
Abstract
Practical relevance:
Abdominal ultrasound plays a vital role in the diagnostic work-up of many cats presenting to general and specialist practitioners. Although hepatic vascular anomalies are less common than disorders of the hepatic parenchyma and biliary tree, our understanding and recognition of these is gradually increasing with advancements in ultrasound technology and image quality.
Clinical challenges:
Despite ultrasonography being a commonly used modality, many practitioners are not comfortable performing an ultrasound examination or interpreting the resulting images. Even differentiating between normal variation and pathological changes can be challenging for all but the most experienced. In addition, some views may be obscured by overlying structures; for example, the termination of a shunt entering the left phrenic or azygous veins is often difficut to see due to the high probability of lung passing between the shunt and the transducer as the cat breathes.
Equipment:
Ultrasound facilities are readily available to most practitioners, although use of ultrasonography as a diagnostic tool is highly dependent on operator experience.
Aim:
This review, part of an occasional series on feline abdominal ultrasonography, discusses the appearance of various hepatic vascular anomalies. It is aimed at general practitioners who wish to improve their knowledge and confidence in feline abdominal ultrasound and is accompanied by high-resolution images. Ultrasound of the liver and biliary tree were discussed in articles published in January and May 2019, respectively.
Evidence base:
Information provided in this article is drawn from the published literature and the author’s own clinical experience.
Keywords
Compared with disorders of the hepatic parenchyma and biliary tree, hepatic vascular anomalies are somewhat less common in the cat. However, as ultrasound technology and image quality continue to improve and our understanding of vascular abnormalities grows, recognition of these disorders is gradually increasing.

Portosystemic shunts
Portosystemic shunts (PSSs) are abnormal vascular connections between the portal system and systemic venous circulation that allow blood to bypass the liver. 4 They may be congenital or acquired, the former being more common in cats.
Congenital portosystemic shunts
Although congenital PSSs are a well-recognised cause of hepatic encephalopathy, they occur far less commonly in cats than in dogs. 5 The use of ultrasonography for the diagnosis of PSSs in both species has been described in detail and only features pertinent to cats are discussed here.6-11 For further information regarding the expected laboratory results, options for surgical management and prognosis in cats with a congenital PSS, readers are referred to two earlier reviews in JFMS by Tivers and Lipscomb.12,13
Congenital PSSs have been reported in both domestic shorthair cats, which account for the majority of cases, and purebred cats, particularly Siamese, Himalayans, Burmese and Persians.5,6,12,14-17 While the majority of cats are presented for investigation of a suspected shunt when less than 12 months of age,6,18 shunts can remain undetected for many years.12,17 Cats with congenital shunts can be normal in size and stature or small and in poor condition, and often present with neurological signs.5,6,15,17
Congenital shunts can be subdivided into those that are located outside the liver (extrahepatic) and those located inside the liver (intrahepatic).
Congenital extrahepatic shunts
Single extrahepatic shunts are more common in cats than intrahepatic shunts, although both have been reported.9,6,17,19,20 Extrahepatic shunts in cats can be divided into five subtypes: left gastrophrenic, left gastrocaval, splenocaval, left gastroazygous and those arising from the left colic vein, with the first three accounting for 92% of shunts in this species (see box below for imaging guidelines and interpretation).22,23
A shunt arising from the left gastric vein is recognised on ultrasound as a large vessel entering the gastrosplenic vein from a cranial direction, usually close to where the latter enters the main portal vein. The shunt, which is often tortuous in nature, can sometimes be followed to its termination in the left phrenic vein, pre- or post-hepatic caudal vena cava (CVC) or azygous vein. In cats with a left gastrophrenic shunt (by far the most common subtype), the anomalous shunting vessel enters the left phrenic vein at the level of the oesophageal hiatus.22,24 It may be possible to follow the dilated left phrenic vein with ultrasound as it travels lateromedially along the caudal surface of the diaphragm before entering the post-hepatic CVC. 24 In cats with a left gastrocaval shunt, the anomalous vessel enters the post-hepatic CVC at the level of the caval foramen, often via a saccular dilation or ampulla, which may be recognised ultrasonographically. 24 As mentioned in the box above, in those cats with a splenocaval shunt, the shunting vessel terminates in the pre-hepatic CVC at the level of the epiploic foramen.24,26 Local disruption to flow resulting in turbulence may be noted in the cava at the site of entry of a shunt (Figure 3).


To image the portal vein starting at the confluence of the cranial and caudal mesenteric veins, the transducer is placed on the right flank with the cat in left lateral recumbency

Colour Doppler ultrasound image depicting normal flow in the portal and gastrosplenic veins. The blue colour in the portal vein confirms that the direction of blood flow is from caudal to cranial (ie, hepatopetal), or from right to left in this image. The red colour in the gastrosplenic vein is consistent with flow towards the transducer and thus flow into the portal vein

Ultrasound image showing altered flow within the caudal vena cava at the level of shunt entry. A colour flow Doppler window has been applied over the cava. In the right side of the window, flow in the cava is depicted as being blue, indicating that flow is away from the transducer and therefore from right to left (or caudal to cranial) in the image, as expected. In the left side of the window, the solid blue colour has been replaced with a mosaic of several colours including red, yellow, blue and cyan. According to the colour map on the left side of the image, this indicates that flow is directed both towards and away from the transducer, which is the typical appearance of turbulence
The presence of a large diameter vessel adjacent to the aorta in the craniodorsal abdomen, containing cranially directed blood flow, is consistent with a left gastroazygous shunt. 9 It should be noted that the normal azygous vein is not seen on ultrasound in cats. 10 It is often difficult to see the termination of a shunt entering the left phrenic or azygous veins due to their inherently cranial location within the abdomen and the high probability of lung passing between the shunt and the transducer as the cat breathes.
The left colic vein is a tributary of the caudal mesenteric vein. Shunts arising from the left colic vein can be identified on ultrasound by the presence of a large vessel containing hepatofugal flow that enters a distended caudal mesenteric vein (Figure 4). 23 An interesting feature of left colic shunts is that they often travel caudally before making a 180° turn to enter the systemic venous circulation via either the CVC or common iliac vein. 23
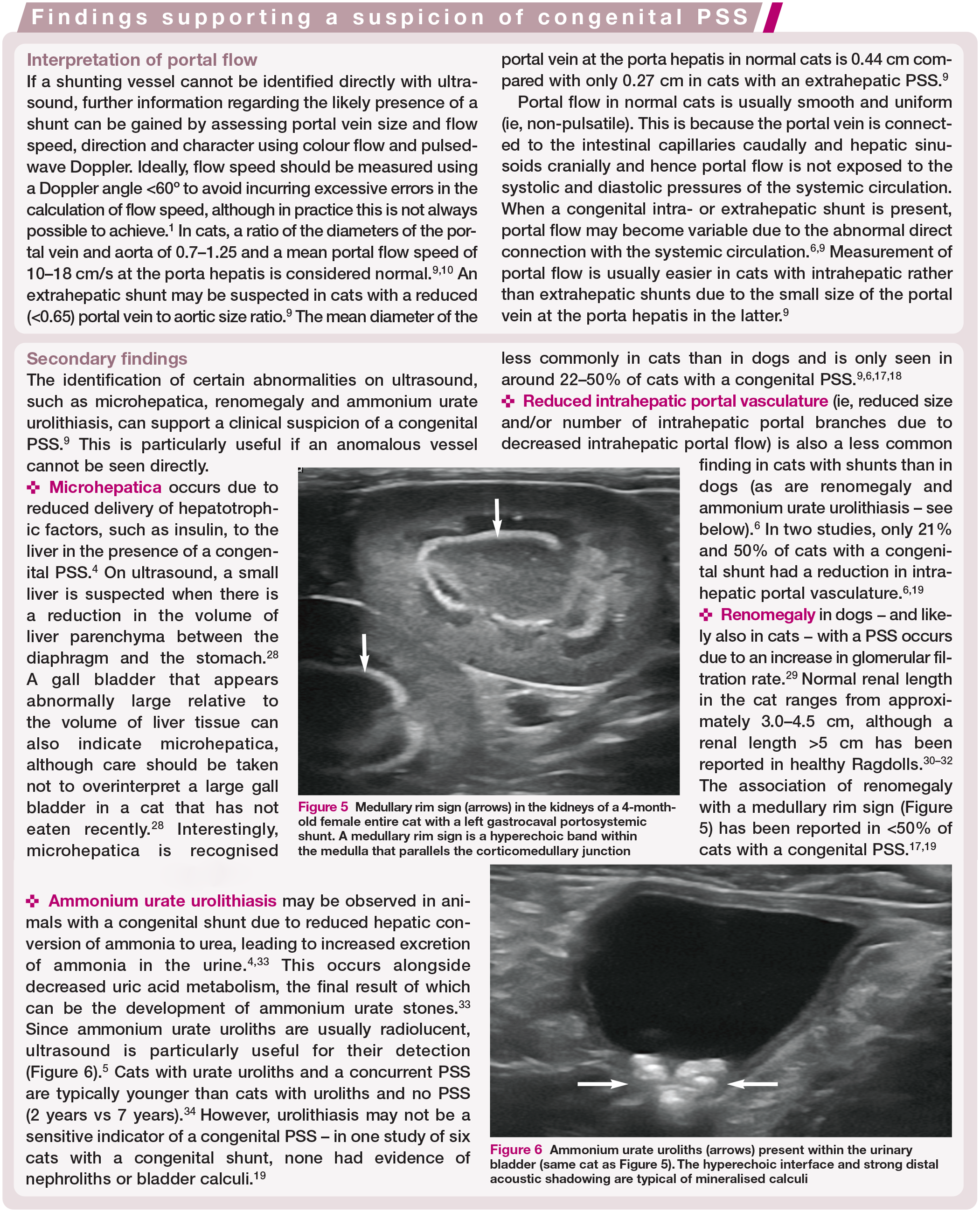
Ultrasound images from a 5-month-old male entire domestic longhair cat with an extrahepatic shunt originating from the left colic vein and terminating in the caudal vena cava (CVC). (a) Image acquired at the level of the confluence of the cranial and caudal mesenteric veins. The diameter of the shunting vessel is much greater than that of the portal vein (PV). (b) Colour Doppler image at the same level as (a) shows abnormal hepatofugal flow in the portal vein cranial to the shunt and within the shunting vessel itself, as denoted by the arrows. As the shunt was followed caudally (c,d), it formed a large, tortuous vessel containing hepatofugal flow (ie, directed from left to right in the images). (e) Focal dilation of the CVC (arrows) at the entry site of the shunt
Congenital intrahepatic shunts
As previously stated, intrahepatic shunts occur less commonly than extrahepatic shunts in the cat. Most intrahepatic shunts in cats are left divisional, although both right- and central-divisional shunts have also been reported. 18 Ultrasound can be used preoperatively to accurately characterise intrahepatic shunts as left, right or central divisional. 18
As in the dog, left-divisional shunts in cats are thought to represent a patent ductus venosus and arise from the left branch of the intrahepatic portal vein, forming a large-diameter vessel, initially travelling cranio-laterally through the left side of the liver before coursing medially to drain into the CVC via the left hepatic vein.18,27 Right-divisional shunts in the cat can similarly present as a large tortuous vessel but are located within the right side of the liver, rather than the left. 27 In dogs, central-divisional shunts are usually formed from a foramen between the intrahepatic portions of the portal vein and CVC, whereas in the cat they take the form of a tortuous intrahepatic vessel. 27 The use of a right or left craniodorsal intercostal and/or subcostal approach is often necessary to identify the intrahepatic shunt ultrasonographically. 9
The ability to identify and follow any shunting vessel will depend not only on operator experience but also on patient cooperation and the extent of any gas within the gastrointestinal tract, which can obscure important anatomy. Therefore, while the ‘shunt hunt’ can be performed with the patient conscious, it is often preferable to use sedation.

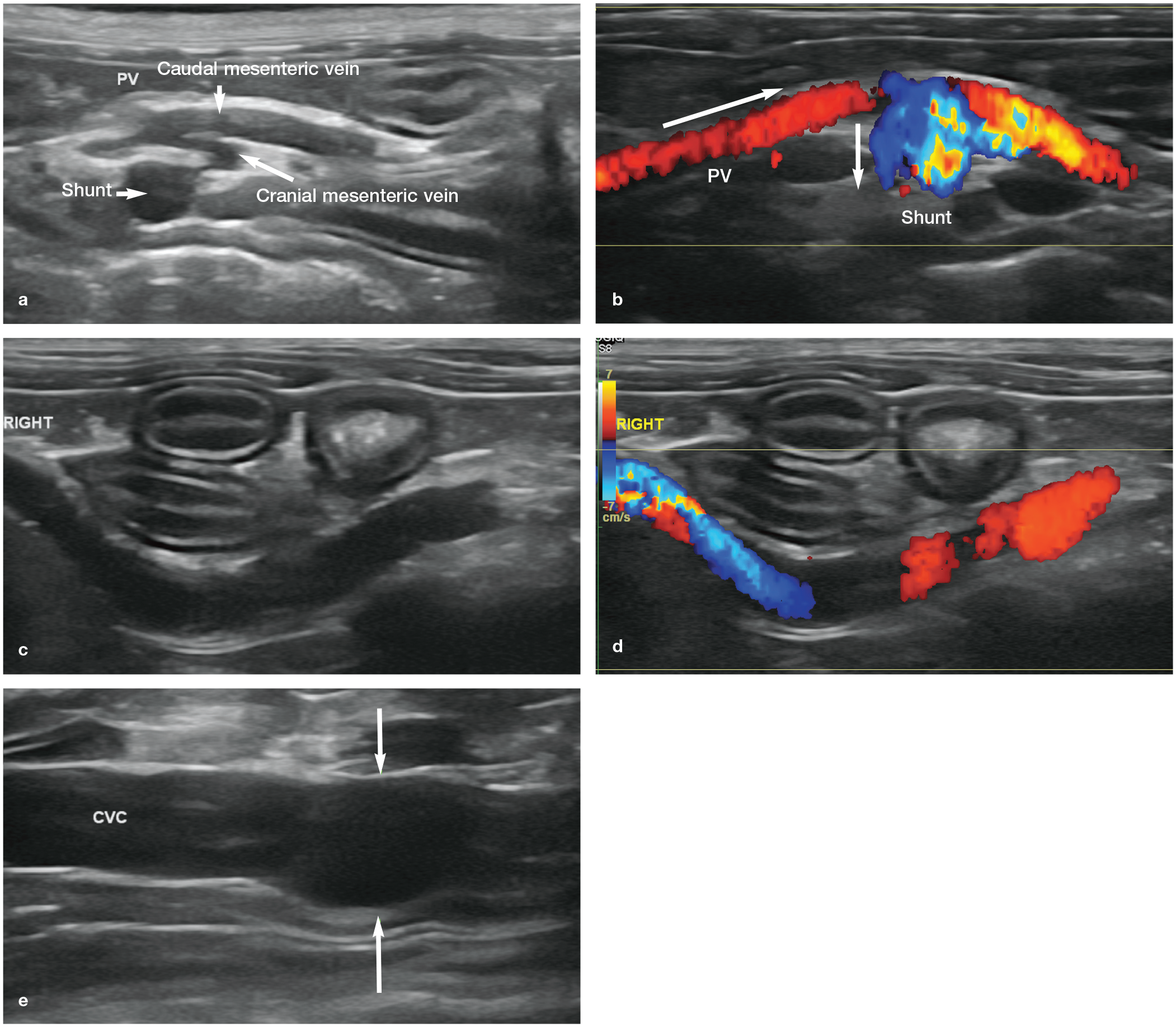
Medullary rim sign (arrows) in the kidneys of a 4-month-old female entire cat with a left gastrocaval portosystemic shunt. A medullary rim sign is a hyperechoic band within the medulla that parallels the corticomedullary junction

Ammonium urate uroliths (arrows) present within the urinary bladder (same cat as Figure 5). The hyperechoic interface and strong distal acoustic shadowing are typical of mineralised calculi

Acquired portosystemic shunts
Acquired shunts are pre-existing embryonic vessels that open up and dilate in response to chronic portal hypertension to allow blood to bypass the liver and enter the systemic circulation directly. The prevalence of acquired portosystemic shunting in cats as a result of portal hypertension is low and only occasional reports exist.35-42 This may be at least in part attributable to the relatively low prevalence of cirrhosis in this species, which is a common cause of acquired shunts in the dog. 39 Acquired shunts have been reported to occur in cats in association with several conditions including hepatic fibrosis,39,41 arterioportal fistulae,37,43 portal vein thrombosis 37 and chronic diaphragmatic herniation, 40 and also as a sequela to surgical attenuation of a congenital PSS.44,45
Although reports of the ultrasonographic appearance of secondary acquired shunts in cats are also rare, acquired shunt morphology appears to mirror that seen in dogs. Acquired shunts can take the form of one or more plexuses of small tortuous vessels in the retroperitoneal space close to one or both kidneys or between the portal vein and CVC (Figure 7).39,40 A peritoneal effusion of variable volume is also commonly found in cats with acquired PSSs. 39
The presence on ultrasound of an acquired shunt taking the form of a solitary abnormal vessel containing hepatofugal flow that originated from the portal vein close to the splenic vein has also been described in two cats with clinical signs of hepatic encephalopathy. 41 In both cases, liver histology revealed congenital hepatic fibrosis, a condition that arises due to congenital biliary cystic lesions and has previously been linked with polycystic kidney disease in cats. 46 The authors of the case report concluded that the congenital liver disease most likely resulted in portal hypertension and the formation of acquired portosystemic collaterals. 41

(a,b) Colour flow Doppler images showing the typical ultrasonographic appearance of acquired shunts that have formed secondarily to portal hypertension. Small vessels such as these are usually best appreciated with colour flow Doppler and can be surprisingly difficult to identify in B-mode grey scale images
Splenosystemic shunts
A separate category of shunt that has been described in predominantly older, spayed female cats is the splenosystemic shunt. 47 It is thought that splenosystemic shunts most likely represent either acquired shunts resulting from previous or current portal hypertension or they are congenital shunts of uncertain clinical significance. 47
On ultrasound, a splenosystemic shunt usually takes the form of a single anomalous vessel that originates from the splenic vein and follows a tortuous course either caudal to the left kidney before entering the left renal vein or CVC adjacent to the renal vein, or continues medial to the left kidney. In some cats, while the shunt may start and end as a single vessel, it can also form a plexus of smaller vessels at some point along the way. Of 33 cats with a splenosystemic shunt identified using ultrasound, 42% also had a hepatopathy that could potentially have resulted in portal hypertension. 47 Three cats had hepatopetal portal flow with a flow speed <10 cm/s and one cat had hepatofugal portal flow, suggestive of portal hypertension. Ascites was also identified in 10 cats.
Splenosystemic shunts have additionally been observed in abdominal radiographs of cats and create what is now referred to as a ‘spaghetti sign’. 48 The typical radiographic appearance is that of a well-defined, tortuous, tubular structure of soft tissue opacity within the left mid-abdominal cavity, lateral to the left kidney and caudal to the spleen. 48


Selected transverse plane computed tomography angiography (CTA) images of the abdomen of a 4-month-old domestic shorthair cat with an extrahepatic left gastrophrenic portosystemic shunt. All images are displayed in a soft tissue window (window level 40; window width 440), were acquired following the administration of iodinated intravenous contrast and are presented in caudal-to-cranial order. The patient’s right-hand side is to the left of the image. (a) Within the cranial abdomen, the portal vein (PV) is visible in the normal location ventral to the caudal vena cava (CVC), just to the right of midline. (b) A short distance cranial to this, the gastrosplenic vein joins the PV from the left (not shown). A large vessel (the shunt) emerges from the gastrosplenic vein at the expected location of the left gastric vein and is located to the left of the PV at this level. Note that the shunt is much larger in diameter than the PV. (c,d) The shunting vessel travels cranially and slightly dorsally within the abdomen, medial to the gastric fundus. (e,f) At the level of the diaphragm, the shunt joins with the left phrenic vein, which runs along the abdominal side of the diaphragm before draining into the post-hepatic CVC. Additional findings identified in the same CTA study included microhepatica and urolithiasis. GB = gall bladder; Ao = aorta
Portal vascular abnormalities
Arterioportal fistulae
An intrahepatic arterioportal fistula is an abnormal communication between a hepatic artery and a portal vein within the liver and can be congenital or, less commonly, acquired. 42 Intrahepatic arterioportal fistulae are extremely rare in the cat and only three cases have been reported to date.37,42,43 The ultrasonographic appearance appears to be very similar to that seen in dogs with the same condition (Figure 9).37,42,53 All three cats were 18 months of age or younger at the time of diagnosis.
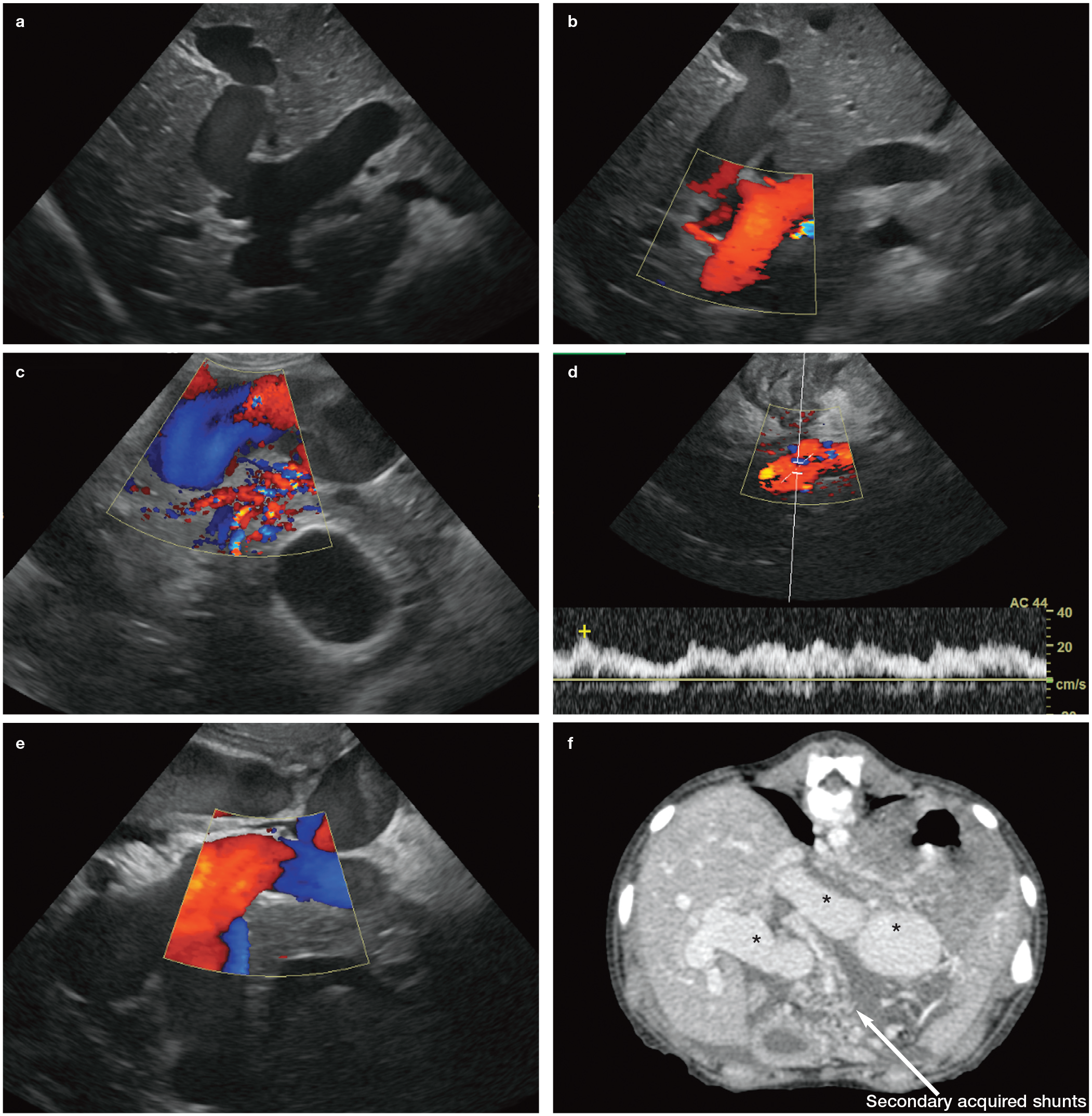
(a) Ultrasound image of a large tortuous vessel representing a congenital arterioportal fistula in the liver of a 4-month-old Golden Retriever puppy. The vessel could be traced from the coeliac artery to the point where it joined the left branch of the portal vein. (b) Colour flow Doppler confirms the presence of blood flow within the vessel, which in this case is directed towards the transducer. (c) In a different region of the liver, a plexus of multiple tiny vessels is present within the hepatic parenchyma below the fistula. These were barely visible on B-mode grey scale images. The gall bladder is visible in the bottom right of the image. (d) Colour flow and pulsed-wave Doppler interrogation of the portal vein shows that flow is hepatofugal (ie, away from the liver), turbulent, pulsatile and travelling at a higher speed than normal. (e) Multiple loops of a dilated anomalous blood vessel within the liver of a 2-month-old Labrador Retriever puppy that also had a congenital arterioportal fistula. (f) Single slice transverse plane computed tomography angiography image through the cranial abdomen of the same dog as in (e). The image is displayed in a soft tissue window (window level 40; window width 440) and was acquired following the administration of iodinated intravenous contrast. Multiple loops of a large tortuous vessel representing an arterioportal fistula are observed within the cranial abdomen (asterisks) and liver. Throughout the abdomen, numerous plexuses of much smaller tortuous vessels are present, consistent with the formation of secondary acquired shunts. A moderate volume of peritoneal fluid is also visible and likely to be the result of portal hypertension
Abdominal ultrasonography was performed on two cats and in both cases revealed ascites and dilation of an intrahepatic portal vein branch containing turbulent pulsatile flow on colour Doppler images.37,42 In one of the cats, an enlarged coeliac artery could be followed with ultrasound from its origin at the aorta to its communication with the dilated portal vein branch. 37 Doppler interrogation of this cat revealed hepatofugal pulsatile flow of abnormally high speed within the main portal vein, which was dilated. 37 Portal flow with these characteristics can be explained by the presence of high-pressure arterial blood flowing into the low-pressure portal system, increasing pressure in the latter and ultimately resulting in portal hypertension. Acquired PSSs arising secondarily to portal hypertension and involving the left renal vein were also identified in both cats.37,42
Portal vein aplasia
Portal vein abnormalities are uncommon in the cat. A single case of congenital absence of the portal vein has recently been reported in a 9-month-old female neutered domestic shorthair cat. While this was suspected on abdominal ultrasound, CTA was necessary for confirmation of the diagnosis. 54
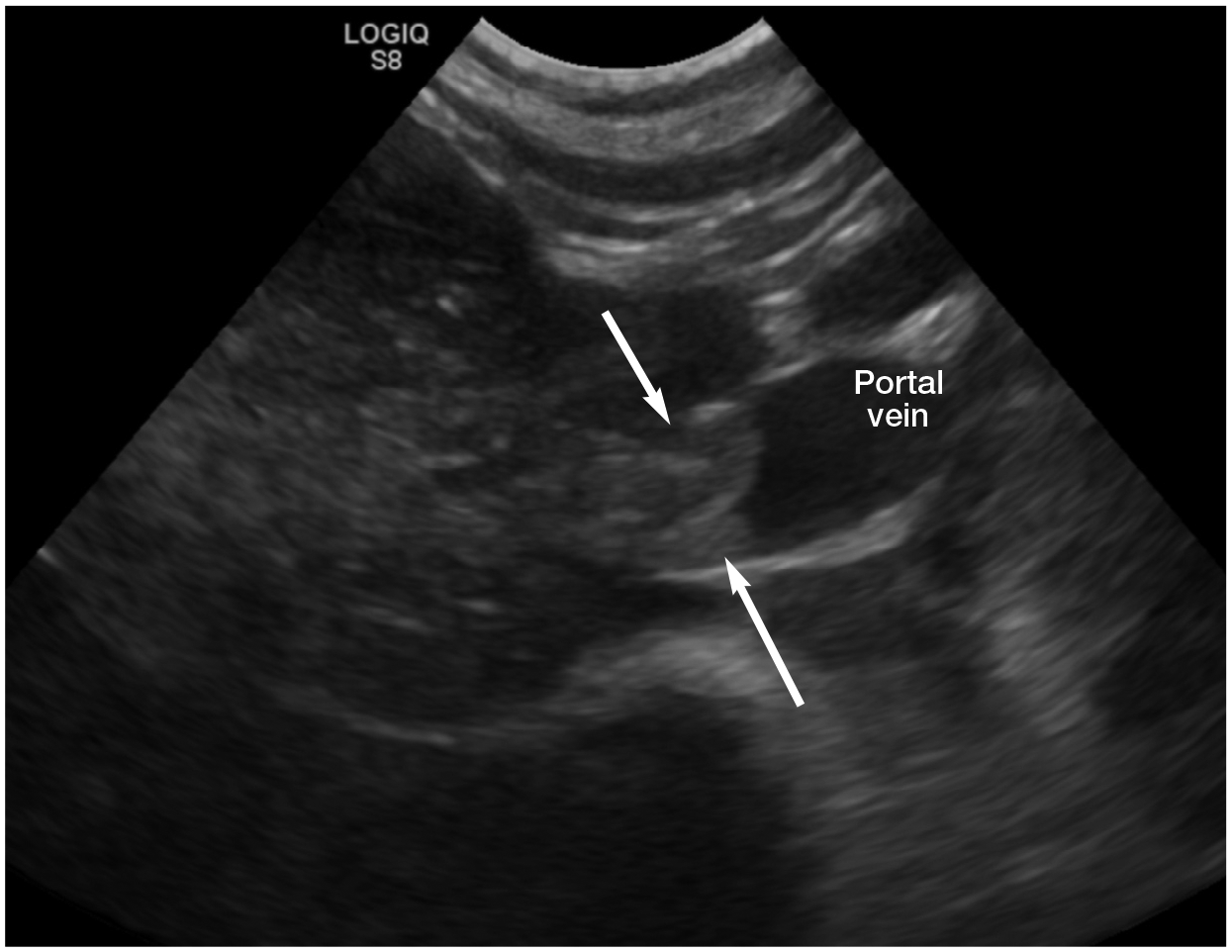
Echogenic thrombus (arrows) obstructing the portal vein of a 4-year-old male neutered Siamese cat with lymphoma
Portal vein thrombosis
Thrombosis of the portal vein can result from vascular stasis, damage to the vessel endothelium or a hypercoagulable state and is a rare cause of portal hypertension in the cat. 55 To date, only seven cases of portal vein thrombosis in cats have been reported in the literature.37,56 Six had evidence of hepatobiliary disease and the remaining cat had raised liver enzymes and hyperthyroidism.37,56 Abdominal ultrasonography was performed in all seven cases. In five cats, the portal vein thrombus had an echogenic appearance on ultrasound, and in the sixth cat reduced blood flow was identified in the renal, splenic and portal veins. 56 In the remaining cat, a hypoechoic mass, presumed to be a thrombus, was identified within the main portal vein; 37 the mass completely filled the lumen of the portal vein and caused mild focal dilation of the vessel. In four of these cats, colour flow Doppler was also used to confirm reduced or absent flow within the portal vein thrombus, and in two cats small plexuses of tortuous vessels, representing secondary acquired shunts, were visible in the region of the portal vein or left kidney.37,56
Thrombi vary in echogenicity depending upon their age and this could explain the variation in appearance of the portal vein thrombi described in these cats. A recently formed thrombus can appear almost anechoic and may be missed without the use of colour flow Doppler. 57 A chronic thrombus, on the other hand, is more likely to be visible with B-mode ultrasound due to its echogenic appearance relative to blood (Figure 10). 57
Key Points
Extrahepatic portosystemic shunts are more common than intrahepatic shunts in cats. The majority arise from the left gastric vein and are best appreciated using a right flank or intercostal window.
Most intrahepatic shunts in the cat are left divisonal and form a large tortuous vessel that runs through the left side of the liver and drains into a hepatic vein.
Acquired shunts are rare in the cat, but when they do occur they often take the form of a retroperitoneal plexus of tiny vessels that directly links the portal and systemic venous systems. Colour flow and/or power Doppler are usually necessary to confirm their presence on ultrasound.
Splenosystemic shunts are typically found in older female cats and present as a long vessel containing hepatofugal flow, running between the splenic vein and a systemic vein – usually either the left renal vein or the CVC.
Arterioportal fistulae are extremely rare in the cat but should be suspected if a large tortuous vessel is identified within the liver (the main differential being a congenital intrahepatic shunt). Typical features on ultrasound include pulsatile hepatofugal flow of high velocity within the portal vein, ascites and multiple acquired shunts.
Portal vein thrombosis has been reported in the cat. The ultrasound appearance depends on the age of the thrombus, with chronic thrombi typically having an echogenic appearance.

Footnotes
Conflict of interest
The author declares no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.