
Abstract
Objectives
The aim of this study was to determine the functional medium- to long-term outcome for cats with a conservatively managed sacroiliac luxation fracture (SILF).
Methods
Inclusion criteria were conservative management of SILF in cats with no other concurrent fractures of the pelvic weightbearing axis and availability of radiographs for review. Radiographic measurements of percentage displacement of the sacroiliac joint and the sacral index were obtained and fracture configuration was assessed. A specific owner questionnaire was completed a minimum of 6 months after the injury. The questionnaire assessed the ability of the cat to perform normal activities, the time to recovery, any behavioural changes and any requirement for long-term analgesia.
Results
Seventeen cats met the inclusion criteria, and 13 owners completed the questionnaire. Twelve cats had an excellent outcome, with no difficulty performing normal activities. One cat had a good outcome, with slight or occasional difficulty performing normal activities.
Conclusions and relevance
Our study provides evidence to support the current guidelines of conservative management of SILF. The inherent bias of case selection in our population implies that this treatment cannot be recommended for all cases of SILF.
Introduction
Pelvic fractures account for approximately 32% of all feline fractures, 1 and 59–93% of reported feline pelvic fractures are sacroiliac luxation fractures (SILFs), with 27–46% being bilateral.1–3 SILF is defined as separation of the iliac wing from the sacrum, 4 and can be associated with sacral fractures. 5 Unilateral SILF can only occur with concurrent pelvic fractures, owing to the rigidity of the pelvic box. 6 Frequent fracture combinations are SILF with pubic symphyseal separation, SILF with ipsilateral pubic and ischial fractures, 6 and SILF with contralateral ilial body and pubic fractures. 1 Even though bilateral SILF can occur without any concurrent pelvic injuries, 6 cats often have associated pubic fractures. 1
Some authors advise surgical stabilisation of all SILFs because the sacroiliac joint forms part of the pelvic limb weightbearing axis,7,8 and there is a lack of evidence to support conservative management of SILF.1,7 Indications for conservative management of SILF are patients being ambulatory, 6 displacement of <50% of the joint surface, minimal pain or instability, absence of concurrent fractures of the weightbearing axis, absence of neurological deficits and <45% narrowing of the pelvic canal.1,7,9,10
Conservative management of pelvic fractures in cats typically consists of cage rest for 2–4 weeks, analgesia, and monitoring of urination and defecation. 10 Con-servative management has been reported for SILF in cats,1,11 with a good outcome and absence of lameness at short-term follow-up (4 weeks) in a retrospective study of 16 cats. 11 Complications associated with conservative management of SILF include displacement of pelvic fragments leading to pelvic canal stenosis and obstipation or constipation, 12 and prolonged recovery. 7 Ankylosis of the sacroiliac joint as well as degenerative changes have also been suggested to occur and affect mobility. 13
Physical examination and assessment of pain are often more challenging in cats than in dogs. 14 Owner-based questionnaires reporting lifestyle alterations and changes in demeanour have been shown to correlate well with objective activity data in cats with osteoarthritis. 15 More recently, an owner-based questionnaire has been used to assess outcome in feline surgically stabilised unilateral and bilateral SILFs,16,17 and feline femoral head and neck excisions. 18 Objective gait analysis using force plates has been reported, but access to this resource is limited and often the data yield can be poor in cats owing to their unwillingness to walk on the lead or be guided. 19
The purpose of this study was to determine the medium- to long-term functional outcome for feline patients treated conservatively for SILF. Our null hypothesis was that cats conservatively managed for SILF would have a poor medium- to long-term functional outcome.
Materials and methods
Clinical records and radiographs of all cats admitted to the Scarsdale Veterinary Group, UK, with SILF from 2008 to 2018 were reviewed after ethical approval was obtained. Inclusion criteria were conservative management of SILF in cats with no other concurrent fractures of the pelvic weightbearing axis (ilium, excluding the ilial wing and acetabulum) and availability of radiographs for review. Cats treated conservatively that had a SILF with >50% displacement or a narrowing of the pelvic canal of >45% were excluded from the study. Cats with type I sacral fractures associated with the SILF were included in the study, while other types of sacral fractures were excluded. Any cat receiving surgical treatment for an orthopaedic condition was automatically excluded from the study, as was any cat with an additional conservatively managed fracture in the weightbearing axis of the pelvis. Retrieved data included signalment, neurological status on admission, fracture type (unilateral SILF vs bilateral SILF, with or without an associated type I sacral fracture), duration of hospitalisation, and concurrent orthopaedic and non-orthopaedic injuries.Radiographic evaluation included assessment of ventrodorsal and lateral pelvic radiographs to confirm the fracture configuration and to perform measurements of percentage displacement of the sacroiliac joint and the sacral index (SI). 20 The percentage displacement was determined based on the total length of the articular surface of the sacrum (a) and the length of the incongruence of the sacroiliac joint (b), using the formula (b/a) × 100, as previously reported (Figure 1). 17 In cases with bilateral SILF, the percentage displacement was recorded for the side with the largest displacement. The SI was determined from the ventrodorsal radiographs and defined as the ratio of the width of the sacrum at the cranial border to the width of the pelvic canal at the narrowest point, measured between the medial cortices of the acetabular bones (Figure 2). 20 The normal value for SI was 0.97 ± 0.025, as previously reported by Hamilton et al, 20 and pelvic narrowing was then expressed as a percentage, with <10% considered mild, 10–30% moderate and >30% severe narrowing.
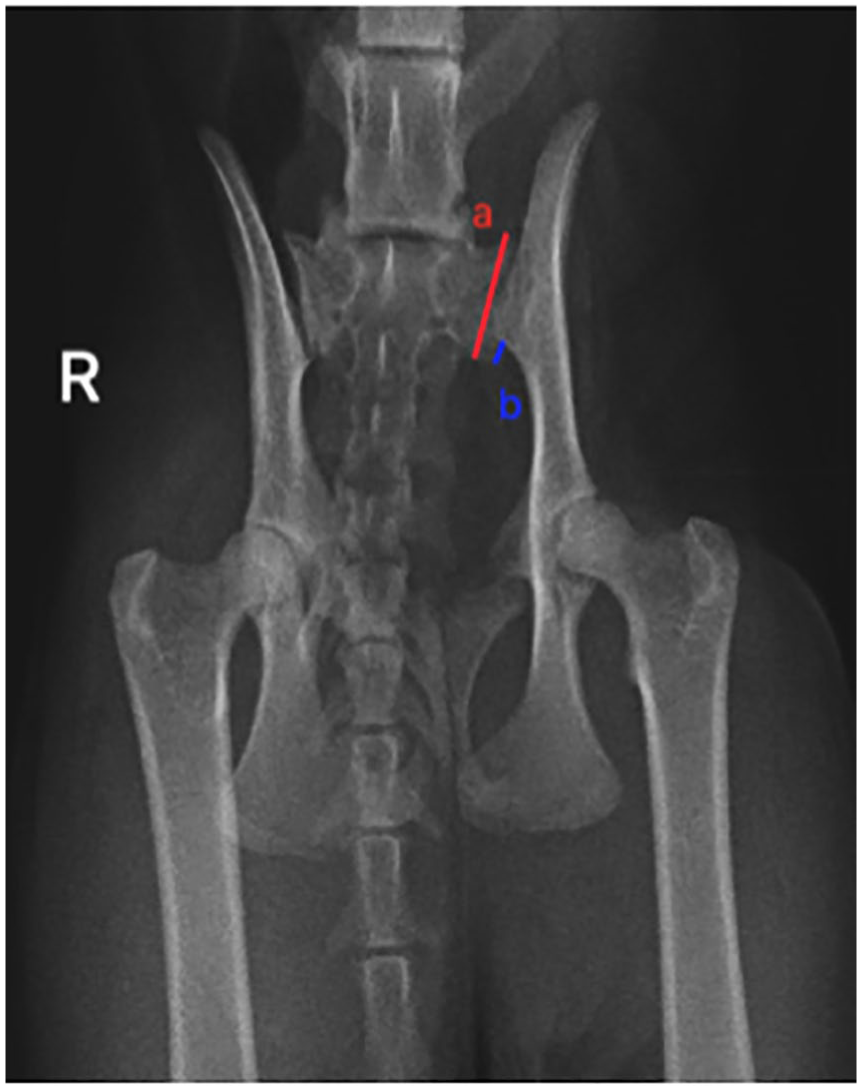
Ventrodorsal radiograph showing calculation of percentage displacement of the sacroiliac joint. ‘a’ indicates total length of the articular surface of the sacrum and ‘b’ indicates length of the incongruence of the sacroiliac joint

Ventrodorsal radiograph showing calculation of the sacral index. ‘S’ indicates the width of the cranial border of the sacrum and ‘A’ indicates the narrowest point of the pelvis measured between the medial cortices of the acetabular bones
A previously reported feline owner-based questionnaire was used and clients were contacted by telephone or post to assess the outcome for the cats treated conservatively for SILF. 18 The questionnaire was adapted from Yap et al18 to include specific questions regarding long-term urination and defecation abnormalities, but is unvalidated (see the supplementary material).
Information obtained included lifestyle changes and the cats’ abilities to perform normal activities. The seven activities (running, climbing, jumping up, jumping down, walking, playing and grooming) were graded from 0 to 4 with a descriptive, discontinuous scoring scale (see the supplementary material), giving a maximum score of 28. As previously reported, 18 an excellent outcome was defined as a total disability score of ⩽4 and a good outcome as ⩽8, with those cats having a slight difficulty in performing normal activities. In the lifestyle questions owners were asked about height of jump, demeanour, defaecation and urination, concurrent medical conditions, ongoing medication and concurrent orthopaedic conditions as dichotomous variables (‘yes’ or ‘no’). They were then finally asked about the time to recovery of normal activity. Clients were asked about current (medium- to long-term) abilities of their cats. Medium- to long-term was defined as a minimum follow-up of 6 months after the trauma. 21
Conservative management was defined as 4 weeks of cage rest following discharge from the hospital, analgesia (oral non-steroidal anti-inflammatories or buprenorphine), and monitoring of urination and defaecation.
Results
Signalment
A total of 56 cats were presented between 2008 and 2018 with SILF. Twenty-five cats underwent surgical stabilisation of their SILF and 31 cats were conservatively managed. Ten cats had surgical management of concurrent orthopaedic injuries (ilial fracture, acetabular fracture and coxofemoral luxation) and conservative management of the SILF. Twenty-one cats with no concurrent orthopaedic injuries had conservative management of their SILF. One of these cats had an abaxial sacral fracture and three cats had bilateral SILFs, with displacement >50%, leaving 17 cats that met the inclusion criteria. Of these, four cats were excluded because the owner was not contactable (n = 2) or declined participation (n = 2).Thirteen cats were, therefore, included in the study. There were 10 domestic shorthairs, one domestic longhair and two Bengal cats. Six were female and seven were male, and all were neutered. The median age at presentation was 30 months (range 12–103 months) and the mean ± SD body weight was 4.4 ± 1.22 kg. The results from our study are summarised in Table 1.
Summary of case details

These cats had type I sacral fractures
SILF = sacroiliac luxation fracture; SI = sacral index; DSH = domestic shorthair; MN = male neutered; FN = female neutered; DLH = domestic longhair
Radiographic assessment
There were three bilateral SILFs and 10 unilateral SILFs. The mean ± SD displacement of the sacroiliac joint was 20 ± 7.76% (median 20%, range 8–40%). The median SILF displacement for the bilateral group was 23% (range 20–25%) and for the unilateral group was 17.5% (range 8–40%). The mean ± SD SI was 0.935 ± 0.49. The mean ± SD SI for the bilateral group was 1.05 ± 0.58 and for the unilateral group was 0.9 ± 0.49. Three cats had an SI within the previously defined normal range (0.97 ± 0.025), one with a unilateral SILF, one with a unilateral SILF with a type I sacral fracture, and one with a bilateral SILF. Four cats had an increased SI, two with bilateral SILFs and two with a unilateral SILF. Four cats had mild narrowing of the pelvic canal (<10%), all with unilateral SILFs, and two cats had moderate narrowing (10–30%), both with unilateral SILFs. Mean pelvic canal narrowing was 3.47%. Two cats had concurrent type I sacral fractures, one with a left-sided SILF with 22% displacement and one with a left-sided SILF with 12% displacement.
Concurrent injuries
Three cats had concurrent injuries not affecting the weightbearing axis of the pelvis, including one abdominal wall rupture, one tail fracture at Cd1–Cd2 and one S3–Cd1 luxation. The cat with a tail fracture initially presented with reduced tail tone, but this resolved within 48 h. The cat with the S3–Cd1 luxation had a urinary catheter placed for initial bladder management, but regained tail tone and urinated voluntarily after 72 h. The abdominal wall rupture was managed surgically and full recovery was documented on the clinical records.
Initial presentation
While four cats were non-ambulatory on presentation, nine cats were ambulatory but lame. Two cats were presented at approximately 4 and 7 days after the trauma (cases 3 and 8), as they had been missing for that time; the rest were examined within 12 h of the trauma. One patient showed pelvic limb neurological deficits (case 8), having reduced withdrawal reflex and reduced muscle tone, and movement consistent with an L6–S1 localisation. This cat had a type I sacral fracture with 22% displacement of the sacroiliac joint.
All patients urinated voluntarily prior to discharge from the hospital. The median duration of hospitalisation was 2 days (range 1–5 days).
Follow-up
Medium- to long-term follow-up ranged from 9 to 116 months (median 48 months) and all cats were alive at the time their owner completed the questionnaire. The mean ± SD disability score (DS) was 0.85 ± 1.3, median 0 (range 0–5), with seven cats having a DS of 0. Twelve cats had an excellent outcome (DS ⩽4). One cat had a good outcome (DS ⩽8), with a score of 5 (case 9). The owner of the cat with a good outcome reported that there was a slight reduction in its speed of running, a reduced height of jump and that the cat was slightly stiff after rest. This cat had a bilateral SILF with 23% displacement and a concurrent body wall rupture. Two owners reported a reduced height of jump that had been present since the injury. One cat had a reduced height of jump that had started 36 months after the trauma (case 10) when the cat was 10 years old. Two cats were slower to jump down from a height (cases 3 and 5). All cats showed normal urination and defaecation. Two cats had altered behaviour, with owners reporting that they were less keen to go out. One cat with a unilateral SILF and an associated type I sacral fracture, with 22% SILF displacement and with neurological signs localised to L6–S1 on presentation, still had occasional loss of balance when walking on a narrow surface (case 8).No cats were on any long-term medication. Six cats took >2 months to fully recover, six cats took 1–2 months and one cat took <1 month.
Discussion
Our study has shown that cats treated conservatively for SILFs have an excellent (n = 12/13) or good (n = 1/13) clinical outcome, and therefore our null hypothesis was rejected.
In our study, only cases that met the previously described criteria for conservative management of SILF were included. The aim of this study was to provide objective data to support the current criteria for conservative management of SILF. The inclusion of multiple fracture configurations with small case numbers would have made the interpretation of the data challenging; for this reason, strict selection criteria were applied. There was one cat (case 8) where surgical stabilisation could have been indicated; this cat was showing neurological deficits following a 22% displaced unilateral SILF and a left sacral type I fracture; the cat was presented 7 days post-trauma and was ambulatory at that stage, so the clinical decision was to proceed with conservative management. Type I sacral fractures are defined as alar fractures originating adjacent to the juxta-articular notch and terminating at the articular surface of the wing of the sacrum. In a study by Anderson and Coughlan, 5 reviewing 17 cases of feline sacral fracture, type I fractures accounted for seven of the cases and in this series none of the cats had associated neurological signs. With our study, we eliminated all type II–V sacral fractures, but we included two cases with type I sacral fractures (cases 3 and 8).
Neurological deficits were noted in 3/13 of our cats on presentation, with suspected sciatic neuropraxia present in 1/13. This cat (case 8) had a unilateral SILF with 22% displacement and a concurrent type I sacral fracture. Two cats had tail injuries (cases 5 and 10), with reduced tail tone and in one cat a transient inability to urinate (case 10). Neurological signs have been reported in 23% of cats with pelvic fractures and sciatic dysfunction in 16%. 2 The lower incidence of sciatic injury in our population is likely to reflect our case selection for conservative management (ie, low SILF displacement). The cat with sciatic dysfunction had residual balance issues at 38 months after the trauma, which had been consistent since the injury. This may indicate residual neurological impairment, although this was not confirmed by a neurological examination. Postoperative sciatic injury has been reported in 13% of cases following stabilisation of pelvic fractures. 2 Meeson and Geddes reported that 3/43 cats with pelvic fractures had persistent neurological deficits at long-term follow-up. 2 This study represents a different population of cats to ours, but 24/32 of the surgically managed pelvic fractures did have surgical stabilisation of SILF. Long-term neurological signs have also been suggested to develop as a result of callus formation, 22 but these were not seen in our study.
In our study, occasional mild lameness was reported in two cats (cases 9 and 11); both had bilateral SILFs with 20% and 23% displacement, respectively. The owner of the cat with bilateral SILF and 23% displacement assigned a DS of 5 (case 9), and also reported some stiffness after rest and a reduced height of jump. Residual lameness has been reported in 9–33% of cats after surgical stabilisation of SILF with a lag screw. 3 This may be under-reported owing to the difficulty of assessing lameness in cats and the absence of a follow-up veterinary examination, 15 which may have detected more subtle lameness. 19 Owner-based questionnaires have been shown to correlate well with activity levels in cats. 15 In our study, two owners reported a reduced height of jump, with one cat having a bilateral SILF with 23% displacement (case 9) and one cat having a unilateral SILF with 40% displacement (case 10). Two owners reported that their cats were slower to jump down (cases 3 and 5); both cats had unilateral SILF with 8% and 12% displacement, respectively. A reduced height of jump and an unwillingness to jump down from a height may indicate some degree of pain in these cats, although their DSs were 5 and 2, respectively, in the reduced height of jump and 1 in the slower-to-jump-down category. Trial treatment with non-steroidal anti-inflammatory drugs and repeated owner assessment could have been used to further assess if these cats were in pain. 15 No cats received long-term analgesia and all owners were satisfied with the clinical outcome of their cats.
Sacroiliac joint ankylosis and degenerative joint disease are thought to develop after conservative management of SILF. 13 The absence of follow-up radiographs prevents the diagnosis of these conditions in our study. However, an excellent outcome in 12/13 cats and a good outcome in the remaining cat suggest that, if present, it did not cause any significant disability.
In our population, the mean SI was 0.935, which is similar to the findings reported by Hamilton et al 20 for normal cats and those following surgical stabilisation of ilial fractures. There is no defined SI at which surgery is indicated and a pelvic canal narrowing of ⩾45% is still used as the measurement at which surgery is recommended. 2 The absence of follow-up radiographs does not allow assessment of the SI after healing, but no cats in our study had reported problems with defecation. Previous studies have suggested that following conservative management of pelvic fractures the degree of pelvic deformity persists and bones stabilise in their displaced position. 11 Hamilton et al 20 reported a mean decrease in pelvic canal diameter following plating of ilial fractures. A narrowing of >45% has been associated with obstipation or constipation, 20 and these clinical signs were not seen in our population.
Reduction in pain, faster return to function and maintenance of the width of the pelvic canal are all potential advantages of surgical stabilisation of SILFs.18,23–25 Owing to the absence of accurate short-term follow-up and a control population, we are not able to determine if a greater level or a greater duration of discomfort was present in the recovery period for this population of cats vs cats with surgically managed SILFs. In our study, all cats returned to excellent/good function at medium- to long-term follow-up. Six cats took >2 months to fully recover.
The limitations of this study include its retrospective nature, the relatively small case numbers, variation in the injury sustained, the subjective medium- and long-term follow-up information obtained by the owner questionnaire, the use of an unvalidated owner questionnaire and the absence of long-term veterinary examination or radiographic follow-up.
Conclusions
In this population of cats, conservative management of unilateral and bilateral SILFs produced an excellent-to-good outcome. Our study supports the current guidelines for the conservative management of SILF. The inherent bias of case selection in our population implies that this treatment cannot be recommended for all cases of SILF.
Supplemental Material
Supplementary Material
Owner-specific questionnaire
Footnotes
Supplementary material
The following file is available online: Owner-specific questionnaire.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Nottingham University (2701 190226).
Informed consent
Informed consent was obtained from all clients prior to inclusion of their cats in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.