lateral side of the second phalanx (P2), permitting DIP joint overextension (ie, claw retraction). This joint position is passively maintained throughout daily routine activities primarily by a single short dorsal elastic ligament (Figure 1). There is little capability or need for digital extensors to act on this already overly extended joint in cats. When required, claws can become exposed (protracted) through flexion of the DIP joint; contraction of the deep digital flexor muscle is the prime mover for this action. However, the concurrent contraction of digital extensor muscles is required to ‘stiffen’ the dorsum of the manus and thereby facilitate the action of the deep digital flexor muscle (Figure 1a).

Drawing of the left digit and metacarpal bone, lateral view. (Drawing is representative of digits II–V.) (a) Normal anatomy of bone, tendon and ligamentous structures of interest; extensors are located dorsally and the flexors palmarly. (b) Distal phalanx removed, hyperflexion of the proximal interphalangeal joint. Bones: distal phalanx (P3, red); middle phalanx (P2, yellow); proximal phalanx (P1, green); metacarpal bone (blue). Joints: distal interphalangeal (DIP) joint, proximal interphalangeal (PIP) joint and metacarpophalangeal (McP) joint. Tendons: superficial digital flexor (blue); deep digital flexor (red) with vinculum (black arrow); digital extensors (thick gray line); distal portion of digital extensors (composite tendon; thin gray line). Ligaments: long dorsal elastic ligaments (a, dotted lines); short dorsal elastic ligament (b, white ligament); proximal digital annular ligament (c). Note: the distal digital annular ligament is not drawn in; it is weak and may be absent; the direction of movement of P2 (blue dashed arrow) results in hyperflexion of the PIP joint
Amputation of P3 entails the transection of ligamentous and tendinous structures that span across the DIP joint, for example, the dorsal elastic ligaments, digital extensor tendons and the deep digital flexor tendon (DDFT; Figure 1b). Notably, the DDFT has an often-overlooked attachment to the palmar aspect of the head (distal end) of P2, 5 referred to as a vinculum 6 or accessory ligament. 7 This connection is designed to allow vessels and nerves to traverse between tendon and bone. 8 The vinculum would be expected to remain after an onychectomy. Therefore, in this post-onychectomy scenario, the freely movable middle phalanx (P2) can be pulled palmarly with each deep digital flexor muscle contraction because of the attachment of the vinculum to the distal P2. The likely result is further flexion (hyperflexion) of the (normally flexed) proximal interphalangeal (PIP) joint. The most common radiographic finding in cats’ paws with complications following onychectomy is residual/retained P3 fragments. This is often reported as a complication following the use of a Resco nail trimmer and is less commonly identified following onychectomy procedures performed with a scalpel or a surgical laser. Nail regrowth has also been reported in some cases of retained fragments.
Materials and methods
Onychectomized cats were sourced from private cat owners, feline sanctuaries and feline rescues; many of the study’s rescue cats were failed adoptions. These cats had some manifestation of undesirable behavior (eg, inappropriate elimination and/or aggression). Prior to inclusion in the study, proper litter box placement and management were in place to eliminate these factors as a cause for the inappropriate elimination behavior. 9 Physical examination, urinalysis (UA) and radiographic changes of the amputated digits were all considered to help localize the cause of the inappropriate behavior.
The physical examination included a detailed look at the digital pads for callus, manipulation of the digits to assess for resistance to extension and deep palpation for signs of pain. If pain could not be localized to the amputated digits with certainty, or if the owner was hesitant to proceed with surgical treatment, then a standardized 2-week buprenorphine trial was planned to determine whether the administration of pain relief would alleviate some inappropriate behaviors. Oral buprenorphine HCl 0.3 mg/ml was sourced from Atlas Pharmaceutical (a 503B drug compounder/manufacturer) and dosed at 0.25 ml/10 lb (4.54 kg) body weight, delivered transbuccally twice daily. Owners were instructed on this method of administration and cautioned that swallowing the medication would lead to its inactivation. If the cat started using the litter box or was less aggressive during this trial, the test was considered positive (ie, non-specific pain contributed to the manifestation of inappropriate behavior). The buprenorphine trial was not implemented if, on examination, manipulation of the digits was painful or the owner consented to the experimental surgery without the trial. The buprenorphine trial was an additional step to help determine the need for total flexor tenectomy (TFT) surgery. The only change occurring to the trial cats was the surgery. Their preoperative behavior was compared with their postoperative behavior.
UA was performed to rule out infection or inflammation of the bladder as the cause of the inappropriate elimination behavior. UA was performed with a VetScan UA (Zoetis) reader and VetScan UA14 urine test strips. The 14 parameters tested by the strip included microalbumin, pH and protein; leukocytes and urine specific gravity (USG) were disregarded and tested as follows. USG was measured with an HSK-Vet refractometer (Heska). Complete UA included a centrifuged sediment analysis performed with an Olympus CX41 microscope by the clinic’s certified veterinary technician. The presence of leukocytes and red blood cells (RBCs; ± bacteria) indicated a urinary tract infection, and was treated as such. Probable interstitial cystitis was diagnosed only when RBCs were present in a large quantity. Crystals with elevated pH and concentrated urine (USG >1.035) were diagnosed as crystalluria with probable cystitis. All cats were required to attain a normal UA to enter the study.
Digital radiographs of the forepaws were made to assess P3 fragments, P3 fragments with claw regrowth, indications of DDFT/vinculum tendonitis, distal P2 inflammation, distal P2 osteochondritis and PIP joint hyperflexion (<90°). Lateral and medial dorsopalmar oblique images with an angle of 45° were obtained using Progeny Imaging Software 2.0 with a Progeny DR Digital Dental Sensor, and an AFP Imaging Image-Vet 70 Plus dental X-ray machine was used to obtain high-resolution images for radiographic paw pathology analysis. Triadan dental charting was used to identify the radiological paw views generated in Progeny. The 45° oblique angle gives a more ventral view for detection of fragment presence and joint and tendon status (Figures 2 and 3). It is much easier to evaluate claw regrowth and/or fragment infection with an oblique paw radiograph (Figures 4 and 5) because a standard tabletop AP radiograph, with flexor contraction present, is looking down on a perpendicular P2. This makes a diagnosis of the P2 condition challenging. The lateral tabletop radiographic view can result in digit overlay, making the individual digits hard to differentiate. Hyperflexed PIP joint changes indicated the need for a flexor tenectomy to relieve the hyperflexion. Because of the financial cost of fragment removal and the challenging surgery needed to remove the P3 fragment(s), it was determined that if a P3 fragment was not regrowing a claw, a TFT could be performed instead of fragment removal. The rationale was that the more plantigrade stance after the tenectomy would result in the cat no longer walking directly on that P3 fragment. The P3 fragment should be removed to avoid further claw regrowth or fragment infection. Detailed instructions for P3 fragment removal have been published by Martell-Moran. 10

Lateral dorsopalmar oblique radiograph of the normal left paw. SDFT = superficial digital flexor tendon; DDFT = deep digital flexor tendon; P2 = second phalanx; P3 = third phalanx

Medial dorsopalmar oblique radiograph of the normal left paw. P1 = first phalanx; P2 = second phalanx; P3 = third phalanx

Lateral dorsopalmar oblique radiograph of an onychectomized left paw. SDFT = superficial digital flexor tendon. P1 = first phalanx; P2 = second phalanx; P3 = third phalanx

Medial dorsopalmar oblique radiograph of an onychectomized left paw
Surgical intervention for onychectomy pain relief
One of our goals was to shift the cat’s weight on to the main (metacarpal) pad to create a plantigrade stance and provide a cushion for the amputated toes rather than the natural digitigrade stance that would direct the amputated digit toward the ground.
The following describes the salvage operation. Premedication, including acepromazine/butorphanol, was given intramuscularly 10 mins before masking with isoflurane. A cuffed endotracheal tube was placed. A Terumo 24 G intravenous (IV) catheter was placed in the femoral vein and lactated Ringer’s solution maintenance flow was started on an IV pump. Clip and surgical preparation of paws were performed using an Oster trimmer clipper with a ¼ inch blade. Under anesthesia, the digital hyperflexion was confirmed before proceeding with the surgery. A four-point paw block was placed. 11 Buprenorphine and maropitant citrate (Cerenia) were given subcutaneously at the start of the surgery. The patient was placed in dorsal recumbency. A Nye tourniquet was placed for no more than 10 mins at the mid-humeral region. A palmar sagittal skin incision was made over phalanx 1 (P1) with a No 11 scalpel blade (Figure 6). The superficial and deep digital flexor tendons were elevated with a root tip extractor (Figure 7). A straight mosquito forceps was applied to the tendons (Figure 8), and a 3 mm tendon segment was removed (Figure 9). A radio scalpel was used to accurately excise the tendon segments on both sides of the forceps. The skin wounds were cleaned and dried. Using the provided applicator tip, GLUture (Zoetis) was carefully placed on the skin edges, which were gently held in apposition until the tissue adhesive was set (Figure 10). All cats recovered smoothly. No paw shaking was observed. Postoperative pain medication, oral buprenorphine (20 µg/kg 2–3 times daily transbuccally) or robenacoxib (Onsior, Elanco; 1 mg/kg once daily) and amoxicillin 11–22 mg/kg (once daily) were dispensed. Bed or cage rest was mandatory for a minimum of 10 days. Fine, scoopable litter was recommended.

Skin incision over phalanx 1 exposing the digital flexor tendons (palmar view). *McP metacarpophalangeal joint

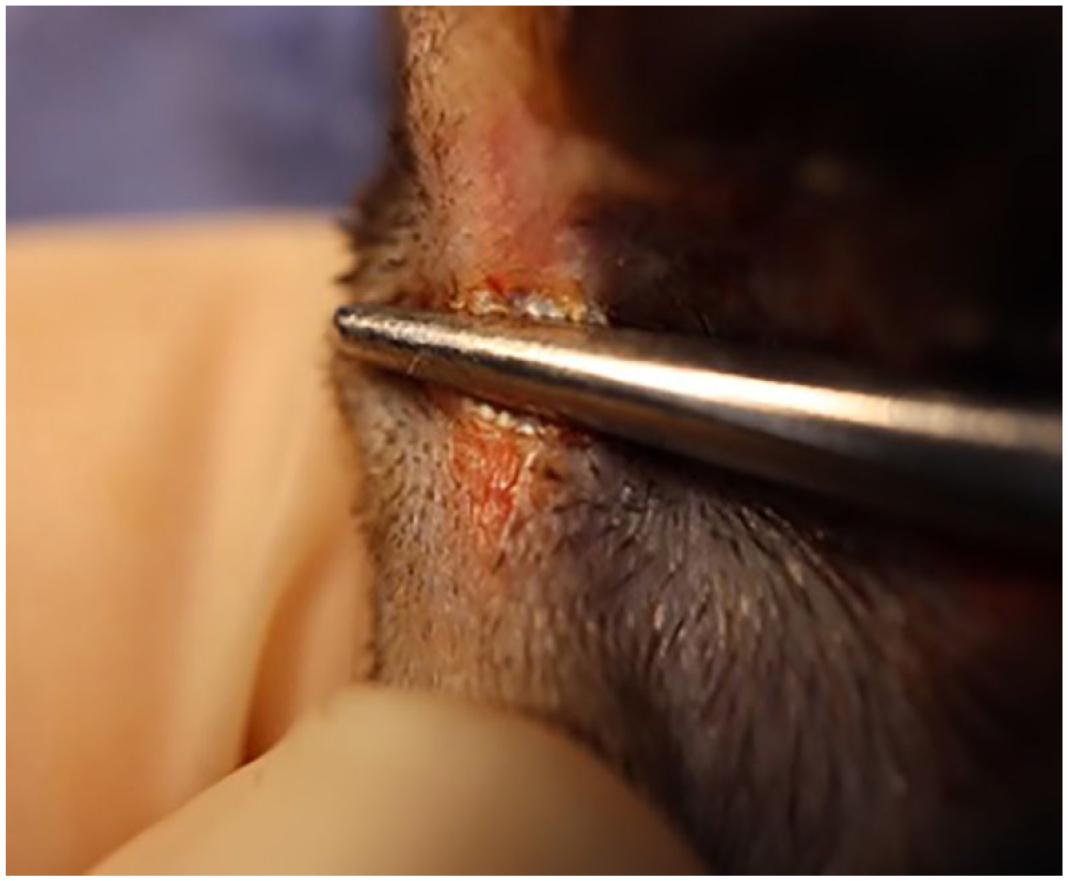
Elevated digital flexor tendons
Placement of mosquito forceps on the flexor tendons

Removal of a 3 mm segment of the digital flexor tendons

Wound closure and full-digit extension confirmation
Results
All cats in this study were previously onychectomized and presented with a history of inappropriate behavior (predominantly inappropriate elimination and/or aggression). Cats entering the study had proper litter box placement/management (see Carney et al 9 ) and a routine UA to rule out these variables as a cause of the inappropriate behaviors. In the majority of the study cats, pain could be localized to the digits with the physical examination. In others, a reason for the inappropriate behaviors could not be determined through physical examination and paw radiography. In this case, the diagnostic buprenorphine (pain relief) trial was used to determine if behavioral issues were related to non-specific pain; 43% (n = 18) of the cats underwent this trial and 89% (n = 16) of these cats had a positive response (ie, they used the litterbox appropriately and/or showed less aggression).
Detailed digital radiographs provided evidence of the tissue changes associated with the onychectomy. Forty-two cats with an average age of 8.6 years (range 5–12.2) had a total flexor tenectomy on digits II–V. All cats except one attained complete extension of these digits. The one exception, the first cat in the study, could not extend some of digits II–V. After a repeat of the tenectomy to transect any remaining tendon, the cat remained at its preoperative level of aggression. Another cat had P2 hyperflexion persist after a complete tenectomy. Possibly caused by PIP joint remodeling, digit V in both front paws could not be fully extended; however, the cat displayed more comfortable walking. Twenty-six cats that had TFT had P3 fragments present. Forty cats had a positive outcome following the salvage surgery and two had the same clinical signs as pre-salvage. This represents a 95.2% success rate for the TFT surgery. All of the cats walked more comfortably and all owners were satisfied with the surgical outcome, even though the cats became flat-footed. One of the concerns was carpal hyperextension (breakdown) following surgery, but this was not observed. The first study cat that received the TFT was monitored for 6 years. It had long, slender legs, small paws and a disproportionately large upper body. No carpal ligament degeneration resulting in hyperextension was observed. None of the cats that had TFT needed long-term pain relief to use their litter boxes following the salvage surgery.
Discussion
Many post-onychectomy complications have been documented.12,13 Research has shown increased inappropriate behavior in onychectomized cats, which has been attributed to back, hip and paw pain. 14
Amputation of the distal portion of the digit removes the claw and destroys the balance of the remaining portions of the limb. The pressure plate gait analysis lacks the resolution to determine an onychectomized cat’s gait change. The graph documenting the results of pressure plate gait analysis, with a high top-end y-axis value, effectively diluted the statistical difference between onychectomized and non-onychectomized cats. 15 Waldron has described various onychectomy techniques. 16 The guillotine (nail trimmer) method is prone to leaving behind a fragment of P3, which can anchor the DDFT to the ventral P3 DDFT insertion (flexure tubercle), leading to hyperflexion of the PIP joint. The DDFT in isolation can pull the distal end of P2 palmarly (via the vinculum), resulting in pain as the end of P2 is driven into the pads of the digits. Therefore, with or without a P3 fragment, the result can bring the normally flexed PIP joint into hyperflexion. Note that the PIP joint is routinely flexed; further flexion of this joint can result in hyperflexion. Owing to the complications of the guillotine technique, at least one veterinary medical board does not consider its use to be the current standard of care.16,17 The surgical removal of P3 fragments has been described in the literature and appears superior with regard to reducing the chance of claw regrowth. However, following P3 fragment removal, cats must be monitored for subsequent hyperflexion.
In the current study, radiographic evidence of identified complications in post-onychectomy cats included retained P3 fragments, some of which are more proximally displaced because these are attached to a contracted tendon. Punctate subchondral lucent areas on the distal P2 articular surface may be due to cartilage devitalization, ischemia and trauma, followed by articular cartilage eburnation; a similar process is described for degenerative osteochondrosis. Other radiographic differential diagnoses for these focal lucent areas are processes similar to subchondral bone cysts, focal vasculitis, focal ischemia or, possibly, focally invasive osteomyelitis. It was beyond the scope of this study to identify the cause of these distal P2 radiographic changes. The cats with a P3 fragment did very well after TFT without P3 fragment removal. Cat rescues and other rehoming organizations will find the TFT to be cheaper and easier to perform than P3 fragment removal. There is some risk that hyperflexion will occur after fragment-removal surgery. Other radiographic findings included dystrophic tendon calcification and bone remodeling at the tendon insertion sites due to altered mechanical stresses. Osteopenia may be the result of disuse bone atrophy. Digital contracture is a sequela of dystrophic and degenerative changes in the soft tissue support structures of the paw, including the distal digits, such that misalignment of the digits disrupts the normal distribution of mechanical forces and stimuli that would normally maintain an active range of motion, digital elasticity and flexibility, and facilitate normal weight-bearing in the paws. The TFT has been used successfully in at least two other studies with a very limited number of cats.18,19 All the cats within this current study manifested clinical signs that were suspected to be a result of onychectomy pain.
Conclusions
Onychectomy has never been researched for short- or long-term side effects. Digital dental sensor images and careful, focused paw examinations have revealed the damage done over time and the pain this procedure can cause onychectomized cats. The TFT can be performed on non-regrowth fragment and no-fragment hyperflexed cats; however, it does leave the cat flat-footed. This must be made clear to the cat’s owner. The standard of veterinary care is dynamic and forever changing. 16 The onychectomized cat may be thought to have an iatrogenic potentially painful disease condition, which should be included in the differential list for inappropriate elimination, and aggressive behavior. In this study, it was shown that inappropriate elimination and possibly aggression, apparently caused by the pain from the original onychectomy, can be alleviated or eliminated with TFT.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.