
Abstract
Objectives
The aim of this study was to describe the anaesthetic management and perianaesthetic complications encountered during hypophysectomy surgery in acromegalic cats. We explored relationships between animal demographic data, the anaesthetic protocol used and presence of perioperative complications.
Methods
Cats having undergone hypophysectomy surgery for the treatment of feline acromegaly at a single veterinary referral hospital were identified from hospital records. The anaesthesia records and clinical notes of these animals were retrospectively reviewed. Descriptive statistics were produced and binary logistic regression run to assess for any relationship between patient factors, anaesthetic management and complications during the perioperative period.
Results
Perianaesthetic complications identified included hypothermia, hypotension, bradycardia and airway obstruction. Mortality at 24 h post-anaesthesia was 8%. The use of alpha (α)2 agonists was associated with a lower incidence of hypotension. Fentanyl infusion was associated with a higher incidence of airway obstruction compared with remifentanil. Subjectively assessed anaesthetic recovery quality had an association with the number of days spent in the intensive care ward postoperatively.
Conclusions and relevance
The anaesthetic management described seems effective for hypophysectomy surgery in cats. Intraoperative complications were common and, while not apparently associated with 24 h patient outcome, drugs and equipment to manage these complications should be available.
Introduction
Hypersomatotropism is an endocrine disease of cats that is becoming increasingly diagnosed. It is unclear whether this increase is due to an improving awareness of the condition, 1 a reflection of a true increase in prevalence in the domestic cat population or a combination of both. The disease is caused by a growth hormone-secreting pituitary gland adenoma. 2 In addition to causing the hypertrophy of soft tissues and cartilaginous structures typically seen in acromegaly, the excessive levels of growth hormone associated with the disease have significant impacts on a number of metabolic pathways, most notably decreasing insulin sensitivity resulting in refractory hyperglycaemia. One study found the prevalence of hypersomatotropism in diabetic cats to be 26%. 3 Although rare owing to the slow-growing nature of the adenoma, signs of neurological disease are possible. 4 These effects together can reduce the animal’s quality of life and also means that animals presenting for hypophysectomy often have comorbidities.
Traditionally, these cases have been managed medically or with radiation therapy, 5 but more recently, surgical removal of the tumour is being offered by some veterinary hospitals. This involves an intraoral approach through the soft palate and skull base to expose and resect the pituitary gland.6,7
Presumably owing to the relative novelty of the surgical procedure in cats, no data could be found in the veterinary literature regarding the anaesthetic management of these cases. The aim of this retrospective study was therefore to describe the anaesthetic management and complications encountered during hypophysectomy surgeries at a single veterinary referral institution between 2012 and 2016, to assess any relationship between these complications and the anaesthesia protocol used and the impact of anaesthetic management and presence of complications on the perioperative outcome. We hypothesised that the presence of intraoperative complications would have a negative impact on perioperative morbidity and mortality. While the term hypersomatotropism is most appropriate for describing increased levels of growth hormone, and acromegaly for the physical changes associated with hypersomatotropism, all cats in this study showed physical characteristics of acromegaly, and so that term will be used in the remainder of this manuscript.
Materials and methods
Ethical approval was granted for this retrospective study by the University’s Social Sciences Research Ethical Review Board (URN 2017-SR1001-1). Thirty-eight client-owned cats that had undergone hypophysectomy for the treatment of acromegaly between 2012 and 2016 at a European veterinary referral hospital were identified from hospital records. The hospital files of each of these animals, which included treatment records, clinical examination and laboratory results, anaesthetic records, diagnostic imaging and surgery reports, were reviewed. One animal was excluded as the anaesthetic record was missing.
Data extracted from the remaining 37 files included breed, weight, age, sex, fructosamine concentration, glucose concentration at anaesthetic induction, plasma pH, evidence of heart disease based on echocardiography, pituitary adenoma size, drugs used for premedication, induction and maintenance of anaesthesia, total anaesthetic duration, total surgical duration, heart rate, blood pressure, body temperature, peripheral capillary oxygen saturation (SpO2), end-tidal carbon dioxide tension (ETCO2), use of controlled vs spontaneous ventilation under anaesthesia, administration of non-anaesthetic drugs during the surgery, total fluid volume administered, subjective assessment of recovery from anaesthesia (‘unremarkable’ vs ‘abnormal’) by the anaesthetist in charge of the case, postoperative analgesia requirement, duration of intensive care unit (ICU) stay and 24 h mortality.
Limits were set for the physiological variables measured during the anaesthetic period, and if these limits were exceeded for two successive readings on the anaesthetic record (ie, >5 mins duration) then that would be considered an anaesthetic complication. These limits were heart rate <90 beats per minute (bpm; bradycardia) or >180 bpm (tachycardia); Doppler-measured non-invasive blood pressure <70 mmHg (hypotension) or >140 mmHg (hypertension); body temperature >39.5°C (hyperthermia), between 38.4ºC and 36.5°C (mild hypothermia), between 36.4ºC and 34.0°C (moderate hypothermia) or <34.0°C (severe hypothermia); 8 SpO2 <96% (hypoxaemia); ETCO2 <35 mmHg (hypocapnia) or >45 mmHg (hypercapnia); and, finally, any note made on the anaesthetic record of an unexpected adverse event.
Anaesthetic complications identified using the above criteria were bradycardia, hypothermia, hypotension and airway complication (identified from a note on the anaesthetic record indicating that the endotracheal tube lumen was suctioned or the cat was re-intubated).
Data were extracted from patient files to a spread sheet (Microsoft Excel 2013 for Windows). Data analysis was undertaken with IBM SPSS 21. Numerical data were evaluated for normality of distribution using the Shapiro–Wilk test. Where data followed a normal distribution, they are reported as mean ± SD. Where data are not normally distributed, values are reported as median (range). Categorical data are described as n (%).
Risk-factor analysis evaluated associations between patient demographic or drug choice and the odds of each anaesthetic complication occurring.
Univariate binary logistic regression analysis was conducted first for each outcome analysed (complications: bradycardia, hypotension, hypothermia, airway complication, duration of ICU stay and 24 h mortality) and factors with a significance level of P ⩽0.2 were added into multivariable logistic regression modelling for further assessment, with statistical significance set at a P value of <0.05. Model building used backwards elimination and the best-fit model was assessed using the likelihood ratio test.
In addition, Cox regression analysis evaluated the risk factors associated with a longer ICU stay. For this, cats dying in the ICU were considered censored (0) and discharge from the ICU was considered event (1).
Results
Descriptive statistics
Demographics
Results of descriptive statistics are summarised in Table 1.
Perioperative parameters and descriptive statistics in 37 cats undergoing hypophysectomy

ICU = intensive care unit; RI = reference interval; ECHO = echocardiography
Anaesthetic management
The most commonly used premedication was methadone alone (0.2 mg/kg) (62% of cases [n = 23]). Alternative premedication included methadone (0.2 mg/kg) combined with an α2 agonist (either medetomidine [5–10 μg/kg] or dexmedetomidine [2.5–5 μg/kg]; 25% of cases [n = 9]), methadone (0.2 mg/kg) combined with alfaxalone (2 mg/kg [5%, n = 2]), methadone (0.2 mg/kg) together with alfaxalone (1–2 mg/kg) and midazolam (0.25 mg/kg [5%, n = 2]) and methadone (0.2 mg/kg) combined with acepromazine (0.01 mg/kg [3%, n = 1]).
Propofol, dosed to effect was used to induce anaesthesia in 73% of cases (n = 27). Alternatively, alfaxalone was dosed to effect in 14% (n = 5) and co-induction combinations of propofol to effect and midazolam (0.25 mg/kg) was used in 8% (n = 3) or alfaxalone to effect and midazolam (0.25 mg/kg) in 5% (n = 2) of cases.
Anaesthesia was maintained with sevoflurane in 86% of cases (n = 32) and isoflurane in the remaining 14% (n = 5). The volatile anaesthetic agent was titrated to maintain a surgical plane of anaesthesia alongside an opioid infusion in all cases. The opioid used was remifentanil (0.2–0.4 μg/kg/min) in 54% of cases (n = 20) and fentanyl (0.2–0.5 μg/kg/min) in the remaining 46% (n = 17). Controlled mandatory ventilation was used in all cats and this effectively maintained the ETCO2 between 35 mmHg and 45 mmHg throughout anaesthesia. As part of the medical protocol for these cases, all cats received an infusion of soluble insulin. The rate of insulin infusion was adjusted to limit hyperglycaemia. Immediately prior to surgically manipulating the pituitary, a hydrocortisone infusion (0.5 mg/kg/h) was started and continued until the cat could receive oral corticosteroids. Additionally, at this time, desmopressin was administered in the conjunctiva to account for change in antidiuretic hormone production. Total intravenous volume administered was limited to 4 ml/kg/h by adjusting concentrations of administered drugs.
Postoperative analgesia was provided with buprenorphine (0.01–0.02 mg/kg) in all but one cat (97%). The remaining cat received methadone (0.1 mg/kg) for postoperative analgesia. Recovery from anaesthesia was deemed to be unremarkable in 30 of the cats (81%) and the remaining seven (19%) were described to have an abnormal recovery. All cats recovered in the ICU ward. Mean stay in the ICU before being transferred to a lower-dependency ward was 6.8 ± 3.8 days. No cats died during surgery, but three cats (8%) died within 24 h of anaesthetic recovery.
Complications during anaesthesia
From the data collection, four intraoperative complications were identified. The most common complication was hypothermia. All but one cat (97%; n = 36) developed some degree of hypothermia at some point during the procedure. The degree of hypothermia was mild in 8% of cats (n = 3), moderate in 70% (n = 26) and severe in 19% (n = 7). Bradycardia was the second most common complication, with 73% of cats (n = 27) having an abnormally low heart rate at some point during the anaesthetic. The lowest recorded heart rate was 75 bpm. Hypotension was seen in 59% of cases (n = 22). The lowest recorded blood pressure was 50 mmHg. Airway obstruction necessitating suctioning or removal of the endotracheal tube occurred in 32% of cases (n = 12).
Risk factors for intraoperative complications
Multivariate logistic regression showed that cats that did not receive an α2 agonist were more likely to suffer hypotension during the anaesthetic period (odds ratio [OR] 10, 95% CI 1.667–59.999 [P = 0.012]).
Additionally, cats that received a constant rate infusion of remifentanil were less likely to suffer airway complications than cats that received fentanyl infusion (OR 0.14, 95% CI 0.02–0.66 [P = 0.013]). There were no other significant associations between the factors analysed and the remaining complications.
Risk factors for prolonged ICU stay
After univariate analysis, multivariate Cox regression showed that cats with recovery described as ‘abnormal’ were discharged quicker from the ICU compared with cats with a recovery quality described as ‘unremarkable’ (OR 3.6, 95% CI 1.28–10.61 [P = 0.015]) (Figure 1).
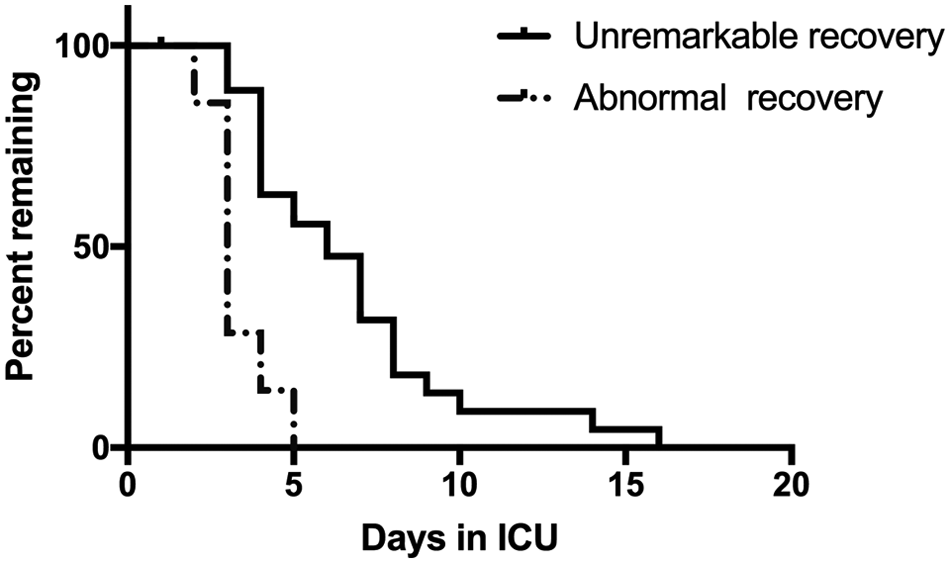
Percentage of cats remaining in the intensive care unit (ICU) over time
Discussion
This study is, to our knowledge, the first to describe the anaesthetic management of cats undergoing hypophysectomy and the first to assess whether the drugs used affect patient stability during the procedure or have any effect on short-term outcome.
The anaesthetic protocols used in this study seem to be well tolerated. Perioperative mortality was lower than previously reported; however, intraoperative complications were common.
Perianaesthetic mortality was found to be 8%. ‘Anaesthetic death’ is a controversial term and the time frame in which death can be attributed to anaesthesia is unclear. 9 Reports across the human literature define anaesthesia-related mortality with marked variation from 24 h to 30 days post-emergence from anaesthesia. 10 A 24 h follow-up period was chosen in this study as it allows comparison with a similar study in cats. 11 The mortality rate reported here is slightly lower than previously reported. 11 In that study, there was one death within 24 h from a total of seven cats undergoing hypophysectomy (14%). It is worth noting that those seven cats underwent surgery for treatment of hyperadrenocorticism rather than acromegaly and the populations between the studies are likely to have had different comorbidities or clinical status prior to surgery.
Intraoperative complications identified during the cases reviewed here included hypothermia, bradycardia, hypotension and airway obstruction.
Hypothermia is a commonly encountered complication in feline anaesthesia. 8 It was the most common complication found in our study, with an overall prevalence of 97%. Redondo et al found that anaesthetic duration was a risk factor for the development of hypothermia. 8 A mean anaesthetic time of 354 mins may explain the high incidence of hypothermia in this study.
The second most common complication identified was bradycardia. Bradycardia was present in 73% of cases, and may have been attributed to factors including hypothermia, 12 or drug effects of the opioids and α2 agonists. However, no significant relationship was found between these factors and it is proposed the small sample size may have prevented detecting any significant effect of these factors on the development of bradycardia.
Hypotension was also frequently identified in this study and is a previously reported complication of anaesthesia in cats. 13 Blood pressure was measured by Doppler ultrasound and it must be considered that this technique may be inaccurate in cats. 14 In our case, the most likely causes of hypotension were vasodilation caused by anaesthetic drugs; potential subclinical dehydration in polyuric diabetic cats; and bradycardia causing a reduction in cardiac output. The cut-off value of 70 mmHg was chosen as it has been suggested that Doppler blood pressure measurement in cats represents a value closer to the mean blood pressure rather than systolic, 14 and values below this may lie outside of vital organ autoregulation thresholds. However, this value is not universally accepted and other cut-offs have been used for definition of hypotension in cats in the veterinary literature.15,16
The final complication identified was airway obstruction. This occurred in 32% of cases. Unfortunately, the change alerting the anaesthetist to the presence of obstruction was not always recorded. When this information was recorded on the anaesthetic form reasons included changes in the capnography waveform, reverberating noise from the breathing system and pressure alarms on the ventilator. The timing of obstruction was also variable, occurring during clipping and scrubbing, as well as during the surgical procedure, and no pattern could be appreciated. To our knowledge there are no published data on the incidence of airway obstruction in cats, but from clinical experience, the rate reported here is much higher than in general feline anaesthesia. Although it may be expected that airway complications may be seen more frequently during a surgery such as this where the soft palate and nasopharynx are involved, additional factors which may have led to the higher-than-normal frequency were hypothesised. These included long anaesthesia time and breathing dry anaesthetic gases, which have been shown to increase tenacity of respiratory secretions and risk obstruction of the endotracheal tube; 17 and laryngeal hyperplasia caused by increased circulating growth factor, which hinders endotracheal intubation and necessitates the use of a smaller internal diameter endotracheal tube than would normally be used for the patient size.
Our study found that cats anaesthetised with a protocol including remifentanil were less likely to suffer airway obstruction as a complication than those receiving fentanyl infusion. This result was surprising and the mechanism behind the result is not immediately obvious. One study found a greater reduction in bronchial mucus transport velocity in human patients receiving remifentanil infusion compared with those receiving morphine, but a mechanism was not established. 18 Furthermore, no study was identified that compared fentanyl and remifentanil directly. Wang et al also found an opioid-induced increase in airway fluid production while reducing mucus transport, but this effect was not specific to fentanyl. 19
As part of the treatment plan at the clinic studied, all cats underwent preoperative echocardiography and 17 cats (46%) had hypertrophic cardiomyopathy. This is slightly lower than the proportion found in an earlier study describing echocardiographic findings in acromegalic cats, where 64% of cats were affected. 20 High circulating levels of insulin-like growth factor-1 are known to cause hypertrophy of the myocardium. 21
This study did not find any relationship between the size of the pituitary tumour and intraoperative complications or short-term survival. This is discordant with a study involving dogs undergoing pituitary mass resection for treatment of hyperadrenocorticism, where tumour size was negatively correlated with outcome. 22 That study analysed data from 306 animals. It is possible that our study population was too small for such a pattern to be appreciated. Additionally, that study also used a ratio of pituitary height to brain area, rather than the absolute pituitary dimension used here.
The use of medetomidine or dexmedetomidine was shown to decrease the incidence of hypotension, perhaps as a result of their vasoconstrictive action, or dose-sparing effects allowing use of less vasodilatory inhalational anaesthetic agent. Additionally, α2 agonists provide good chemical restraint for aggressive cats, and their use has not been shown to be deleterious in cats with hypertrophic cardiomyopathy. 23 The α2 agonists have also been shown to have neuroprotective action against neuronal ischaemia in in vitro laboratory animal studies. 24
Opioid infusion was administered to all cats for analgesia and to reduce volatile anaesthetic dose requirements. 25 Both fentanyl and remifentanil have pharmacokinetic profiles that make them suitable for infusion for short periods. However, in humans, the context-sensitive half-time for fentanyl increases after a few hours infusion, prolonging recovery. 26 One study in cats showed no prolonged elimination following infusion of fentanyl for 2 h in conscious cats, 27 but there are no data, to our knowledge, on the pharmacokinetics of fentanyl beyond this timescale in felines. In light of the relatively long surgical time and effect on airway obstruction found in this study, remifentanil may be the better option for this procedure as its elimination is rapid and unaffected by infusion duration. 28
A recovery quality described as ‘unremarkable’ was associated with a longer stay in the ICU. This is a surprising result, and may be spurious owing to the very subjective and often limited description of the recovery on the anaesthesia record. For example, it was rarely expanded upon as to whether the recovery was ‘abnormal’ in terms of duration, altered mentation or presence of emergence delirium, dysphoria, etc. It is also possible that systemically healthier patients may have recovered faster and more roughly, leading their recovery to be more likely described as ‘abnormal’.
Limitations of this study include its retrospective nature and the small sample size. However, this is the first study to describe the management and complications encountered during the anaesthetic period in cats undergoing hypophysectomy. These preliminary data may still be a useful reference to anaesthetists responsible for these cases.
Conclusions
Anaesthesia for hypophysectomy in cats with acromegaly can be performed using the protocols described in this study. The mortality rate was slightly lower than in the limited existing literature. Common complications during the anaesthetics included hypothermia, hypotension, bradycardia and airway obstruction.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.