
Abstract
Objectives
This study compared Doppler and oscillometric (PetMAP+) devices (with or without proprietary optimisations) for the non-invasive measurement of blood pressure in conscious cats.
Methods
Twenty-three cats were enrolled; however, five were excluded as fewer than five measurements were obtained for each assessment. All measurements were obtained according to American College of Veterinary Internal Medicine consensus guidelines. Oscillometric device modes A and B were operated according to the manufacturer’s guidelines. Doppler and oscillometric devices were used alternately as the first device.
Results
Systolic arterial blood pressure (SAP) measurements were obtained by Doppler (SAPd) and oscillometry; the mean of each set of five values was used for statistical analysis. There was a significant difference between SAPd and SAP measurements in oscillometric modes A (P <0.001) and B (P <0.001). While both modes measured SAP higher than SAPd, B had a smaller bias (+15.72 mmHg) and narrower limits of agreement (LOA). There was also a significant difference between SAPd and mean arterial pressure (MAP) on oscillometric modes A (P = 0.002) and B (P <0.001). Both modes’ MAP readings were lower than SAPd and oscillometric A MAP was closer to SAPd (–14.94 mmHg), with a smaller bias and narrower LOA.
Conclusions and relevance
The findings support that Doppler and oscillometric devices cannot be used interchangeably, with or without proprietary optimisations. Methodology should always be taken into account and reference intervals (RIs) need to be defined for the different methodologies. Until methodology-specific RIs are published, definitive diagnosis of hypertension and sub-staging of patients with kidney disease according to the International Renal Interest Society guidelines remains challenging.
Introduction
Blood pressure (BP) is a valuable measurement in feline veterinary medicine. Non-invasive BP (NIBP) measurement in conscious cats is a vital part of routine monitoring of older individuals, and for patients on medication that may affect BP. Moreover, it is an important indicator of cardiovascular function in critically ill 1 and anaesthetised animals. 2 Monitoring cases of known systemic hypertension and assessing cats with potential causes of secondary hypertension are major indications for routine BP measurements in middle-aged to older cats (from 9 years of age, onwards).3–5 Primary, also called idiopathic, hypertension has been reported in 13–20% of cats with hypertension.4,6,7 It is not yet fully understood if some of these cats might have non-azotaemic chronic kidney disease (CKD), undiagnosed primary hyperaldosteronism or if environmental factors may play a role. Genetic predisposition to primary hypertension has been reported in humans; 8 however, this has not yet been documented in cats. Secondary hypertension is strongly associated with diseases such as CKD, hyperthyroidism, primary hyperaldosteronism and, less commonly, other rare diseases such as hyperadrenocorticism and pheochromocytoma.4,9,10The most common condition associated with feline hypertension in cats is CKD. Azotaemia and hypertension are intimately linked; azotaemia has been found in up to 74% of hypertensive cats, and 19–65% of cats with CKD have been found to be hypertensive.9–12 However, the prevalence and severity of hypertension does not appear to be related to the severity of the CKD.9,13,14 Hypertension is most likely to cause disease in tissues with a rich arteriolar supply3,15 and an early recognition of hypertension is required to prevent irreversible organ damage to the heart, brain, eyes and kidneys, as these are particularly vulnerable to hypertensive injury or so-called target organ damage (TOD).3,4,7,9,10,16
BP can be measured directly via intra-arterial catheterisation or indirectly via non-invasive devices that incorporate a compressive cuff placed on a limb or the base of the tail. Invasive BP (IBP) measurement is recognised as the gold standard; however, this method is not commonly used as it is impractical in routine clinical practice; it requires technical expertise, advanced medical equipment and is uncomfortable for the patient.3,17 For this reason, indirect BP measurements obtained via NIBP devices such as Doppler ultrasonic sphygmomanometry or oscillometry are more commonly used.
Doppler ultrasonic and oscillometric machines are popular NIBP devices currently available in the UK. Doppler devices have been extensively used in feline medicine,18,19 with one study demonstrating good correlation and accuracy vs direct BP assessment. 20 They detect blood flow utilising the Doppler effect on moving red blood cells. Systolic (SAP) and diastolic (DAP) arterial BP can be measured; however, the DAP measurement can be difficult to obtain, and the accuracy of these measurements is dependent on the operator’s experience, particularly when measuring DAP.2,21 It can be difficult to obtain BP values in fractious and uncooperative cats. Oscillometric devices are technically easier to use than Doppler machines. They rely on the detection of oscillations in the artery and built-in algorithmic calculations to produce automated SAP, mean arterial pressure (MAP) and DAP measurements. It is important to remember that while Doppler devices all use the same methodology, each oscillometric device uses the particular algorithm devised by its manufacturer. In addition, while they are usually easier to use than Doppler devices, it is still not always possible to achieve BP measurements using them.2,20,22–26
Studies have tried to establish reliable reference intervals (RIs) for SAP in healthy conscious and anaesthetised cats using intra-arterial, Doppler and oscillometric equipment (Table 1). A number of studies have suggested that traditional oscillometry measurements are less accurate than Doppler in conscious cats and often underestimate SAP at higher values.2,20,22,24–26 One study found no significant difference between mean SAP readings when they compared a Doppler device (CAT Doppler; Thames Medical) and an oscillometric device (Memoprint SCB; medVetGmbH); however, the oscillometric machine produced significantly higher estimates of DAP. 23 When looking at Table 1, the mean SAP by IBP ranged from 118 to 160 mmHg vs 115 to 139 mmHg for oscillometric devices and 121 to 162 mmHg for Doppler devices, so there is a great deal of variation, irrespective of the methodology or device used.
Published arterial blood pressure (mmHg) values obtained from cats

Data are mean ± SD unless otherwise indicated
IQR = interquartile range
It is important to remember that, as in other species, BP in cats varies markedly within and between individuals.19,27–29 The cat’s activity level, excitement and anxiety can play a significant role in the accurate measurement of BP. It is important to give cats time to calm down and acclimatise after entering the consultation room and to use a stress-free approach.27–29 One study showed up to an 80 mmHg change in SAP in response to a simulated clinic visit, showing the potential magnitude of situational hypertension in healthy cats. 27 Systolic arterial BP can be affected by many external variables, including the operator, conditions within the environment when and where the BP measurement is taken, the equipment, the position of the cat, the size of the cuff and the site of measurement.19–21,23,27,29,36–39 Accepting the difficulties of gaining reliable BP readings, once each clinic establishes its own reliable protocol and its own bias on the RI (eg, being higher in a noisy clinic), BP can be reasonably reliably assessed in pet cats.
While there appear to be no gender or breed effects on BP,31,32 a large longitudinal study established a small but significant increase in BP with increasing age, equating to ~1–2 mmHg per annum for cats over 9 years of age. 14 Indirect SAP measurements exceeding 160 mmHg have been associated with TOD in several studies.4,7,10,12,40–43
The purpose of this prospective study was to evaluate the agreement of SAP measured using a Doppler machine (Parks model 811; Parks Medical Electronics) and an oscillometric device (PetMAP+, model 7142; Ramsey Medical) in two modes: mode A (PetMAP+ mode for proprietary optimisations [PPO]) and mode B (Optimized None [ON]). The PPO mode has built-in proprietary algorithms designed to optimise the estimation to equate to intra-arterial pressure. As IBP measurements could not be performed as a comparison, the accuracy of either machine could not be compared against a gold standard control. The hypothesis was that there would be good agreement between SAP measurement by the Doppler and the oscillometric device.
Materials and methods
Animals
The study was conducted in the Hospital for Small Animals of the Royal (Dick) School of Veterinary Studies in 2015. The survey was approved by the Veterinary Ethical Review Committee (VERC) at the Royal (Dick) School of Veterinary Studies. The ethical review committee approved this study to be conducted under the legislation of Animals (Scientific Procedures) Act 1986. Feline inpatients and healthy cats belonging to staff members were recruited for this study. Cats that were fractious, uncooperative and that moved excessively were excluded. Any cat receiving a drug known to have an effect on BP, or that had been anaesthetised or sedated within the previous 12 h, was also excluded.
BP measurements
To achieve standardised conditions all BP measure-ments were obtained according to the guidelines in the American College of Veterinary Internal Medicine (ACVIM) consensus statement on feline hypertension. 3 A single, well-trained operator with the help of a consistent assistant made all BP measurements in a designated cat ward. The Doppler (Parks model 811; Parks Medical Electronics) and oscillometric (PetMAP + model 7142; Ramsey Medical) devices were used alternately as the first device. Both devices were operated carefully according to the manufacturer’s guidelines. Measurements were taken on the antebrachium of the non-weightbearing forelimb, with the cat sitting comfortably and the limb positioned at the level of the heart. The same inflatable cuff provided by Ramsey Medical was used for both devices. An ideal cuff width between 30% and 40% of limb circumference was chosen. Prior to all BP measurements, each cat was given a 5-min acclimatisation period to the inflatable cuff in the aim of reducing stress-induced situational hypertension. All BP measurements were performed successively with the first measurement of each device discarded and the subsequent five measurements averaged.
Doppler measurement
The hair over the probe site was not clipped to reduce stress to the cat. Coupling gel was placed over the palmar aspect of the common digital artery and the Doppler probe was applied to obtain a clear audible sound. The cuff was manually inflated until the pulse signal was no longer audible, then gradually deflated. The reappearance of flow sounds in conjunction with the manometer reading represented the SAP (as it was for the Doppler device; SAPd). The cuff was completely deflated between each measurement.
Oscillometric measurement
The device was programmed to ‘Clinic Mode’ for full operator control over the timing and frequency of BP measurements. Measurements were taken from the ON mode and PPO mode for ‘Cat Forearm’ to obtain SAPon and SAPppo. Indirect MAP and heart rate readings were taken automatically, from which SAP and DAP were calculated by the device. Readings that were obtained during a sudden movement or displayed a poor oscillometric envelope were discarded and subsequently replaced.
Statistical analysis
The mean of the five SAP measurements was used for statistical analysis. Bland–Altman analysis was used to determine the agreement between SAP measurements of the Doppler and SAP of the oscillometric device in both modes, as well as SAP measurements of the Doppler and MAP of the oscillometric device in both modes. The differences in SAP (SAPon – SAPd) or (SAPppo – SAPd) were plotted against the mean of each pair of measurement. The bias was defined by the mean differences between the two methods (∑ [SAPon – SAPd]/n) and (∑ [SAPppo – SAPd]/n). The precision was calculated from the SD of the differences and limits of agreement (LOA) were calculated from the bias ± 1.96 × SD. A paired-sample t-test was run to determine whether there was a statistically significant mean difference in the SAPd compared with the SAP measured by the two oscillometric device modes. Results were presented as mean ± SD. A P value <0.05 was considered significant. Overall statistical analysis was achieved using GraphPad Prism version 8.2.1.
Results
Successful readings
Twenty-three cats were enrolled; however, five cats were excluded as fewer than five BP measurements could be obtained for each assessment. In total, 18 cats were included in the study: 10 males and eight females, with a median age of 8 years (range 9 months to 17 years).
A total of 270 measurements were taken from the 18 conscious cats, with 90 readings from the Doppler, and each of the oscillometric device modes (Table 2). Measurements for these 18 cats were successfully obtained in 100% of attempts using the Doppler device and 94.4% of attempts using the oscillometric device. Five of the oscillometric readings were unsuccessful as they displayed a poor oscillometric waveform envelope and were therefore discarded as unreliable results. These are not present in the data in Table 3. The hypertensive patients were followed up and treated appropriately.
Average of blood pressure measurements obtained from the 18 cats included in the study
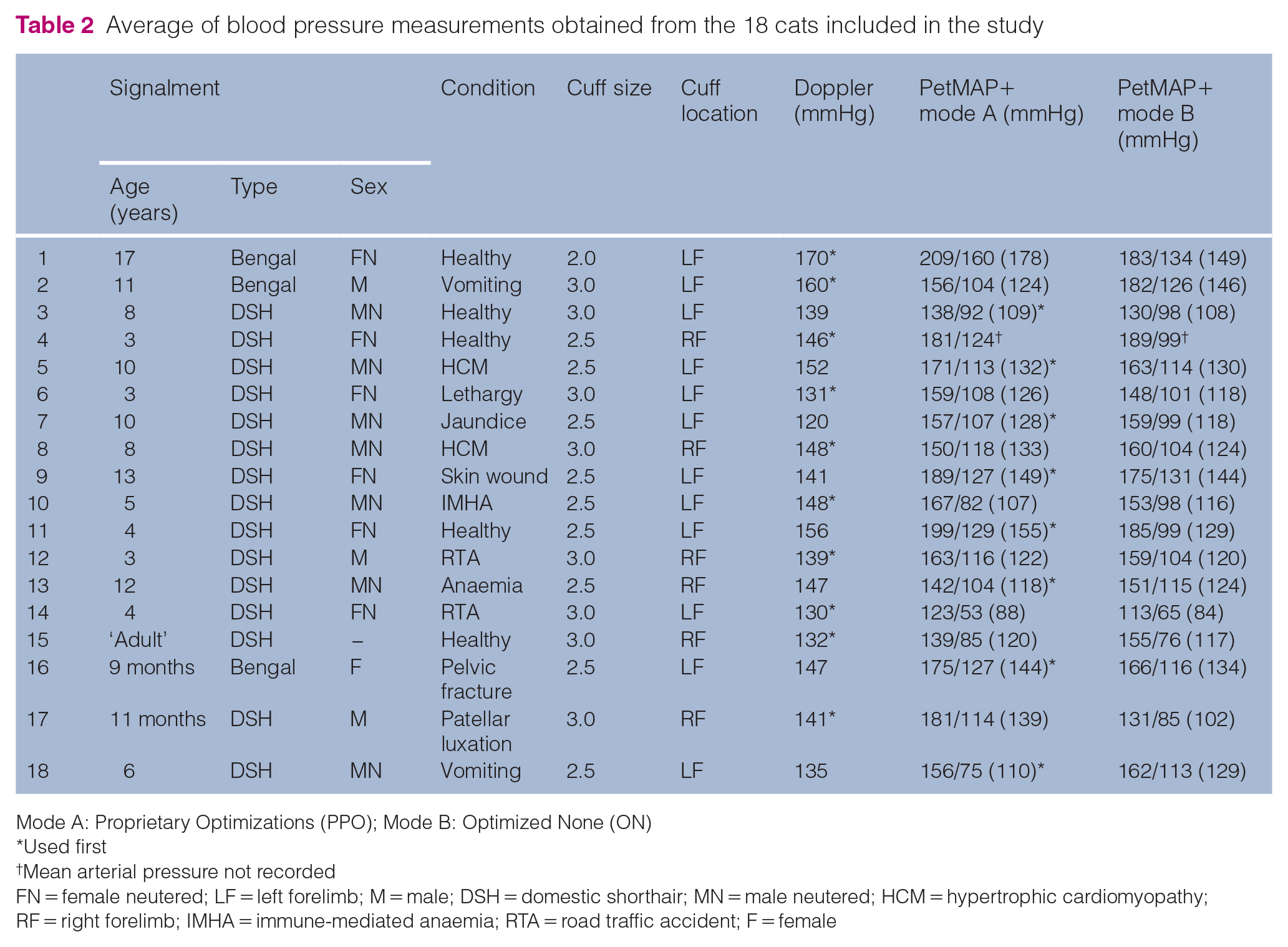
Mode A: Proprietary Optimizations (PPO); Mode B: Optimized None (ON)
Used first
Mean arterial pressure not recorded
FN = female neutered; LF = left forelimb; M = male; DSH = domestic shorthair; MN = male neutered; HCM = hypertrophic cardiomyopathy; RF = right forelimb; IMHA = immune-mediated anaemia; RTA = road traffic accident; F = female
A summary of Bland–Altman analyses of PetMAP+ Proprietary Optimizations (PPO) (mode A) and Optimized None (ON) (mode B) function vs Doppler in conscious cats

Lowest and highest measurement recorded
BP = blood pressure; LOA = limits of agreement; SAP = systolic arterial pressure; MAP = mean arterial pressure
Agreement between SAPd and SAP (oscillometric device)
Bland–Altman analyses of the differences between SAP measurements from the two devices were plotted against the mean of the SAPd (Figures 1 and 2). Comparison of oscillometric mode A with SAPd gave an average bias of +21.28 mmHg (95% confidence interval [CI] 12.49–30.07 mmHg). The lower limit of agreement (LLA) was calculated as −13.36 mmHg, and the upper limit of agreement (ULA) was calculated as +55.92 mmHg; the difference between the upper and lower limits was 69.28 mmHg. Comparison of oscillometric mode B with SAPd produced an average bias of +15.72 mmHg (95% CI 7.46–23.98 mmHg). The LOA were calculated as −16.83 for the LLA and +48.28 for the ULA; the difference between LLA and ULA was 65.11 mmHg.

Bland–Altman plot of the differences between systolic arterial blood pressures (SAPs) measured by the Doppler and PetMAP+ Proprietary Optimizations (PPO; mode A) oscillometric device; measurements from the two devices were plotted against the mean of the Doppler SAP measurements. Dashed line indicates the bias (average difference); dotted lines indicate the upper limit of agreement and lower limit of agreement

Bland–Altman plot of differences between systolic arterial blood pressures (SAPs) measured by the Doppler and PetMAP+ Optimized None (ON; mode B) oscillometric device; measurements from the two devices were plotted against the mean of the Doppler SAP measurements. Dashed line indicates the bias (average difference); dotted lines indicate the upper limit of agreement and lower limit of agreement
There was a significant difference between SAPd and oscillometric modes A (P <0.001) and B (P <0.001). As indicated by the bias, both oscillometric device functions overestimated the SAP vs SAPd. However, the oscillometric mode B performed better for the detection of SAP, as demonstrated by the smaller bias and narrower LOA. A possible proportional bias was noted on both modes as the degree of the overestimation was greater at higher than at lower BP measurements: this suggests there is less agreement between the methods when measuring higher BP.
Agreement between SAPd and MAP (oscillometric device)
The differences between MAP measurements were plotted against the SAPd (Figures 3 and 4). Comparison of MAP on oscillometric mode A with the SAPd gave an average bias of −14.94 mmHg (95% CI −23.66 to −6.22 mmHg). The LOA were calculated as −48.18 mmHg for the LLA and +18.30 mmHg for the ULA; the difference between LLA and ULA was 66.48 mmHg. The comparison of MAP on oscillometric mode B with the SAPd produced an average bias of −20.24 mmHg (95% CI −26.78 to −13.70 mmHg). The LOA were calculated as −45.17 for LLA and +4.70 for ULA; the difference between ULA and LLA was 49.86 mmHg.
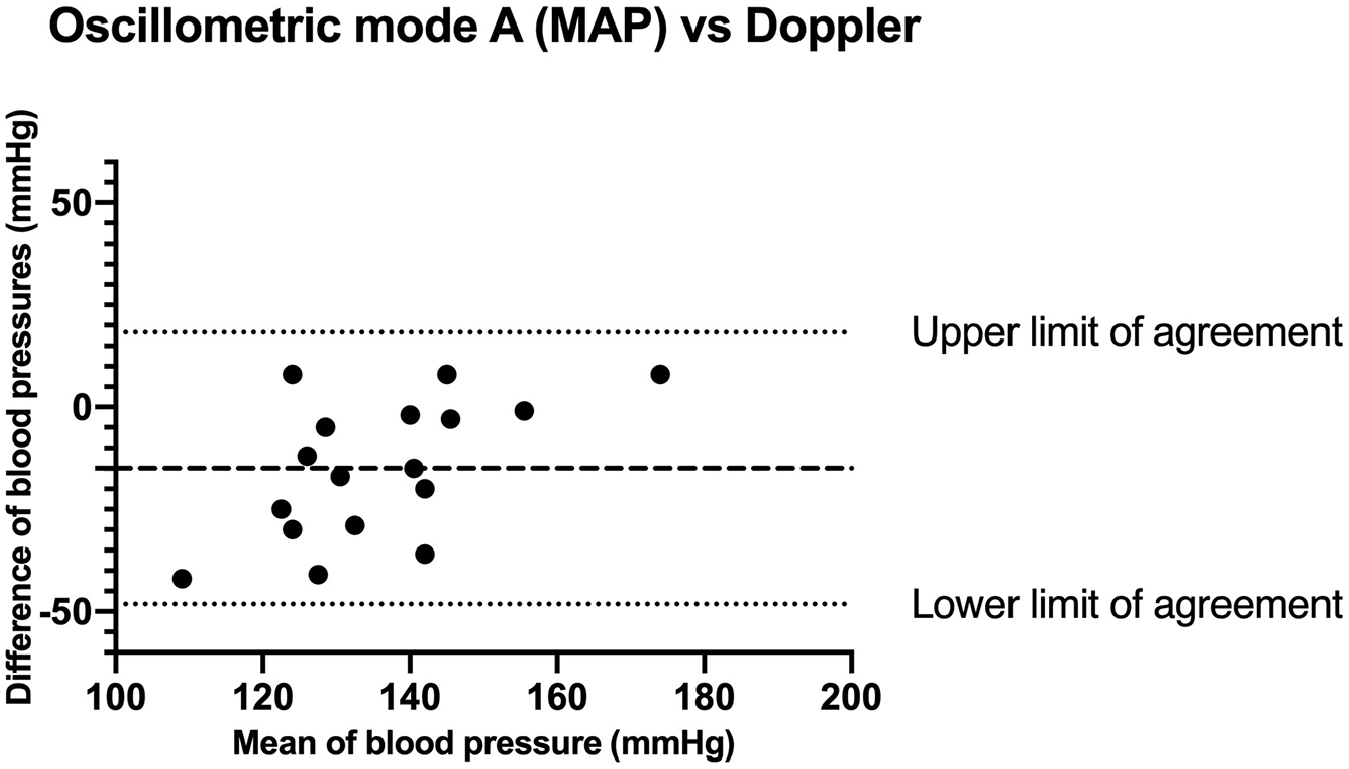
Bland–Altman plot of the differences between systolic arterial blood pressures (SAPs) measured by the Doppler and mean arterial pressure (MAP) by PetMAP+ Proprietary Optimizations (PPO; mode A) oscillometric device; measurements from the two devices were plotted against the mean of the Doppler SAP measurements. Dashed line indicates the bias (average difference); dotted lines indicate the upper limit of agreement and lower limit of agreement

Bland–Altman plot of differences between systolic arterial blood pressures (SAPs) measured by the Doppler and mean arterial pressure (MAP) by PetMAP+ Optimized None (ON; mode B) oscillometric device; measurements from the two devices were plotted against the mean of the Doppler SAP measurements. Dashed line indicates the bias (average difference); dotted lines indicate the upper limit of agreement and lower limit of agreement
There was a significant difference between the SAPd and oscillometric MAP in mode A (P = 0.002), as well as between SAPd and oscillometric MAP in mode B (P <0.001), with the MAP being lower than SAPd. Oscillometric mode A was closer to the SAPd as demonstrated by the smaller bias and narrower LOA. A possible proportional bias was noted on mode A as the degree of the underestimation was greater at lower than at higher BP measurements. This trend was not noted with mode B.
Discussion
The aim of this study was to compare the Doppler BP device (Parks model 811) to the more recently marketed veterinary oscillometric machine (petMAP+). The study evaluated the bias and precision of SAP measurements with this oscillometric device set in two different modes; petMAP+ PPO (mode A) and ON (mode B). The study showed that the oscillometric device had poor agreement with paired Doppler measurements in conscious cats. The reported positive bias and wide variability of SAP for both oscillometric modes indicated poor agreement and precision. In both modes, the mean SAP was higher than that for the Doppler (bias of + 21.28 mmHg and + 15.72 mmHg for modes A and B, respectively). It has been suggested that SAPd may be more reflective of MAP in cats. 44 To investigate this the oscillometric device MAP measurement was compared with SAPd and found to be lower (bias of −14.94 mmHg and −20.24 mmHg for modes A and B, respectively).
Other oscillometric devices are also reported to show significant variability in BP measurements; these include the Memoprint SCB (medVet), 23 Memo Diagnostic HDO Pro SþB (medVet) 5 and Dinamap Model 8300 (Critikon). 20 A study evaluating the previous petMAP device reported poor agreement between the indirect and direct BP methods, and concluded that the device could not be recommended for BP measurements in cats. 45
The newer petMAP+ oscillometric device was evaluated in an unpublished study of 10 cats, and reported overall improvements to BP accuracy and oscillometric sensitivity; however, the cats were lightly anaesthetised. 46 In the present study, using the same device as above, but in conscious cats, the readings with mode B (ie, mode ON) showed a better accuracy and precision to SAPd than mode A (although it gave a mean bias of +15.72 mmHg). This is in agreement with the manufacturer, who states that petMAP+ ON should show better correlation with ‘other [indirect] BP devices’. However, the manufacturer states that PetMAP+ PPO (mode A) is designed to improve the correlation between NIBP to IBP measurements; it is also unique to the selected species (dog and cat) and cuff placement site (forelimb, tail or hindfoot). Built-in proprietary algorithms have been formulated to produce readings that are 10–20% higher than SAPd, on the basis that Doppler devices consistently underestimate the intra-arterial SAP; hence, it should reflect intra-arterial SAP more accurately. The tendency of Doppler devices to consistently underestimate intra-arterial SAP has been supported by several studies in anaesthetised cats.2,36,44 In the current study, using mode A, SAP gave a mean bias of +21.28 mmHg, so it was ~10–20% higher, as per the manufacturer’s claims. It has been previously described that SAPd is occasionally closer to MAP than SAP as measured by IBP.46,47 In the current study, MAP (by oscillometry) had a mean bias against SAPd of −14.94 mmHg in mode A, and −20.24 mmHg in mode B, which means MAP (by oscillometry) was overestimated by the SAPd in both modes; however, the true relationship of MAP (by oscillometry) and MAP (by IBP) is unclear at this time.
Studies have assessed IBP, and compared it with oscillometric and Doppler devices, in conscious and anaesthetised cats (Table 1); unfortunately, no study has compared all three devices in both situations. Some studies have attempted to validate indirect BP devices in anaesthetised patients, while fewer have been performed in conscious animals.19,20,22,23,32–34 In one study, the Doppler (Parks model 811; Parks Medical) and oscillometric devices (Dinamap 8300; Critikon) provided a reliable estimate of BP in anaesthetised cats; however, the Doppler device provided the most reliable measurements in conscious cats. 20 It has been suggested that traditional oscillometry is less accurate than Doppler in conscious cats as it often underestimates BP, especially at higher values, and produces less reliable readings.2,20,23,24,26 In contrast, the current study found the oscillometric device overestimated the SAP vs the Doppler. That said, its SAP on mode A was almost within the 10–20% the manufacturer defined, which may be closer to the real SAP; it also found MAP to be within the 10–20% the manufacturer defined in mode A. As with other studies, there was considerable variation between the two devices; although the mean SAP of the Doppler device was close to those previously reported (ie, 143 mmHg vs from 121 to 162 mmHg; Table 1), the mean SAP of the oscillometry device in both modes was higher than previously reported (ie, 159 or 164 mmHg vs from 115 to 139 mmHg; Table 1). Moreover, they were not defined enough to be usefully applied to ACVIM guidelines. Further studies are needed before devices that can meet the guidelines for measuring BP in conscious animals can be universally validated; ACVIM guidelines recommend that currently available devices should be used with a degree of caution. 3
Consistent with several studies reporting measurement failures in the evaluation of oscillometric devices, albeit in anaesthetised cats,2,5,20 failure to obtain a reading occurred in approximately 5.6% of the measurement attempts with the oscillometric device in the current study. Previous user-specific errors that have been shown to have an adverse effect on BP determinations include the operator’s experience with the Doppler device2,21 and improper cuff size in both Doppler and oscillometric devices.2,19 As the same cuff was used for both machines, and the operator was experienced, these were unlikely to have played a significant role the current study’s findings.
The main limitations of the study were its small sample size and that a comparison of the two non-invasive methods were not compared with a direct gold standard BP measurement. To compare both modes on the oscillometric device with the Doppler, each cat had to have >15 individual BP assessments. This means that even some of the placid cats became restless, so a full assessment could not be performed, and cats had to be removed from the study. A larger number of cats would have improved the study, as would having more cats with BP above and below the RI. However, as participation involved numerous BP measurements, the stress of inclusion would have been inappropriate for hypertensive patients. Most hypotensive cats are hospitalised in our Intensive Care Unit, where such a study is not allowed.
It has been suggested that lower RIs for normal SAP values should be used when using oscillometric devices, compared to those used with the Doppler, as two cats with ocular TOD were missed using the Memoprint oscillometric device (medVet). 23 However, the range of mean values found with both types of device is very variable (Table 1), and the current study found that oscillometric SAP was higher than SAPd, rather than lower, so this suggestion does not appear sensible. There is a real need for method-specific RIs, one for SAPd and another for oscillometric devices; that is, if different oscillometric devices can be found to have the same RI (which has so far not proved to be the case; Table 1). Additional studies may be able to determine if it is possible to create a conversion calculation between Doppler and newer oscillometric devices. Given the potentially deleterious effects of missing hypertensive cats and overtreating cats falsely believed to be hypertensive, this area of feline medicine urgently needs more investigation.
Conclusions
This oscillometric device did not produce SAP readings in good agreement with the Doppler device in conscious cats. While the petMAP+ PPO features did produce results 10–20% higher than SAPd, which the manufacturer suggests is more consistent with invasive BP monitoring, there was still variability and lack of a gold standard. However, the beneficial qualities of the oscillometric device such as portability, intuitive user interface and minimal requirement of restraint still renders this device (and other oscillometric machines) a useful option in fractious and uncooperative cats. Owing to the previously reported tendency of some oscillometric devices to underestimate SAP, especially at higher values,2,20,23–25 compared with the Doppler, while the current study found the PetMAP+ to overestimate SAP, all BP readings should be integrated with the patient’s history and physical examination.Importantly, individual cats should be assessed using the same machine, cuff size and procedure each time (which should be recorded in their notes) so that changes over time can be assessed; this way, they become their own control, unrelated to any published RIs. Regardless of the BP measurement method and BP value, significant clinical signs that reflect TOD should be investigated via a funduscopic examination, neurological evaluation and thoracic auscultation. 16 Methodology-specific RIs are needed for more accurate sub-staging of patients with kidney disease, and decision-making about when to start antihypertensive treatment, as the current variability makes decision-making according to the International Renal Interest Society, International Society of Feline Medicine and ACVIM guidelines challenging.48–50
Footnotes
Acknowledgements
The authors would like to thank all of the owners who allowed their cats to be used in this study, Dr Darren Shaw for his help with statistical analysis of these data and Luke Winter for cat holding assistance while the cats had their blood pressure taken. The petMAP+ device was kindly lent by Ramsey Medical.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals (owned or unowned) and procedures that differed from established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient. The study therefore had ethical approval from an established committee as stated in the manuscript.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.