
Abstract
Objectives
The aim of this study was to compare indications, complications and mortality rates for perineal urethrostomy (PU), transpelvic urethrostomy (TPU) and prepubic urethrostomy (PPU).
Methods
A retrospective review of, and follow-up owner questionnaire for, cats undergoing urethrostomy between 2008 and 2018, at a single referral hospital, were performed.
Results
Fifty-six cats underwent urethrostomy (PU, n = 37; TPU, n = 8; PPU, n = 11). The presenting problem was significantly associated with urethrostomy technique (P <0.001). For PU cats, feline idiopathic cystitis (FIC; n = 21 [56.7%]) was the most common problem, whereas for PPU cats, trauma (n = 9 [81.8%]) was most common (P <0.001). Urethrostomy technique was associated with imaging diagnosis (P <0.001) of the urethral lesion. Most PU cats had no diagnostic imaging lesion (n = 15 [40.5%]) or obstructive calculi or clots (n = 10 [27.0%]), and all PPU cats had urethral rupture. Ten (90.9%) PPU cats had a pelvic lesion, while 21 (56.7%) PU cats had a penile lesion. TPU cats had a range of presenting problems and imaging diagnoses. Short- and long-term complications were reported in 33/55 (60.0%) and 11/30 (36.7%) cats, respectively. The number of cats with long-term complications was greater among PPU cats (P = 0.02). Short-term dermatitis (P = 0.019) and long-term incontinence (P = 0.01) were associated with PPU. Short-term mortality was 5.6% and long-term mortality was 13.3%; both were independent of urethrostomy technique. Quality of life post-urethrostomy, across all techniques, was graded as good by 93% of owners.
Conclusions and relevance
In this study, PU was the most common feline urethrostomy technique indicated for FIC. Short-term urethrostomy complications are common, irrespective of urethrostomy technique. Long-term complications are less frequent but more common with PPU.
Introduction
Feline perineal urethrostomy (PU) is a salvage procedure that makes the narrow distal penile urethra redundant, by creating a permanent urethral opening between the wider, more proximal, pelvic urethra and the perineal skin. Its primary indication is for male cats with recurrent urethral obstruction due to feline idiopathic cystitis (FIC) that cannot be managed by urethral flushing and catheterisation. 1 Reported complication rates are 13–25% and 20–42% in the short and long term, respectively, with mortality rates of up to 24%. 2
Feline prepubic urethrostomy (PPU) has been described as a technique to deal with a failed PU, irreparable injury of the intrapelvic urethra or congenital narrowing of the intrapelvic urethra. 3 In this surgery the pelvic urethra is transected as far caudally as possible, but proximal to the site of injury and sutured to the skin of the ventral midline, just cranial to the pubis. 3 Complication rates of up to 83.3% and mortality rates of up to 38% are reported, which appear to exceed those of PU.4,5
Owing to the apparently high complication rate associated with PPU vs PU, transpelvic urethrostomy (TPU) has been described as an alternative technique for cats with failed PU. 6 In this procedure the caudal intrapelvic urethra is accessed by making a window in the pubis. The urethrostomy is then created between the exposed intrapelvic urethra and overlying skin. A single study of 11 cats reported a complication rate of 36%, with no mortality. 6
In summary, based on the reported complication and mortality rates for each technique, preservation of the longest length of urethra possible according to the underlying disease process is recommended. Accordingly, PU would be preferred over TPU, which, in turn, would be preferred over PPU. To our knowledge, no studies have directly compared the three feline urethrostomy techniques. The purpose of the current study was to perform a retrospective review of feline urethrostomy procedures at a single referral centre, in order to directly compare the indications, complications and mortality rates of PU, PPU and TPU. Our null hypothesis was that when used for the appropriate indication, the outcome for each of these techniques would be the same, when outcome was assessed according to complication rates, mortality and owner satisfaction.
Materials and methods
Cats undergoing urethrostomy, between January 2008 and November 2018, at a single referral hospital were identified and retrospectively reviewed by searching computerised clinical records. Data recorded for each cat included signalment, history and the results of physical examination, clinical pathology and diagnostic imaging. Surgical reports, anaesthesia records and hospitalisation records were reviewed to confirm details of urethrostomy technique, perioperative treatments and postoperative progress. The variables collected are given in Tables 1–7.
Presenting clinical signs demonstrated by 56 cats undergoing urethrostomy

Cats are grouped according to presenting problem. Number (%) of cats with each clinical sign are given
FIC = feline idiopathic cystitis
Summary of abnormal blood test results demonstrated by cats undergoing urethrostomy

Cats are grouped according to presenting problem. Number (%) of cats with each abnormality out of the total number of cats, for which blood tests were available, are given
FIC = feline idiopathic cystitis; PCV = packed cell volume
Diagnostic imaging studies performed in 56 cats undergoing urethrostomy
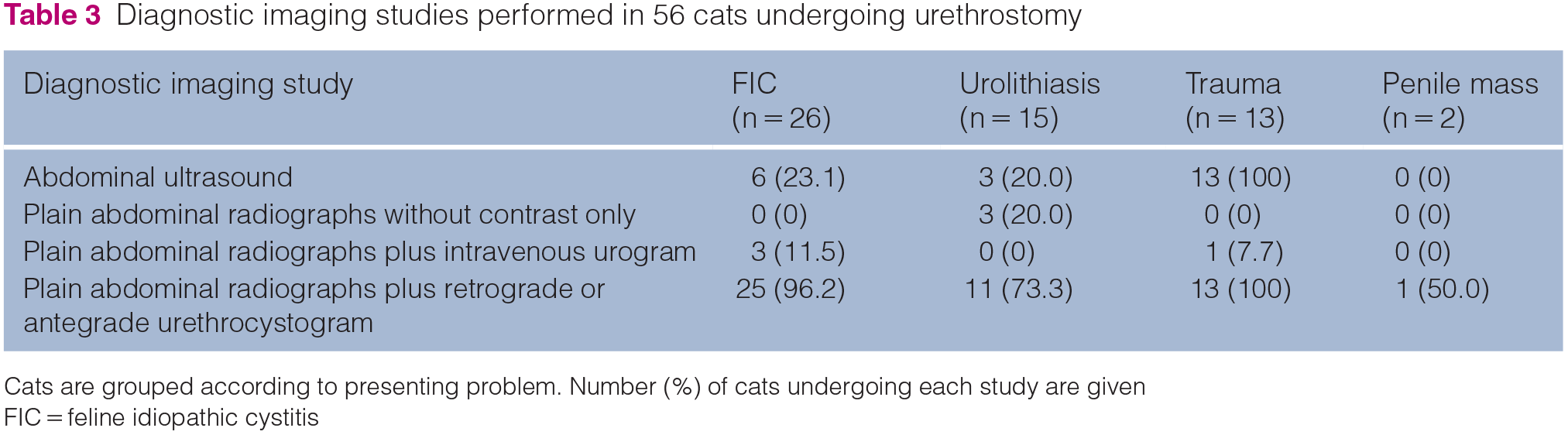
Cats are grouped according to presenting problem. Number (%) of cats undergoing each study are given
FIC = feline idiopathic cystitis
Location of urethral lesion seen on diagnostic imaging studies in 56 cats undergoing urethrostomy

Cats are grouped according to presenting problem. Number (%) of cats undergoing each study are given. P values are given for significant associations between location of urethral lesion and presenting problem
FIC = feline idiopathic cystitis; NS = not significant
Type of urethral lesion seen on diagnostic imaging studies in 56 cats undergoing urethrostomy

Cats are grouped according to presenting problem. Number (%) of cats with each lesion are given. P values are given for significant associations between type of urethral lesion and presenting problem
FIC = feline idiopathic cystitis; NS = not significant
Short-term complications in 55 cats undergoing perineal urethrostomy (PU), transpelvic urethrostomy (TPU) and prepubic urethrostomy (PPU)
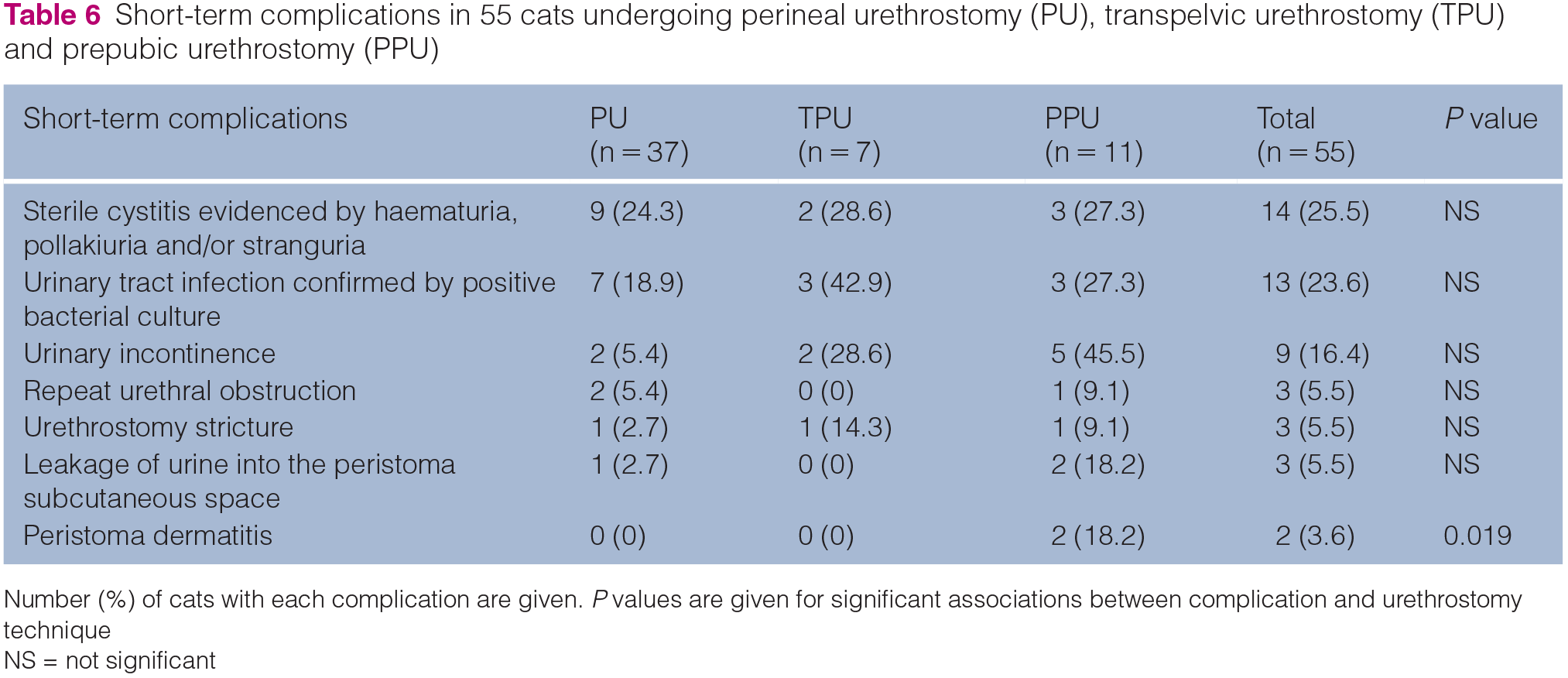
Number (%) of cats with each complication are given. P values are given for significant associations between complication and urethrostomy technique
NS = not significant
Long-term complications in 30 cats undergoing perineal urethrostomy (PU), transpelvic urethrostomy (TPU) and prepubic urethrostomy (PPU)
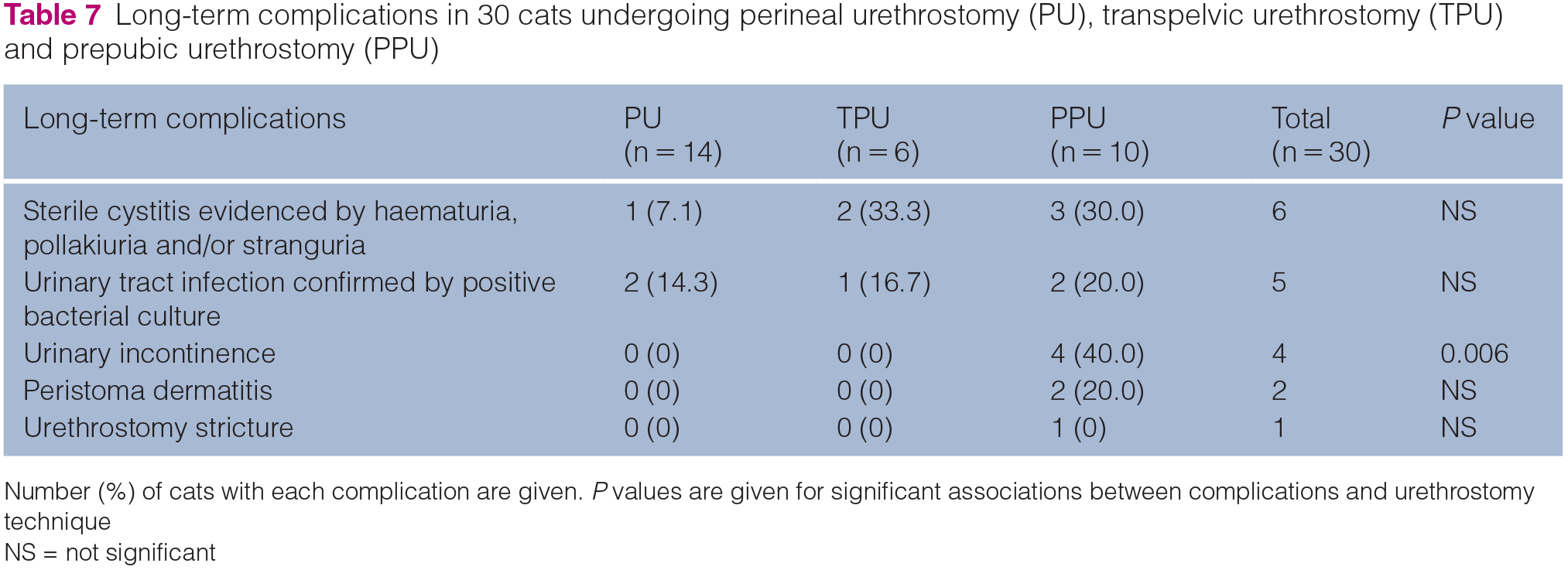
Number (%) of cats with each complication are given. P values are given for significant associations between complications and urethrostomy technique
NS = not significant
A board-certified specialist surgeon performed all of the surgeries, with or without the assistance of a surgical resident. PU, TPU and PPU were performed following the published techniques of Wilson and Harrison, 1 Bernard and Viguier, 6 and Bradley, 3 respectively.
The outcome of urethrostomy was assessed according to complications, mortality and owner satisfaction. Short-term outcome was defined as outcomes recorded in the case records during the first 4 weeks postoperatively. During the study period, suture removal for all urethrostomy surgeries occurred at the referral hospital, 10–14 days after surgery. Moreover, hospitalisation until suture removal was offered to all clients. This allowed detailed monitoring for early complications, which were dealt with by the referral hospital, normally within the first 4 weeks postoperatively. Short-term complications were divided into minor and major complications. Minor complications were defined as those that required no intervention or pharmacological treatments only. Major complications were defined as those that required surgical or other procedural intervention, or that resulted in death or euthanasia.
Long-term outcome was defined as outcomes arising after the first 4 weeks postoperatively. Long-term outcome was therefore less detailed and obtained primarily by means of an owner telephone questionnaire, which was completed at the time this retrospective study was carried out and also by review of the case records. The maximum duration of long-term follow-up was therefore determined by the date of surgery and the date of the telephone questionnaire. The telephone questionnaire is outlined in Table 8. This questionnaire was conducted by telephone, which allowed the interviewer to use appropriate language to ensure understanding of all technical veterinary terms.
Guide for telephone owner questionnaire used to assess long-term follow-up and owner satisfaction

QMHA = Queen Mother Hospital for Animals; UTI = urinary tract infection
Statistical analysis was performed using IBM SPSS Statistics, Version 25 (IBM). Cats were divided into three groups according to urethrostomy technique: PU, TPU and PPU. Data for these three groups were compared graphically and statistically. For continuous variables, the Kruskal–Wallis test, followed by the Dunn’s pairwise test, were used to explore differences between the three groups. For categorical variables, the Pearson χ2 test, followed by the Fisher’s exact test, were used to explore differences between the three groups. Statistical significance was set at P <0.05.
This study was approved by the local social science ethical review board (URN SR2017-1506).
Results
Signalment
Fifty-seven cats underwent urethrostomy between January 2008 and November 2018 at the study hospital. One cat was excluded due to incomplete medical records, leaving 56 study cats. These 56 cats included 37 cats (66.1%) that underwent PU, eight cats (14.3%) that underwent TPU and 11 cats (19.6%) that underwent PPU. Figures 1–3 demonstrate each of the urethrostomies. Fifty-four cats (96.4%) were neutered males and two cats (3.6%) were entire males. Fifty-one cats (91.1%) were domestic shorthair or domestic longhair cats, and five cats (8.9%) were pure breeds. The median age was 5.9 years (range 6 months to 18 years). The median weight was 4.9 kg (range 2.5–8.2 kg). There was no difference among surgical groups with respect to breed, age or body weight.

Photograph of a perineal urethrostomy at suture removal. The cat’s head is to the left of the photograph

Photograph of a transpelvic urethrostomy stoma immediately postoperatively. The cat’s head is to the left of the photograph

Photograph of a prepubic urethrostomy immediately postoperatively. A cystostomy tube is also in place. The cat’s head is to the left of the photograph
Presenting problem, clinical pathology and diagnostic imaging
The primary presenting problems leading to urethrostomy for the 56 study cats included the following: recurrent urethral obstruction due to FIC (n = 26 [46.4%]); urolithiasis (n = 15 [26.8%]); major trauma (n = 13 [23.2%]); an inflammatory penile mass (n = 1 [1.8%]); and a penile adenocarcinoma (n = 1 [1.8%]). Presenting signs are summarised in Table 1. Blood tests results based on those performed on admission to the study hospital or just prior to referral are summarised in Table 2. Of 56 cats, 34 (60.7%) had urine bacterial culture and sensitivity testing performed; 12 (21.4%) had a positive culture recorded before or at the time of surgery; and 23 (41.1%) were prescribed antibiotics empirically or based on culture and sensitivity. Diagnostic imaging studies and findings are summarised in Tables 3–5.
Cats presenting with FIC
The 26 cats with FIC had a median duration of clinical signs prior to urethrostomy of 221.5 days (range 8–1245 days). Prior to referral, 25 (96.2%) cats underwent urethral catheterisation, a median of three times (range 1–7) and 21 (80.8%) cats were prescribed medical management for FIC. After referral, procedures performed prior to urethrostomy included urethral catheterisation in 11 (42.3%) cats; cystostomy tube placement in five (19.2%) cats; bladder rupture repair in one (3.8%) cat; and abdominal drain placement in one (3.8%) cat. In addition, pharmacological treatments for cystitis, including one or more of meloxicam, prazosin and buprenorphine, were initiated in 22 (84.6%) cats. Urethrostomy was performed at a median of 3 days (range 0–43 days) after referral.
Cats presenting with urolithiasis
The 15 cats with urolithiasis had a median duration of clinical signs prior to urethrostomy of 19 days (range 0–1095 days). Prior to referral, all 15 cats underwent urethral catheterisation, a median of two times (range 1–4) and 12 (80%) cats were prescribed medical management for FIC. After referral, procedures performed prior to urethrostomy included urethral catheterisation in three cats (20%) and cystostomy tube placement in four cats (26.7%). In addition, pharmacological treatments for cystitis, including one or more of meloxicam, prazosin and buprenorphine, were initiated in 12 (80%) cats. Urethrostomy was performed at a median of 3 days (range 0–74 days) after referral.
Cats presenting with trauma
For the 13 cats with major trauma, urethrostomy was performed a median of 20 days (range 1–44 days) after the trauma. Concurrent injuries were seen in 11 cats (84.6%), including pelvic fractures, skin wounds, pleural and peri-cardial fluid, and abdominal wall rupture. Treatment prior to urethrostomy included surgical fracture management in two (15.4%) cats, surgical wound management in four (30.8%) cats, cystostomy tube placement in nine (69.2%) cats, urethral catheterisation in five (38.5%) cats, abdominal wall repair plus abdominal drain placement in one (7.7%) cat and pelvic limb amputation in one (7.7%) cat. Urethrostomy was performed at a median of 13 days (range 1–42 days) after referral.
Cats presenting with penile/preputial masses
Two cats presented with a penile/preputial mass. The median duration of clinical signs prior to urethrostomy was 45 days (range 30–60 days). Neither cat had episodes of prior urethral obstruction or cystitis. Biopsy of the lesions revealed a penile adenocarcinoma in one cat and an inflammatory penile lesion in the other. Thoracic and abdominal staging (CT scan) was performed for the cat with penile adenocarcinoma and no metastatic disease was noted. Surgery was performed 1 and 9 days after referral, respectively.
Association between primary presenting problem and urethrostomy technique
A significant association was found between primary presenting problem and urethrostomy technique (P <0.001). Of the 37 PU cats, FIC (n = 21 [56.7%]) was most common, followed by urolithiasis (n = 12 [32.4%]), trauma (n = 2 [5.4%]) and penile mass (n = 2 [5.4%]). Of the 11 cats with PPU, trauma (n = 9 [81.8%]) was most common, with only two (18.2%) FIC cats. TPU cats included a more even range of FIC (n = 3 [37.5%]), trauma (n = 3 [37.5%]) and urolithiasis (n = 2 [25%]).
Association between diagnostic imaging findings and urethrostomy technique
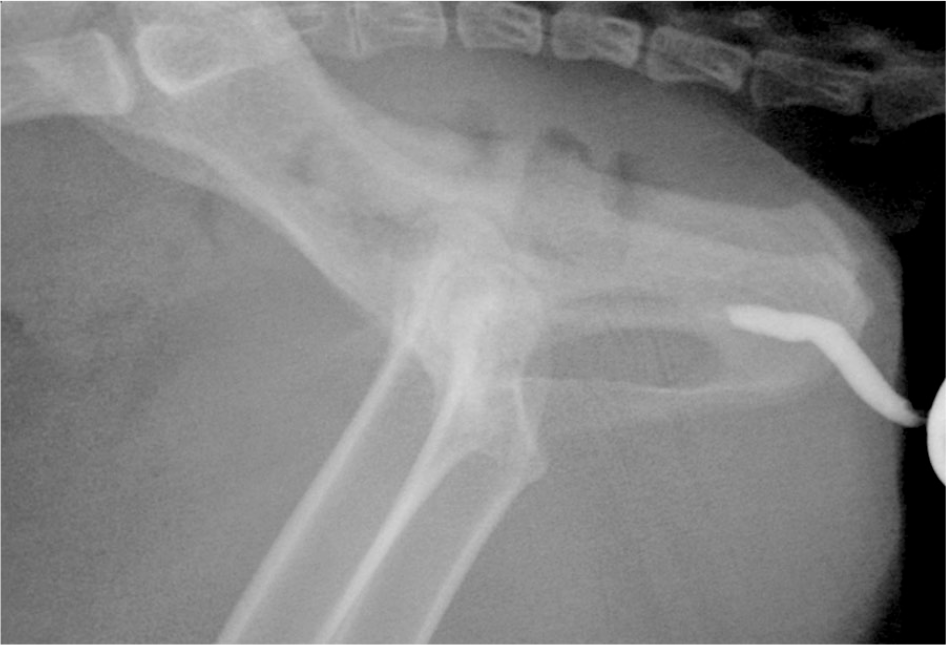
A significant association was found between urethrostomy technique and both the nature (P <0.001) and site (P <0.001) of lesion, as determined by plain radiography and positive contrast retrograde urethrocystography and/or normograde cystourethrography. For this analysis, the penile urethra was defined as the portion of the urethra at or distal to the ischial arch and the pelvic urethra was defined as the portion of the urethra within the pelvis. Figures 4–8 exemplify the range of radiographic lesions and sites of urethral injury. Fifteen (40.5%) PU cats had no lesion, 10 (27%) had calculi or clots, eight (21.6%) had stricture and four (10.8%) had rupture. Conversely, 100% of PPU cats had rupture, with four (36.4%) also having stricture. The TPU cats included the full range of lesions: stricture (n = 4 [50%]), rupture (n = 2 [25%]), stricture plus rupture (n = 1 [12.5%]) and calculi (n = 1 [12.5%]). As expected, all except one (9%) cat with PPU had a pelvic lesion. PU cats included one (2.7%) with a pelvic lesion and 21 (56.7%) with a penile lesion. TPU cats included six (75%) with a penile lesion and two (25%) with a pelvic lesion.

Normal positive contrast retrograde urethrocystogram highlighting contrast filling the entire urethra and entering the bladder

Positive antegrade urethrocystogram highlighting contrast filling of the urethra up to the level of the ischial tuberosity where it stops abruptly, indicating a penile urethral stricture. This cat underwent a perineal urethrostomy

Lateral radiograph of the caudal abdomen and pelvis showing a single radiopaque urolith in the penile urethra. This cat underwent a perineal urethrostomy

Positive contrast retrograde urethrocystogram showing contrast leakage from the intrapelvic urethra at the level of the ischium indicating a urethral rupture at this level. This cat underwent a transpelvic urethrostomy
Positive contrast retrograde urethrocystogram showing an abrupt stop in contrast filling of the urethra within the pelvis indicating a urethral stricture at this level. This cat underwent a prepubic urethrostomy
Surgery
The median surgical times for PU, TPU and PPU were 85 mins (range 35–235 mins), 150 mins (range 60–200 mins) and 150 mins (range 85–270 mins), respectively. Surgical time was significantly shorter for PU compared with TPU (P = 0.034) and PPU (P = 0.019).
Short-term outcome
One TPU cat did not return for suture removal and was lost to follow-up. Short-term complications were reported in 33/55 (60%) cats, including 23/37 (62.2%) PU cats, 4/7 (57.1%) TPU cats and 8/11 (72.7%) PPU cats. There was no association between number of cats with complications and urethrostomy technique. Short-term complications are given in Table 6. The only complication significantly associated with a particular urethrostomy technique was peristomal dermatitis, which was only seen in two (18%) cats with PPU (P = 0.019). No association could be found between incidence of complications and any of the preoperative and operative variables reported in Tables 1–5.
Sterile cystitis was left untreated in 6/14 (42.9%) cats as clinical signs were mild or self-resolving. Eight of 14 (57.1%) cats were treated with a combination of drugs for the management of FIC (meloxicam and/or prazosin). Urinary tract infections (UTIs) were treated with anti-biotics according to culture and sensitivity, with no further follow-up performed. Urinary incontinence was managed by skin care as for peristomal dermatitis below.
Urethral obstruction was reported in two cats with PU and one cat with PPU prior to hospital discharge. One PU cat was euthanased as a result and the other two cats were successfully managed with temporary urethral catheterisation. Stoma stricture was seen 2 weeks after urethrostomy in one PU cat and 3 weeks after urethrostomy in one cat with TPU and one cat with PPU. The cats with PU and PPU underwent successful revision surgery; the PU was revised to a TPU and the PPU was revised to create a more cranial stoma. The cat with TPU was euthanased. Urine leakage into the peristoma subcutaneous space was successfully managed in one cat with PPU by revision surgery and one cat with PU by temporary placement of a urethral catheter. Peristomal dermatitis (Figure 9) in two cats with PPU was treated successfully with daily care, which included bathing in water, drying and application of barrier sprays.

Photo of a cat that underwent prepubic urethrostomy 14 days postoperatively. The photo demonstrates peristomal dermatitis and dribbling urinary incontinence
Three of 55 (5.4%) cats died in the short term. Short-term mortality was not associated with urethrostomy technique. One cat with PU with penile adenocarcinoma suffered respiratory arrest 3 days after urethrostomy, the cause of which was unidentified. One cat with PU and one with TPU were euthanased owing to urethral obstruction and stoma stricture, respectively, as described above.
Short-term complications were divided into minor and major complications. Minor complications were seen in 32/55 (58.2%) cats overall: 20/37 (54.0%) PU cats; 4/7 (57.1%) TPU cats; and 8/11 (72.7%) PPU cats. Major complications were seen in 9/55 (16.4%) cats overall: 5/37 (13.5%) PU cats; 1/7 (14.3%) TPU cats; and 3/11 (27.3%) PPU cats. There was no association between incidence of minor and major complications and urethrostomy technique.
Long-term outcome
The cat that underwent a TPU following stricture of the PU stoma was considered as part of the TPU group for long-term follow-up. Long-term follow-up was available for 30 cats: 14 PU cats; six TPU cats; and 10 PPU cats. The median duration of follow-up was 29.5 months (range 2–125 months). Long-term complications were reported in two (14.3%) PU cats, two (33.3%) TPU cats and seven (70%) PPU cats, and are summarised in Table 7.
Long-term complications were seen in more cats with PPU than cats with PU and TPU (P = 0.02). The only complication significantly associated with a particular urethrostomy technique was urinary incontinence, which was only seen in four (13.3%) cats with PPU (P = 0.006). No association was found between the incidence of long-term complications and any of the preoperative and operative variables reported in Tables 1–5. Both cats that underwent stoma revision surgery were included in the long-term follow-up. The cat that underwent revision of a PU to a TPU had no reported long-term complications. The cat with the revised PPU had occasional urinary incontinence.
Long-term mortality was reported in 4/30 (13.3%) cats. One cat with PPU was euthanased for reasons related to urethrostomy. This cat had recurrent episodes of cystitis, urinary incontinence and peristomal dermatitis, and was euthanased 9 months postoperatively owing to stoma stricture. Three cats died for reasons unrelated to urethrostomy.
Of the 30 cats with long-term follow up, 29 owners completed the follow-up questionnaire. Overall, most owners were satisfied with the outcome following surgery, with 28 (96.6%) owners stating they would recommend urethrostomy to other cat owners. Quality of life was rated as good in 27 cats (93.3%), moderate in one cat (3.4%) and poor in one cat (3.4%). All owners of the cats in the PU group stated that they would recommend the procedure and reported a good quality of life in their cats. The two cats rated as having a moderate and poor quality of life underwent TPU and PPU, respectively.
Discussion
To our knowledge this is the first study to directly compare the three feline urethrostomy techniques with regard to the surgical indications and short- and long-term outcomes.
This study shows that cats undergoing PU or TPU were more likely to present for FIC or urolithiasis, rather than trauma. Conversely, cats undergoing PPU were more likely to present for trauma. With regard to location of the urethral lesion, cats undergoing PU or TPU were more likely to have a penile urethral lesion, while cats undergoing PPU were more likely to have a pelvic urethral lesion. These results support the current literature, which suggests that urethrostomy technique in cats should be based on the location of urethral injury, with preservation of as much of the urethra as possible. Our study further shows that cats undergoing PPU were more likely to have a urethral rupture or stricture than cats undergoing PU or TPU.
Further, this study found no association between duration of clinical signs prior to urethrostomy and outcome. Therefore, we present no evidence to suggest that earlier surgical intervention in these cases results in fewer postoperative complications. To our knowledge, this is the first study to report the duration of clinical signs prior to urethrostomy surgery and its influence on outcome.
In this study we report short-term complications in 60% of cats undergoing feline urethrostomy, irrespective of urethrostomy technique, which is higher than previously reported for PU (13–25%)7–9 and TPU (36%), 6 and lower than that in some PPU reports (up to 83.3%). 4 The high short-term complication rate in the current study could be related to the fact that all cats were hospitalised until the time of suture removal or returned to the referral hospital for suture removal and were therefore closely observed, perhaps allowing for detection of more minor complications than in previous reports. Indeed, minor short-term complications were noted in 58.2% and major complications were noted in 16.4%.
This study reports an overall long-term complication rate of 36.7%, but the long-term complication rate was significantly higher in the PPU group (70%) compared with the PU and TPU groups. This is in agreement with previous reports, which have found a similarly high long-term complication rate of 83.3% for PPU, 5 but a long-term complication rate for PU of 25–31.8%.2,8,9
This study reports good owner-rated, long-term quality of life following urethrostomy in 93.3% of the cats, irrespective of urethrostomy technique, with 96.6% owner satisfaction. These figures are comparable to previous reports of owner-rated quality of life following PU surgery, where 75–88% of cats were judged as having a moderate-to-good quality of life.2,10 However, they are contradicted by another study, which reports a satisfaction rate of 33.3% among owners of cats undergoing PPU, which was significantly lower than the 81.8% satisfaction among owners of cats undergoing PU. 5 This difference in PPU satisfaction may be due to indication for urethrostomy, rather than surgical technique. In the study by Sousa-Filho et al, 5 the primary indication for PPU was feline lower urinary tract disease plus failed PU, but the primary indication for PPU in the current study was pelvic urethra trauma. Urethrostomy does not correct the underlying problem in feline lower urinary tract disease, but cats presenting with urethral trauma (excluding iatrogenic causes) have no underlying urinary tract disease.
In our study, 16.7% of cats had one or more UTIs during the long-term follow-up period. No difference in the incidence of bacterial UTI at long-term follow-up was seen in the surgical groups. This is in contrast to a recent study of 28 cats, which reported a higher incidence of UTIs in cats undergoing PPU vs PU (66.7% vs 22.7%). 5
Urethrostomy stricture has been reported in up to 11% of cats in early reports of PU 11 but does not feature in all case series. This may be owing to early reports identifying the primary cause for stricture as inadequate release of the penile urethra from the pelvis, 11 which could then have been avoided in later studies. A study by Bass et al 8 reported a 12% incidence of stricture within the first 4 weeks of PU. 8 A study looking at revision following PU stoma stricture reported that revision was performed at a median of 71 days following initial surgery. 12 In our study, stricture was seen in only one cat (2.9%) that underwent PU. Two previous studies have reported no stricture formation following PPU.4,5 Similarly, only 1/9 cats undergoing TPU showed evidence of stricture but showed no associated clinical signs. 6 In our study, stoma stricture was noted in one PPU cat and one TPU cat within 4 weeks of surgery and in another PPU cat 9 months after surgery. This is a major complication that resulted in euthanasia in two cats and revision surgery for one cat.
Peristomal dermatitis is another complication reported after urethrostomy. This is uncommonly reported following PU, and in a previous PU study only one cat had signs of dermatitis. 8 Peristomal dermatitis is considered more common following PPU owing to the location of the stoma and was reported in 43.7% and 83.3% of PPU cats in two separate studies.4,5 In our study, two cats, both in the PPU group, were successfully treated for peristomal dermatitis in the first 4 weeks after surgery. Two different cats in the PPU group were reported to have peristomal dermatitis in the long term.
Urinary incontinence is another reported complication that may result from nerve (pudendal nerve, sacral spinal cord or pelvic plexus) damage; excessive urethral distension secondary to obstruction; or reduction in urethral length. 13 In one study of PU cats, incontinence was not noted. 8 Incontinence has been reported in 12–58% of cats following PPU. 14 In our study, early incontinence was seen in nine cats (17%), with no difference seen among the surgical groups. However, at long-term follow-up, incontinence was significantly more common in the PPU group.
Limitations of this study include its retrospective design, the low numbers of cats in the TPU and PPU groups, and the low number of cats available for long-term follow-up. In addition, long-term follow-up ranged in duration from 2 to 125 months. Furthermore, the cats lost to follow-up were not evenly distributed between the surgical groups, with a higher percentage of PU cats being lost to follow up than TPU and PPU cats. The study was also conducted over a 10-year period. During this period the team of board-certified surgeons was very stable, but, nevertheless, multiple surgeons were involved and there may have been some unreported variations in case management. In addition, the owner questionnaire may have been exposed to a bias with satisfied owners being more likely to respond.
Conclusions
This study highlights the different surgical indications in terms of reason for presentation, location and type of urethral injury for cats undergoing perineal, transpelvic and prepubic urethrostomies. While we found that the short-term outcome was not significantly different between the three techniques, our null hypothesis was rejected, as PPU was associated with a higher long-term complication rate of incontinence than PU and TPU.
Footnotes
Author note
This paper was presented in abstract form at the 28th ECVS Annual Scientific Meeting 2020.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee, while not necessarily required, was nonetheless obtained, as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.