
Abstract
Objectives
The aim of this study was to assess outcomes in cats diagnosed with uroabdomen at a single referral centre.
Methods
Fifty-three cats diagnosed with uroabdomen at a veterinary teaching hospital were identified between June 2003 and September 2016. Data collected included signalment, presenting signs, aetiology, location of rupture, presence of concurrent injury, outcome of urine culture, presence of uroliths and packed cell volume (PCV)/creatinine/potassium levels at presentation. Cats managed medically and surgically were included, and the use of urinary catheters, cystotomy tubes and abdominal drains were recorded. It was determined if patients survived to discharge or if they were euthanased or died.
Results
Seventy-four percent (n = 39) of cats survived to discharge. Elevations in creatinine (P = 0.03) were shown to be significantly correlated with survival to discharge. Sex, age, location of rupture, presence of uroliths, outcome of urine culture, presence of concurrent injury, potassium at presentation and PCV at presentation were not associated with survival to discharge. There was no difference in survival between cats that were medically or surgically managed.
Conclusions and relevance
Cats that develop uroabdomen have a good chance of survival. Electrolyte and biochemistry values should be assessed at the time of presentation, in addition to the presence of concurrent injury.
Introduction
Uroabdomen is defined by the presence of urine in the abdominal cavity as a consequence of rupture of the urinary tract. It can lead to metabolic and multisystemic disturbances, which can be fatal if not treated. In cats, the most common site of rupture is the urinary bladder. 1 There is no age or breed predisposition. 2 A previous abstract of 110 cats with pelvic fractures found that male cats were at increased risk of developing urethral rupture or uroabdomen. 3 Studies in dogs have indicated that males have a higher risk of developing traumatic urinary bladder rupture and, subsequently, developing uroabdomen.1,2 Delay in the diagnosis of uroabdomen has been shown to increase mortality rates. 4
The most commonly reported cause of uroabdomen in both cats and dogs is blunt or vehicular trauma.1,4–6 Iatrogenic trauma and urethral obstruction have also been identified as causes of uroabdomen. 7
Presenting signs of patients with uroabdomen will vary depending on the aetiology, location and duration of urinary tract rupture. Reported clinical signs in cats include lethargy, anorexia, abdominal pain, ascites, dehydration, haematuria, dysuria, vomiting, hypothermia and other signs relating to trauma.2,5,8–10 Rupture of the urinary tract cannot be ruled out on palpation of an intact urinary bladder or the patient’s ability to urinate normally.4,7
Patients with uroabdomen can present as an emergency and need to be stabilised with medical management. Typical issues that need addressing include azotaemia, metabolic acidosis, hyponatremia, hyperphosphatemia and hyperkalaemia.4,5,10 Surgery may be required in some cases to correct the defect in the urinary tract.
The current literature in cats focuses on the aetiology, diagnosis and treatment of patients that develop uroabdomen.1,5,8 There is a paucity of information that identifies prognostic factors associated with uroabdomen in cats. This study aims to highlight factors that are associated with outcome in a retrospective population of cats.
Materials and methods
Electronic medical records from a veterinary teaching hospital were analysed to identify patients diagnosed with uroabdomen over a 12-year period between June 2003 and September 2016.
Inclusion criteria included cats of any age or sex that had been diagnosed with uroabdomen. Cats were excluded if they were euthanased within 2 h of presentation. Uroabdomen must have been diagnosed by either comparing biochemical parameters of abdominal fluid and peripheral blood or by contrast radiography, confirming extravasation of fluid from the urogenital tract into the abdominal space. Clinical management of each case was at the discretion of the clinician.
Data collected from the medical records included signalment, presenting signs, aetiology, location of rupture in the urinary tract, the method of diagnosis, if contrast was used, concurrent injury (musculoskeletal or soft tissue), presence and type of uroliths, if the case was managed medically or surgically, surgical procedure performed (if relevant), bacterial culture results and time until discharge. The use of abdominal drains, urinary catheters and cystotomy tubes was also recorded. Records also identified potassium, creatinine, packed cell volume (PCV) and total solids at presentation. For analysis, age was classified using previously published life stage guidelines in cats. 11 PCV was categorised as low (<29), normal (29–48) and high (>48), using published reference intervals (RIs). 12 Aetiology was categorised into the following subgroups: external trauma (road traffic accident, other blunt trauma or dog fight); iatrogenic (cystocentesis, urinary catheterisation or manual bladder expression, or postsurgery); urethral obstruction; and unknown. For cats to be considered medically managed, no surgical intervention was performed, and they were managed with either an indwelling urinary catheter or abdominal drain. Survival to discharge was noted; if the patient did not survive to discharge the reason for euthansia or cause of death was identified.
Statistical analysis
All non-normally distributed continuous data were described using the median with a range. Non-parametric continuous data were analysed using the Mann–Whitney test. Categorical data were analysed using either Pearson’s χ2 test or Fisher’s exact test; the former was used when cells were >5. P values <0.05 were considered significant.
Results
Fifty-three cats met the inclusion criteria. Of these, 68% (n = 36) were male and 32% (n = 17) were female. The median age of cats in this study was 4 years (range 0.75–12 years). The median body weight was 4.5 kg (range 2.4–7.0 kg).
The most common presenting signs included inappetence (36%; n = 19), lethargy (28%; n = 15), abdominal pain (23%; n = 12), dysuria (19%; n = 10) and vomiting (15%; n = 8). The most common cause of uroabdomen in this study was urethral obstruction (21%; n = 11), followed by being hit by a car (19%; n = 10) (Figure 1).

Aetiology of cats in this study diagnosed with uroabdomen
Survival to discharge
Seventy-four percent (n = 39) of cats survived to discharge; 19% (n = 10) were euthanased and 8% (n = 4) died. The causes of death and euthanasia in cats managed medically and surgically are represented in Figure 2. Sex, age, location of rupture, presence of uroliths, outcome of urine culture, presence of concurrent injury, potassium at presentation and PCV at presentation were not associated with survival to discharge (Table 1). Whether a patient was medically or surgically managed had no correlation with survival to discharge.

Causes of death and euthanasia of cats in this study that did not survive to discharge (n = 14)
Characteristics of cats diagnosed with uroabdomen associated with survival to discharge
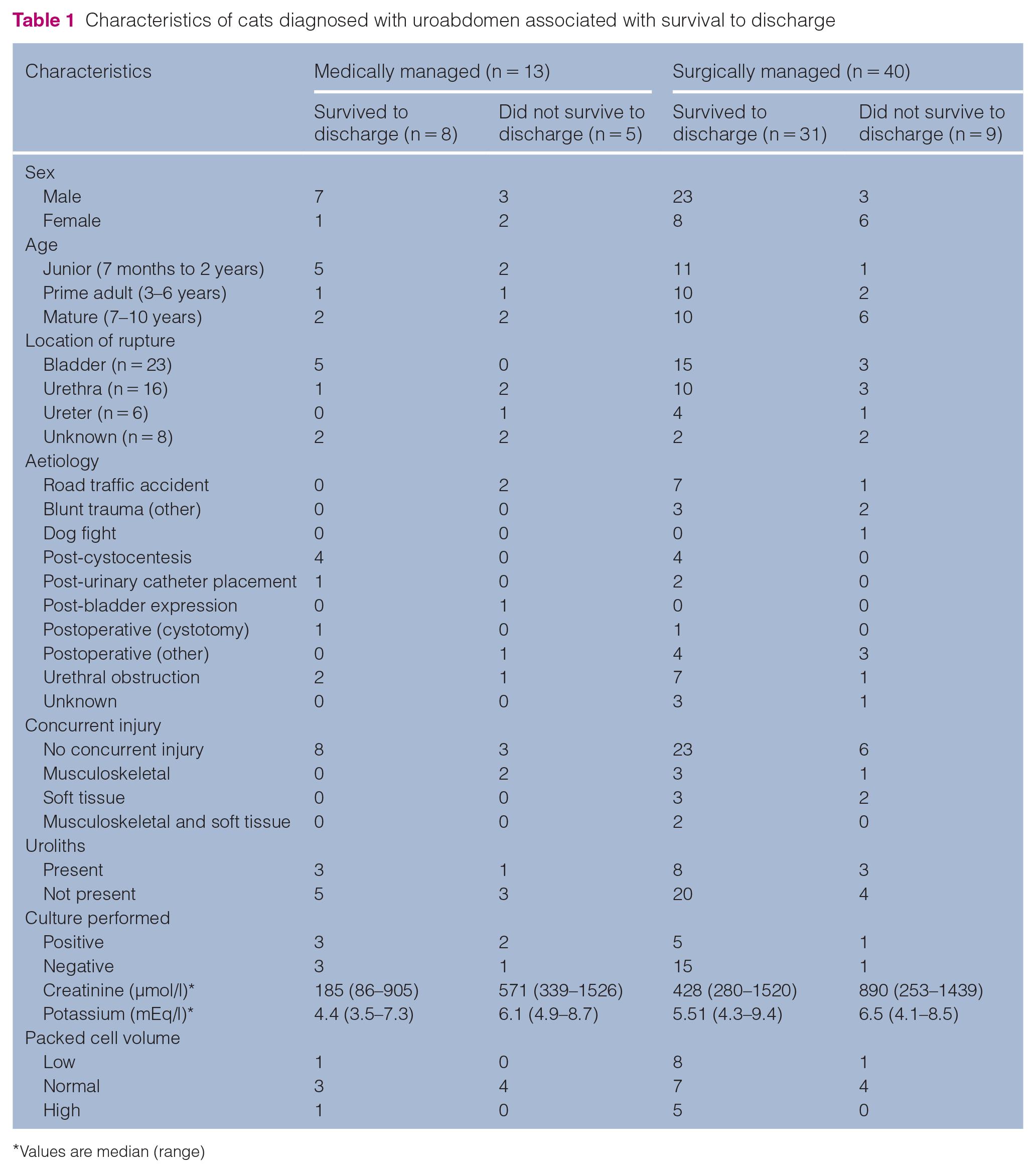
Values are median (range)
Elevations in creatinine on presentation (P = 0.03) were shown to be significantly associated with failure to survive to discharge in a univariate analysis.
Five patients had pelvic fractures; of these, four survived to discharge. All pelvic fractures were caused by blunt trauma, four of which were road traffic accidents.
Medical management
Twenty-five percent (n = 13) of cats with uroabdomen received only medical management; of these, 62% (n = 8) survived to discharge. Abdominal drains were placed in six medically managed cats, of which two survived. Urinary catheters were placed in six cats, of which all six survived. One cat, which did not survive, had both a urinary catheter and abdominal drain.
Surgical management
Seventy-five percent (n = 40) of cats underwent surgery to manage their uroabdomen; of these, 78% (n = 31) survived to discharge. Contrast imaging was used to determine the location of rupture in 85% (n = 34) of cats managed surgically. Four cats had preoperative abdominal drains placed; three of these survived to discharge. Postoperatively, five cats were managed with a urinary catheter; all of these survived. Fifteen cats had postoperative cystotomy tubes; of these, 12 survived. Ten cats had abdominal drains postoperatively; of these, six survived. Two cats had both a cystotomy tube and abdominal drain; one survived. In two cats that died owing to cardiac arrest, one died during recovery from anaesthesia and one died 5 h after recovery from anaesthesia. Two cats were euthanased intraoperatively due to intraoperative findings suggesting a poor prognosis.
Discussion
In this study, the mortality rate of cats diagnosed with uroabdomen was 26% (n = 14). Other recent studies had similar mortality rates of 25% in cats that developed urethral ruptures, 13 and 38.5% in a study of 26 cats with uroabdomen. 5
The most common reason for euthanasia in the present study was acute kidney injury (AKI) in three cats and deteriorating clinical status in three cats. In the cats with AKI, elevations in both urea and creatinine above the RI were noted postoperatively. Although none of the clinical records noted financial reasons for euthanasia, it is difficult to ascertain whether this played a role in the decision to euthanase cats within this study. The owner of one cat that was medically managed declined surgery for unknown reasons; this cat was euthanased owing to clinical deterioration.
Male cats were over-represented in this study, with similar findings in other studies.5,14 Male cats have longer and narrower urethras than females; previously, it has been discussed that this may make bladder rupture more likely as it cannot adapt to a sudden increase in urinary tract pressure. 1 Although this study included more male cats, it did not show that survival to discharge was associated with sex.
Trauma (external and iatrogenic) was the most common cause of uroabdomen in 53% of cats. This was in agreement with other studies; a retrospective study of 26 cats with uroperitoneum found trauma was associated with 85% of cases. 5 A more recent study looking into urethral rupture in 63 cats found trauma was the cause in 56% of patients. 13 There was no correlation between trauma and survival to discharge in this population of cats.
The most common location of rupture in this study was the urinary bladder (43%; n = 23), followed by the urethra (30%; n = 16); a study of 26 cats also had similar findings. 5 No correlation between location of rupture and survival was made.
In this population of cats, a correlation between elevations in creatinine and not surviving to discharge was shown to be statistically significant. When patients develop uroabdomen, potassium from the urine is reabsorbed through the peritoneal membrane, leading to hyperkalaemia. 15 Creatinine is similarly reabsorbed, but, being a larger molecule, this process occurs more slowly than potassium; therefore, elevations in creatinine may suggest the presence of uroabdomen may be more prolonged, leading to a poorer outcome. All cats that did not survive to discharge within this study had creatinine levels above the normal RI on presentation. Given the small cohort and low death rate, clear conclusions cannot be made between outcome and creatinine levels on presentation.
In this study, there was no statistically significant difference in survival between cats that were managed surgically or medically. Surgery was aimed at correcting a defect in the urinary tract or providing urinary diversion, and therefore further stabilising patients. This study did not identify whether patients developed intraoperative or postoperative complications. Causes for euthanasia in cats that did not have surgery included deteriorating clinical status, development of anuria and poor prognosis. All cats that had only urinary catheters placed survived to discharge; small tears of the bladder or urethra can heal without surgery with urinary catheter placement.7,16
In this study, 25% of cats had concurrent injury; however, this was not shown to correlate with survival. Patients with uroabdomen can have a variety of concurrent conditions such as fractures, neurological dysfunction and abdominal organ damage, among others. Other studies have shown that concurrent injury negatively impacts survival. Feline trauma patients with multiple injuries were shown to have an increased mortality rate. 17 Patients that had diaphragmatic hernias with concurrent soft tissue and orthopaedic injury were shown to have a lower survival rate. 18 This study had a small cohort with a low death rate, with a small proportion having concurrent injury, which may limit our interpretation of the data.
Owing to the retrospective nature of this study, it was not possible to collect all desired data for each patient. There was variability between clinician techniques and records.
Conclusions
This study indicated that cats that develop uroabdomen have a good chance of survival. Patients should have their electrolyte and biochemistry values assessed on presentation and concurrent injury identified. Although primarily a surgical condition, in which defects in the urinary tract should be surgically managed, sole medical management can be successful in appropriate cases.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not necessarily required.
Informed consent
Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work for the procedure(s) undertaken. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.