
Abstract

Johann Schönlein coined the term ‘tuberculosis’ in 1834, 48 years before the causative agent Mycobacterium tuberculosis was first visualised by Robert Koch. At that time, one in seven of the world’s human population was thought to be infected. Despite significant efforts in the intervening almost 200 years, this prevalence has actually increased to an estimated one in three. While M tuberculosis may have been the first tuberculous organism identified, it is restricted to infecting a very small number of species. By comparison, the causative agent of ‘zoonotic tuberculosis’, Mycobacterium bovis, has a very wide host range. So named for its predilection for bovine hosts, M bovis can actively infect an exceptionally broad range of species including, but not limited to, cattle, badgers, deer, camelids, a variety of rodents, human and non-human primates, raccoons, possums and coyotes. Not surprisingly, our feline patients are also susceptible.
Last year, we were alerted to a highly unusual group of feline M bovis tuberculosis cases.1,2 Initially, the striking feature was that these cases presented with a rare manifestation of disease – alimentary tuberculosis (Figure 1). This contrasts with most ‘typical’ cases of tuberculosis in cats in the UK, which are cutaneous and/or pulmonary. The investigation became even more complex when diagnostic tests confirmed M bovis infections; this was unexpected as these cats were living in areas of the UK that either have a very low prevalence of M bovis in cattle and badgers (such as Lancashire) or are officially M bovis free (such as Scotland).
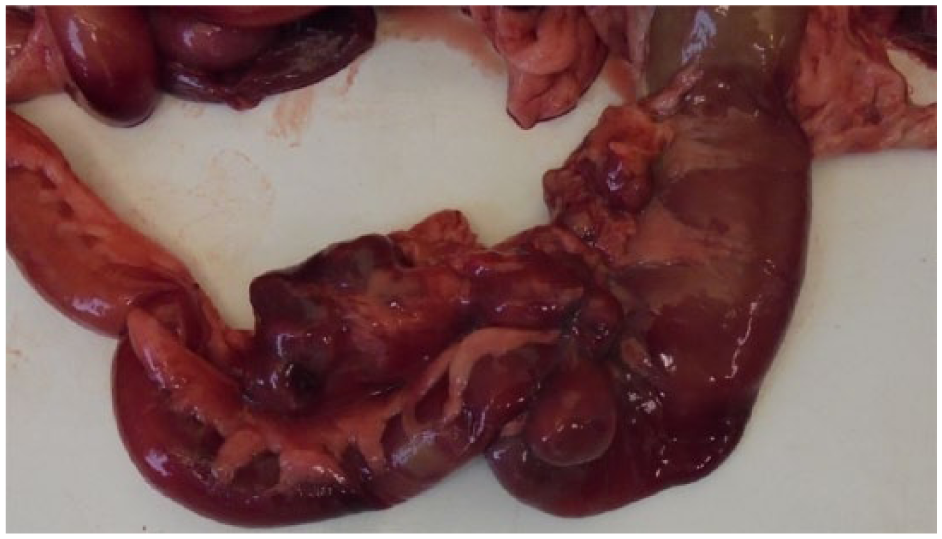
Grossly abnormal intestine and associated lymph nodes removed for specialist mycobacterial culture from a 1-year-old male neutered Persian cat that was weaned onto the Natural Instinct Wild Venison product and continued to eat it as a sole ration until developing marked chronic weight loss, hyporexia and an expiratory wheeze. This cat was euthanased on welfare grounds due to the severity of its clinical signs
We investigated the lifestyle histories of the cases to try to identify any possible routes of exposure to M bovis. We discovered that all of the cats were indoor-only (ie, they were at negligible risk from wildlife or rodents), they were of different breeds and were mostly young, and none had been fed raw (unpasteurised) milk or lived with people with active tuberculosis. The only common feature was that all were fed (in varying proportions) a commercial raw food diet: Natural Instinct Wild Venison (Figure 2). On discussion with the company, and from their subsequent investigations, it transpired that some of the ingredients had not been meat-inspected in line with EU requirements so the safety of the product could not be confirmed; the company voluntarily recalled the food,3 and its venison product has since been discontinued.

The venison product (now discontinued) linked to this outbreak
The EU requirements in question (principally EU Regulation 853/2004 4 ) state that a wild venison carcase (including its gralloch, or innards) must be inspected by a trained person (which can be the stalker) after the deer’s death to look for any signs of disease, parasites or contamination. However, the stalker does not have to bring the gralloch ‘off the hill’, so infections could be missed. In addition, the supply by hunters of small quantities of wild game meat directly to local retailers is not covered by these regulations and therefore is not subject to any of the defined rules for food of animal origin.
In this case, possible contamination could have been avoided if this Regulation had been correctly adhered to. However, in order to reduce the risk of a similar incident occurring in the future it is our view that examination of entire game carcases (including the gralloch) should be undertaken by a qualified, specially trained veterinary surgeon in an abattoir if the meat from the carcase is intended for consumption as a raw food product (for either people or pets). Within the UK, such a policy change could be applied across England and Wales, or limited to the high-risk and edge areas (ie, buffer zones between high- and low-risk areas) for endemic M bovis infections in cattle and wildlife. Additionally, we feel it would be sensible to prevent the feeding of raw offal to any companion animal. This policy is already in effect for packs of hounds; since October 2017, the feeding of offal from livestock species to packs of hounds has been banned in England following our previous work investigating another raw food-associated M bovis outbreak, and no new cases have since been reported.5,6
Our initial investigation into this current outbreak is reported in this issue of JFMS, 2 and since the writing of this article new cases have continued to occur. To date we have diagnosed 45 cases with active clinical disease and 73 with inactive (ie, latent) infection, and screened in excess of 50 clinically well, test-negative cats where owners were concerned regarding historical exposure to the contaminated product. A more up-to-date report of our findings is in preparation and will be published as soon as possible.