
Abstract
Objectives
The objective of this study was to compare ground reaction forces (GRFs) of a group of cats after femoral head and neck ostectomy (FHO) with those of a historical control group.
Methods
We searched the database of the Small Animal Clinic of the Veterinary University in Vienna for cats that had undergone unilateral FHO at least 1 year previously. Owners were telephoned and invited to the clinic with their cats for a re-examination. An in-house owner questionnaire-based evaluation, complete orthopaedic examination, hip radiography and gait analysis with a pressure-sensitive plate were performed, and results were compared within and between groups (FHO group and control group [CG]).
Results
Seventeen cats that had undergone FHO (FHO group) at least 1 year previously and 15 healthy cats (CG) from a previous study were included. Measured GRFs (peak vertical force and vertical impulse [IFz] normalised to total force [%TF]) of the FHO legs were lower than those of the other legs of the FHO group and the legs of the CG. Results of the owner questionnaire were generally good and did not match the results of the GRF comparison. Furthermore, the gaits evaluated during the orthopaedic examination did not correlate with the measured GRFs where we identified a certain degree of lameness (reduced IFz, %TF) in all cats. Cats with limb shortening (dorsally displaced major trochanter major) were not revealed to have different GRF measurements.
Conclusions and relevance
This is the first study to assess GRFs in a large group of cats that had undergone FHO, comparing findings with those in healthy cats. Even if the differences are statistically significant, but rather small, our findings point to a long-term residual gait abnormality that could be detected using a pressure-sensitive plate but not always with an orthopaedic examination, in cats 1 year after FHO.
Introduction
Hip joint injuries and pathologies in cats are common. Generally, these include fractures of the femoral head and/or neck,1–6 acetabular fractures, 1 femoral luxation1,7 and osteoarthritis (OA) secondary to hip dysplasia. 8 Femoral head and neck ostectomy (FHO) is most commonly used as a salvage procedure for the treatment of irreparable damage to the hip joint. This surgery is relatively quick and easy to perform, has a low initial complication rate and requires little follow-up by clinicians. 1 As studies have proven that FHO is not generally a good alternative to endoprosthesis, 9 total hip replacement (THR) is currently the gold standard for the treatment of hip joint disease in dogs. Reports on THR in cats indicate good mid-term functional outcomes;10–15 however, reports on the long-term outcome of FHO in cats are scarce.9,16,17 As THR has been a competitive alternative to FHO in cats for the last several years, 10 it is increasingly relevant to provide more objective data on the success of FHO in cats.
Owing to the lack of studies evaluating long-term FHO results in cats with objective outcome measures, such as gait analysis, we conducted a study to compare a group of healthy cats with a group of cats that had previously undergone unilateral FHO. The aim of the study was to clinically and radiographically reassess cats after FHO performed more than 1 year ago, by first measuring ground reaction forces (GRFs) and temporospatial parameters, and second by comparing the findings with those of a sound, historical control group (CG) from a previous study. We hypothesised that cats would display reduced GRFs (peak vertical force [PFz] and vertical impulse [IFz]) after FHO.
Materials and methods
Animals
This study was approved by the Institutional Ethics and Animal Welfare Committee and was in accordance with Good Scientific Practice guidelines and national legislation (reference number ETK-13/10/2017). We searched the database of the Small Animal Clinic of the Veterinary University in Vienna for cats that had undergone FHO between 1 January 2007 and 4 May 2017. Cats with an FHO performed on one leg (left or right hindlimb) and no additional fractures, injuries or pain in the fore- or hindlimbs at the time of the operation were included. Subsequently, a board-certified surgeon re-examined (using clinical and radiographic examinations and pressure-sensitive plate measurements) the qualifying cats at least 1 year after the operation. The CG data were retrieved from a previous study.18,19
Study design and experimental equipment
For this study, we contacted the owners of cats that had undergone FHO at least 1 year ago; their cats were brought in for re-examination and GRF measurement.
All clinical and radiographic examinations and pressure-sensitive plate measurements were conducted at one institution (University of Veterinary Medicine, Vienna, Austria). Upon re-examination, the owner was asked to complete a questionnaire; this questionnaire was adapted from a previously published and validated pain scale, 20 and an in-house visual analogue pain scale. The maximum possible score was 110 points (for the owner questionnaire, see file 1 in the supplementary material). After a complete clinical and orthopaedic examination (for the lameness grades, see file 2 in the supplementary material), the cats were brought to a quiet room dedicated to gait analysis with the owner and two researchers, in keeping with the study settings described in the previous studies with the CG cats.18,19 After a short period of acclimatisation in this room, toys, food, and verbal and visual stimuli were used to entice the cat to cross the pressure-sensitive plate in a straight line, sometimes with a portable cartoon wall placed on one side of the walkway (for the technical details, see file 3 in the supplementary material). Gait cycles were excluded when there was an apparent change in velocity (trotting or stopping), when the cat left the plate or when it turned its head. The measurements were considered valid if the cat crossed the plate at least three times, allowing for at least five valid step cycles to be measured.
After the gait analysis, radiographs (Siemens; AXIOM Iconos R 200) of the entire pelvis, hip and stifle joints, and lumbar spine were acquired in ventrodorsal and laterolateral or mediolateral views. Radiographs were assessed for arthrosis in the contralateral hip joints or lumbar spine, bony proliferations at the former resection plane and evidence of an incomplete resection.
Outcome parameters and processing
In the cats, gait velocity (V) from the left forelimb was recorded. Gait parameters evaluated were PFz (N), IFz (Ns), time to PFz (TPFz, %stance phase [StPh]), step length (SL [m]), paw contact area (PCA [cm²]) and stance phase duration (SPD [s]). The GRF data were presented as normalised total force (%TF).18,21 The symmetry indices (SIs [%]) of the forelimbs and hindlimbs were calculated from the PFz (SI[PFz]) and IFz (SI[IFz]), as described previously;18,19 an SI of 0% represents perfect symmetry between the contralateral limb pair (for the formula, see file 4 in the supplementary material).
To better compare the two groups’ legs, the left hindlimb was assessed in all previously operated legs in the FHO group. The right hindlimb was designated as the contralateral leg (CO), the left forelimb was the ipsilateral limb (IPS), and the right forelimb was the diagonal limb (DI).
Statistical analysis
All measured data were processed with SPSS, version 24 (IBM). The data corresponding to the CG were obtained from previous studies.18,19 The Kolmogorov–Smirnov test was used to determine the normality of the data distribution. Descriptive statistics were calculated for each parameter in both groups. Data are presented as mean ± SD. A general linear model (GLM) compared the legs within and between the groups. An independent sample t-test was used to detect statistically significant differences between each parameter in FHO and CG cats. Furthermore, a t-test was used to compare the parameters in FHO cats with and without a clinically determined dorsally displaced greater trochanter and an incomplete resection. Pearson’s correlation analysis was used to assess the relationship between the age of the cat at the time of operation, the results of the orthopaedic examination, and the scores from the owner questionnaires with GRFs and temporospatial parameters. A P value <0.05 was considered statistically significant.
Results
After searching the database and contacting the owners by telephone, 17 client-owned domestic shorthair (DSH) cats (Figure 1) were included in the FHO group. The historical CG consisted of 15 healthy client-owned DSH cats.

Flowchart describing the chronological order of examinations, inclusions and exclusions of cats during the search process and the number of cats finally subjected to each step.
The mean age of the cats in the FHO group was 3.0 ± 3.3 years (range 0.4–10.9 years) at the time of operation and 8.5 ± 3.3 years (range 3.7–16.0 years) at the time of re-examination. The mean time between the operation and the re-examination was 5.5 ± 2.6 years (range 1.7–10.3 years). The FHO was performed for hip luxation in 12 cats, femoral neck fracture in two cats and spontaneous capital physeal fracture in three cats. The CG included seven castrated male cats and eight spayed female cats with a mean age of 7.2 ± 4.2 years (range 2.6–14.9 years).
All data were normally distributed. Body weights of the cats in the FHO group and CG were 2.8–7.7 kg (mean 4.6 ± 1.2 kg) and 3.8–6.6 kg (mean 5.0 ± 1.1 kg), respectively; there were no significant differences between groups.
The scores from the owner questionnaire ranged from 13 to 46 points (mean 27 ± 9 points).
During the orthopaedic examination, FHO limbs of 9/17 cats were diagnosed to be sound (grade 0); 7/17 cats were found to be lame (grade 1). One cat was unwilling to move in the consultation room so the condition of its FHO limb could not be assessed. Upon palpation of FHO limbs, 13/17 cats experienced pain while flexing and extending the hip joint; in two cats, crepitus was felt. Palpation revealed that 10/17 cats had a dorsally displaced major trochanter (see file 5 in the supplementary material).
On radiographic examination, all 17 cats showed proliferations at the excision site, with five cats showing residual femoral necks. In 14 cats, the trochanter minor was not included in the resection site. Cats in the FHO group showed lumbar spine spondylosis (n = 6), contralateral hip joint arthrosis (n = 3) and ventrodorsal plane muscle atrophy (n = 10) (see file 6 in the supplementary material).
GRFs and temporospatial parameters
Gait velocity was 0.30–0.85 m/s (mean 0.63 ± 0.14 m/s) in the FHO cats, and 0.52–0.83 m/s (mean 0.70 ± 0.09 m/s) in the CG cats. There was no statistically significant difference in the velocity between the two groups.
All measured GRF values and temporospatial parameters of the FHO and CG cats are presented in Table 1. While there was no difference in the GRFs in the control cats between the contralateral legs, FHO legs showed significantly lower PFz (%TF; P = 0.045) and IFz (%TF; P <0.001) than all other legs in the FHO group, as well as the left hindlimbs in the CG (P = 0.033 and P = 0.001; Figure 2). Additionally, in the FHO group, the DI leg had higher PFz %TF (P = 0.041) and IFz %TF (P = 0.019) values than those of the remaining legs.
Ground reaction forces (normalised to total force [%TF]) and temporospatial parameters of the cats that had undergone femoral head and neck ostectomy (FHO) and those of the 15 healthy cats in the control group (CG)

Data are mean ± SD (range)
Left hindlimb in the CG or the leg with a previous FHO
Significant difference compared with contralateral limb pair
Significant differences compared with ipsilateral limb pair
Significant differences compared with diagonal limb pair
Significant differences compared with FHO and CG cats for the leg
PFz = peak vertical force; TPFz = time to PFz; StPh = stance phase; IFz = vertical impulse; SPD = stance phase duration; SL = step length; PCA = paw contact area; FL = fore left; IPS = ipsilateral; FR = fore right; DI = diagonal; HL = hind left; FHOl = previous FHO leg; HR = hind right; CO = contralateral
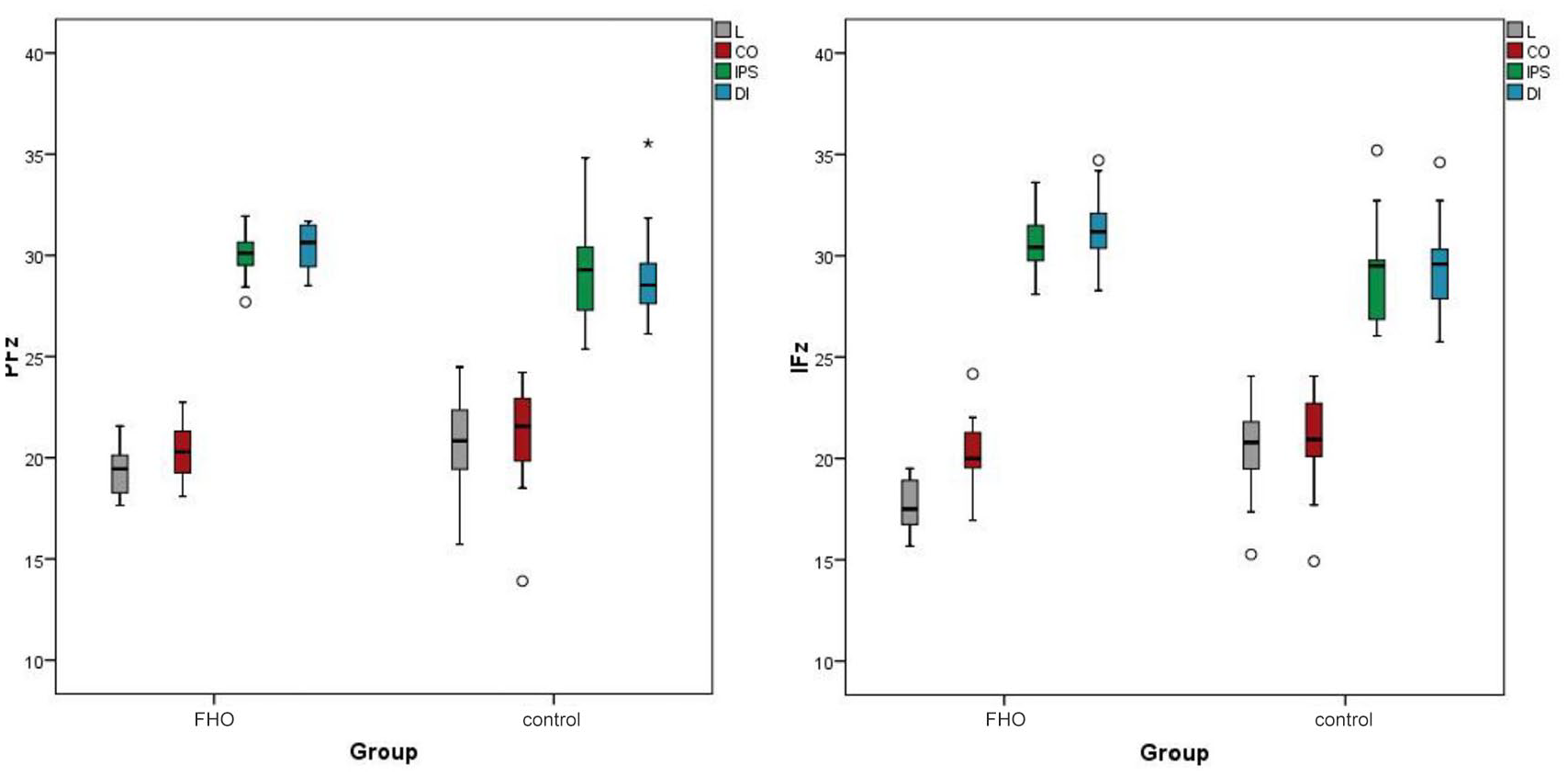
Ground reaction forces measurement (peak vertical force [PFz] and vertical impulse [IFz] normalised to total force [%TF]) in the femoral head and neck ostectomy (FHO) group and control group. Values observed more than 1.5 times the interquartile range (IQR) below the first quartile (Q1) or above the third quartile (Q3) are marked as a circle. Values more than three times the IQR below Q1 or above Q3 are marked with an asterisk. L = lame; CO = contralateral; IPS = ipsilateral; DI = diagonal
The TPFz (%StPh) of the forelimbs was significantly later than that of the hindlimbs (P <0.003) in both groups. There was no significant difference in TPFz between the forelimbs of both groups and hindlimbs of the CG. However, FHO legs showed a later TPFz than the CG legs. Similarly, with regard to DI limbs, the TPFz of the FHO was later than that of the CG (P = 0.039).
In the FHO group, the SIs(PFz) of the forelimbs and hindlimbs were 1.12% ± 0.82% and 3.54% ± 1.73%, respectively, and the SIs(IFz) of the forelimbs and hindlimbs were 3.36% ± 2.43% and 7.17% ± 3.64%, respectively. The corresponding values in CG cats were 1.35% ± 0.89% and 3.14% ± 1.79%, respectively, and 1.86% ± 1.39% and 2.40% ± 2.34%, respectively. The SIs(PFz and IFz) of the forelimbs were significantly lower than that of the hindlimbs in the FHO group (P <0.001 and P = 0.003, respectively). SI(PFz) showed no statistically significant differences between the groups; however, the SI(IFz) was always higher in the forelimbs (P = 0.039) and hindlimbs (P <0.001) of the FHO group than those in the CG.
In the FHO group, the SPD of the FHO legs was significantly shorter (P <0.002) than that of the remaining three legs (CO, IPS, DI). The forelimbs of the FHO cats showed no significant differences. There were also no significant differences between the IPS and CO. In the CG cats, the SPD of the forelimbs was significantly longer than that of the hindlimbs (P <0.003). There was no difference in SPD between the forelimbs and hindlimbs. The GLM also showed that the SPD of DI was significantly longer in the FHO group than in the CG (P = 0.04).
There was no difference in SL within (between the legs) or between the two groups (FHO group and CG). Similarly, there were no differences in the PCA between the FHO group and the CG, but (P <0.001) both forelimbs (IPS and DI) of both groups showed a larger PCA than both hindlimbs (L and CO) of both groups (P <0.001).
Furthermore, we found a significant correlation between the age at the time of surgery and forelimb SI in the FHO group (r = 0.493, P = 0.044). No other parameters seemed to be influenced by the cat’s age at the time of operation. There were no correlations found between the owner questionnaire scores and any of the other parameters (GRFs and temporospatial parameters), and between GRFs and the degree of subjective lameness during the orthopaedic examination. Specifically, 7/9 cats that were assessed as sound (grade 0) showed a reduced PFz (%TF), and all of them showed a reduced IFz (%TF) in the FHO leg. The clinically described dorsal displacement of the greater trochanter in cats did not affect the measured GRFs. Except for the SI(IFz) in the forelimbs (P = 0.041), cats with a dorsal displacement had a higher SI than in cats with a normal greater trochanter. An incompletely resected neck did not show any significant differences in GRF values or temporospatial parameters.
Discussion
Our results proved the hypothesis that FHO legs show reduced GRFs (PFz [%TF] and IFz [%TF]). In general, we found that the results did not positively correlate with the owner questionnaire scores and visual gait analysis. All cats that were found to be sound during the orthopaedic examination were shown to have a reduced IFz (%TF), and most of them were also found to have a reduced PFz (%TF) in the leg operated on.
FHO is a salvage procedure that alleviates pain in cats. Similar to previous studies, the most common indications for this operation in our population of cats were femoral luxation and fractures of the femoral head and neck.1,2,3,5,9,16 Previous studies assessing the success of FHO in cats were conducted mainly based on owners’ assessments.1,16 Owners were generally very happy with the results of the operation, and cats with FHO showed little to no deviation from their normal gait patterns.1,16 Cats are able to conceal pain very well by nature, and so validated owner questionnaires are valuable in measuring pain;20,22,23 despite this, however, the pain estimation of pet owners can often be clinically inaccurate. In a previous study, the clinician and owners found it difficult to discriminate between a lame and a healthy cat, especially when the cats were walking. 9 We experienced the same difficulty with our owner assessment questionnaire – all of the owners assessed their cats as experiencing no pain, but we were able to detect radiographic changes (eg, spondylosis and OA) in the contralateral hip joint. This finding is consistent with a report from a previous study, wherein 90% of cats had radiographic evidence of OA but only 4% of them were considered to be lame. 8
Nevertheless, as we used a non-validated owner questionnaire, conclusions should be drawn with caution. Furthermore, in our study, the clinicians were not able to detect lameness in 9/17 cats during the orthopaedic examination. One of the reasons could be that the measured differences in GRFs between the FHO and all the other legs are statistically significant but relatively small. It is unclear if lameness in FHO cats persists because of pain or if it is a sequela of pseudarthrosis and therefore a biomechanical lameness. 1 During our re-examinations, most cats experienced pain upon palpation of the diseased hip. Therefore, these results, together with the results of the GRFs, revealed that FHO in at least some of the cats can cause long-term pain and gait abnormalities.
GRF measurement has been already used to evaluate pain after onychectomy in cats;24–26 however, it has not often been used after orthopaedic operations. 27 To the best of our knowledge, only one case report has used GRFs to measure the outcome of bilateral FHO in a cat. 17 This report was able to show that 2.5 years after surgery, GRFs were equally distributed within all four legs and were within the expected physiological values for healthy cats. In dogs, Off and Matis 9 measured GRFs in a larger group using treadmills and integrated force plates after FHO, revealing results that were rated as good in 38% of dogs, satisfactory in 20% and poor in 42%. In our study, we were able to prove that cats that had undergone FHO at least 1 year previously showed lower PFz (%TF) and IFz (%TF) in the operated leg than the legs of the control cats. We also showed that FHO cats had lower GRFs and shorter SPD in the operated leg than in the other legs; they also had a higher SI in the hindlimb. This higher SI(PFz) and SI(IFz) in FHO cats is due to the lameness in the operated hindlimb. Therefore, SI can be used to distinguish between lame and healthy cats. This finding has also been described in a recent study, where the SI(IFz) in the hindlimb was always higher in a group of lame cats than in a group of sound cats. 28 Additionally, we saw that there was a positive correlation between the age at the time of surgery and the SI in the forelimb. It seems that the older the cats were at the time of surgery, the less equal the distribution of forces were over the other three legs at least 1 year after the surgery; these cats were also more likely to compensate for the change in the hindlimbs by using their forelimbs. We also found that the DI displayed higher GRFs than the legs of healthy cats. Underlying this fact, the DI also had a longer TPFz and a longer SPD in the operated cats than in the healthy cats. This might be due to a compensatory mechanism, as has been previously described in the case of dogs. 29
Incomplete resection of the femoral neck has been speculated to be one of the reasons for residual lameness.9,14 In the present study, 5/17 cats had an incompletely resected femoral neck; these cats did not show lower GRFs than the other cats. This finding is in accordance with that of Rahal et al, 17 who found no relationship between GRFs and an incompletely resected femoral neck. Resection of the minor trochanter has been speculated to reduce bony contact between the acetabulum and femur to reduce postoperative lameness. The literature suggests that this could also reduce the risk of trapping the sciatic nerve. 30 In contrast, it can be argued that the insertion of the iliopsoas muscle at the minor trochanter has a certain stabilising importance for the resected femur – it reduces the incidence of limb shortening and lameness. In three cats in our study, the minor trochanter was completely resected. None of the cats was lame upon visual orthopaedic examination, while one showed crepitus on palpation. With such a small sample size, we were unable to conclude whether the inclusion or exclusion of the minor trochanter during an osteotomy is recommended.
Exostoses should be considered as a long-term consequence of mechanical overload, and monitoring them for biomechanical function is helpful. Although Off and Matis 9 found that all cats had lesions in the trochanter minor region, these were unrelated to the functional outcome. In our study, the radiographs showed that all cats developed exostosis in the area of the former resection site, the associated acetabulum and/or the trochanter minor. This could be explained by the increased mechanical load in those areas. If, indeed, exostosis leads to lameness, the current results are unable to prove this. However, we were unable to compare this group with a group of operated cats without exostosis.
Dorsal displacement of the greater trochanter is a common sequela in FHO cats, affecting 10/17 cats in our study. The consequences, namely limb shortening and loss of extension, are suspected to cause lameness.9,10 In our study, we were unable to confirm that dorsal displacement leads to significantly lower GRFs compared with GRFs for the normal physiological position of the femur in relation to the pelvis. It is the gait that becomes more asymmetric, as indicated by the higher SI in the forelimbs in the cats with dorsal displacement. This, again, seems to be a compensatory mechanism in cats, accounting for the differences in hindlimb length.
One of the major limitations of this study is that the cats were operated on more than 1 year ago, meaning that the data were retrospective in nature. Interpretation of the results is limited by the owners’ desire to bring back their cats for re-examination, thus incurring potential observational and transfer biases. Further prospective studies with repeated measurements during the pre- and postoperative phases might be able to provide additional information and stronger data regarding the results after FHO in cats. Furthermore, the use of a historical CG, such as a group of cats that had been measured earlier, can lead to further bias. It would have been ideal to measure the studied parameters in the CG at the same time it was done in the FHO cats. Another limitation of the current study is the low number of re-examinations, as we found it difficult to compare all the clinical and radiographic results with the measured GRFs. Furthermore, the GRF measurements considers the presence/absence of lameness at only one moment in time; therefore, we do not know if the measurements vary at different times. Another drawback is the use of a non-validated owner assessment questionnaire. We suggest that further studies employ a validation process of the questionnaire to strengthen future results.
Conclusions
To the best of our knowledge, this is the first study to measure GRFs in a group of cats at least 1 year after FHO, showing reduced PFz (%TF) and IFz (%TF) during ambulation. However, the owner questionnaire scores and visual gait analysis during the orthopaedic examination failed to match these results. This may be partially due to the differences in GRF measurements in FHO cats, which were statistically significant but small. Therefore, conclusions should be made with caution. Nevertheless, we think that this fact is clinically relevant, as it is well known that orthopaedic examinations can overlook gait abnormalities, while GRF measurements can detect low-grade hindlimb lameness in cats. 28
Supplemental Material
File 1
Owner questionnaire
Supplemental Material
File 2
Lameness grades
Supplemental Material
File 3
Technical details of the pressure-sensitive plate and recording system
Supplemental Material
File 4
Symmetry index
Supplemental Material
File 5
Cats with femoral head and neck excision – results of the clinical examination and owner questionnaire
Supplemental Material
File 6
Cats with femoral head and neck excision – results of the radiographic examination
Footnotes
Supplementary material
The following files are available online:
File 1: Owner questionnaire.
File 2: Lameness grades. 31
File 3: Technical details of the pressure-sensitive plate and recording system.
File 4: Symmetry index.
File 5: Cats with femoral head and neck excision – results of the clinical examination and owner questionnaire.
File 6: Cats with femoral head and neck excision – results of the radiographic examination.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals (owned or unowned) and procedures that differed from established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient. The study therefore received ethical approval from an established committee, as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) performed (either prospective or retrospective studies). For any animals or humans individually identifiable within this publication, informed consent (either verbal or written) for their use in the publication was obtained from the people involved.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.