
Abstract
Objectives
The aim of this retrospective study was to describe the location and distribution of craniomaxillofacial (CMF) fractures in 45 cats presented to a veterinary referral centre between 2012 and 2017.
Methods
Cats with a history of head trauma, one or more CMF fractures and a pretreatment CT scan of the CMF region were included in this study. For the purpose of the study, the CMF skeleton was divided into 15 functional anatomical regions and the fracture sites were allocated to one of these functional regions. Statistical analysis was performed using R.
Results
Skull fractures were evident in 80.0% of cats, and mandibular fractures in 86.7% of cats in this study. The median number of anatomical functional regions affected was eight and there was evidence of moderate or strong correlation between fractures of different regions of the mid-face. Where fractures were recorded in the nasopharynx and orbit they were bilateral in 93.5% and 89.7%, respectively. Twenty-six (57.8%) of the cats had fractures affecting one or both temporomandibular joints, which included fractures of the mandibular fossa, condylar neck and condyle. Twenty-nine cats (64.4%) had tooth fractures and seven cats (15.6%) had significant eye injuries.
Conclusions and relevance
Cats presenting with a single symphyseal separation or parasymphyseal fracture are very likely to have further fractures at other locations. Fractures in the nasopharynx, orbit, nose, upper jaw, intermaxillary suture and zygomatic arch regions (the ‘mid-face’) are likely to occur together. The pattern of distribution of mandibular fractures is not as predictable as that for maxillary fractures. CT imaging is required to achieve a complete diagnosis of the location and distribution of skull fractures in cats after head trauma.
Introduction
The maxillofacial skeleton in cats is commonly fractured owing to its prominent position and its susceptibility to sustaining serious trauma.1,2 Injury can result from a road traffic accident (RTA), a fight or a fall from a height (high-rise syndrome). 1
Physical examination is generally insufficient to accurately classify maxillofacial injuries, owing to soft tissue swelling and the inaccessibility of the deep mid-face region. Clinical findings can include epistaxis, abrasions, eye trauma, jaw fracture, symphyseal separation, tooth fracture and temporomandibular joint (TMJ) luxation. 3
In the veterinary literature, CT imaging has been shown to be superior to plain radiography for the identification of craniomaxillofacial (CMF) anatomical structures and CMF fractures. 4 The last published study to look at the distribution of mandibular fractures in cats, by Umphlet and Johnson in 1988, 5 relied on conventional radiographs and not CT.
An appreciation of the incidence and distribution of facial fractures in traumatised cats could help to develop an understanding of the most appropriate diagnostic and treatment options for these patients. This retrospective study describes the location and distribution of skull fractures in 45 cats presented to an oral surgery department of a veterinary referral centre between 2012 and 2017, and looks for evidence of common fracture patterns, correlation of the occurrence of fractures between functional regions and associated ophthalmic and dental injuries.
Materials and methods
The medical records of cats treated for head trauma by the Dentistry and Oral Surgery Department at Eastcott Referrals, Swindon, UK, between 2012 and 2017 were reviewed. Cats that had a record of head trauma, one or more skull fractures and a pretreatment CT scan of the entire skull were included in this study. Signalment, presence of CMF fractures, cause of trauma and presence of concomitant ophthalmic and dental injuries were recorded.
CT scans were performed obtaining transverse, 0.625 mm collimated images using a Lightspeed 4 CT scanner (GE Healthcare) with a kVp of 120 and auto-mA. All CT scans were obtained with patients under general anaesthetic. Cats were premedicated with methadone (0.2 mg/kg IV) and medetomidine (2.5 μg/kg IV). Anaesthesia was induced with propofol (5 mg/kg IV), cats were intubated and maintained on isolflurane in oxygen.
CT images were assessed by a specialist and two residents in dentistry and oral surgery. Radiographic data were obtained and viewed using the Horos platform, which enables reformatting in coronal, sagittal and axial planes. The skull was divided into 15 functional anatomical regions (Figure 1), and each region containing a fracture was identified and recorded. CT images were initially assessed independently and the presence or absence of fractures recorded in each functional region. No attempt was made to account for the number or type of fractures. The results of the three observers were compared and where differences occurred the CT images were re-examined by all observers together in order to arrive at a consensus.

Colour-coded diagrams showing the functional regions used for recording craniomaxillofacial fractures and with labels to show their relationship with the bones of the skull and mandibles
The boundary of each functional region was defined in order that data analysis would provide useful clinical information. For example, fractures of the rostral part of the body of the mandible were recorded separately from the symphysis/parasymphysis and mid-/caudal mandibular body as fractures in these regions present different clinical and surgical challenges. Fractures that extended between two or more regions were recorded as separate fractures in each region.
Descriptive statistics were used to describe the incidence of fractures of specific functional regions.
Further analysis of the data was performed to look for associations between fractures in each functional area using the following tests. Pearson’s correlation coefficient was calculated for all paired regions and tested for significance against 0. A P value <0.05 shows that correlation is evident above noise in the data, and a correlation coefficient of >0.7 indicates a strong relationship and >0.5 a moderate relationship. The occurrence of bilateral fractures was estimated using a generalised linear mixed effects model with a binomial distribution and logit link function. The response was an indicator of bilateral or unilateral, the fixed effect was the skull region and a random effect of cat was included to account for repeat measures. With this model means were estimated for each skull region, including 95% confidence intervals. The occurrence of maxillary or mandibular fractures, in the presence of a parasymphyseal fracture or symphyseal separation, was modelled with two generalised linear models, again with binomial distributions. The responses in the models were an indicator of extra fractures beyond (para-)symphyseal, in the maxilla or mandible, with an intercept as the fixed effect. The mean probability was estimated from each of these two models with 95% confidence intervals. For all models described above the estimated probabilities were tested for significance differences from 0.5, random chance, where a P value <0.05 indicates a significant difference.
Statistical analysis was performed using R v3.3.3. 6
Results
This retrospective study of 45 cats included 23 neutered males, four entire males, 17 neutered females and one entire female. Mean age was 53 months (range 5–240 months). Thirty-two cats (71.1%) were <60 months old. The breed distribution was as follows: 39 domestic shorthairs, one Burmese, one Persian, one Turkish Van, one Havana, one Bengal and one Persian cross.
Causes of trauma in these patients were RTA (n = 34), fall from a height (n = 1), bite wounds from a dog (n = 1), fight injury with another cat (n = 1), domestic accident (n = 1 [impact from a falling garden gnome]) and unknown cause (n = 7).
The incidence of fractures in each functional region, and the proportion of cases where these fractures were bilateral, is shown in Table 1. Skull fractures were evident in 80.0% and mandibular fractures in 86.7% of cats in this study. Of those with skull fractures, 86.1% had bilateral fractures and of those with mandibular fractures 18.0% were bilateral. TMJ luxation was present in four cats (8.9%).
In the skull, bilateral fractures were particularly common in the mid-face region (nose, upper jaw, intermaxillary suture, orbit, nasopharynx and zygomatic arch)

Where nasopharyngeal and orbital fractures were recorded they were bilateral in 90.3% and 83.9%, respectively (Figure 2)
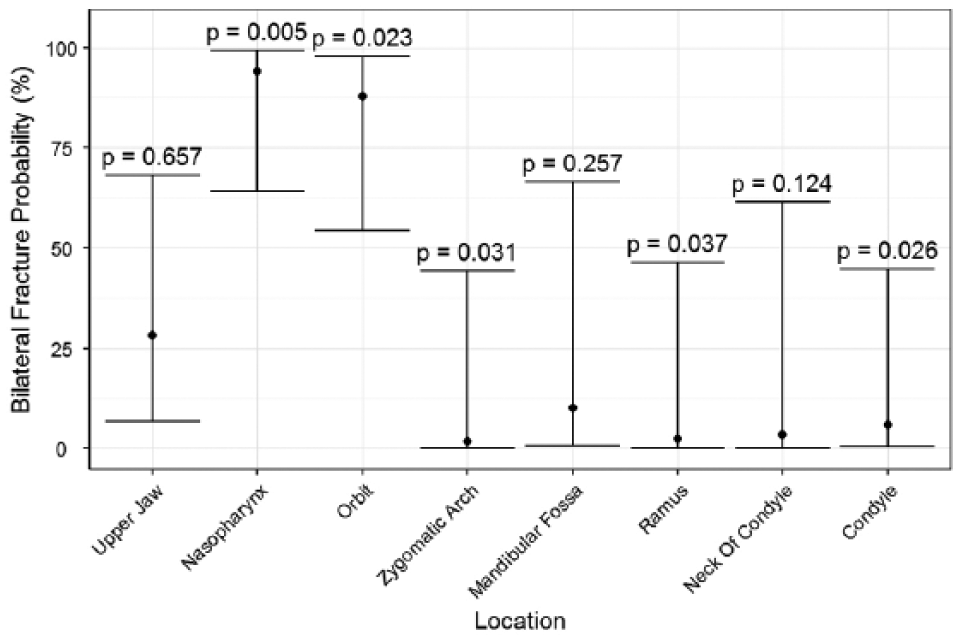
Estimated probabilities of bilateral fractures, in the presence of at least one fracture, with 95% confidence intervals. P values <0.05 indicate that the probability is significantly different from 0.5; ie, random chance
The number of functional regions with a fracture in each cat ranged from 1–13. Only one cat had a single functional region affected. The median number of fractures per cat was eight, with a median of five skull fractures and a median of two mandibular fractures per cat (Figure 3).
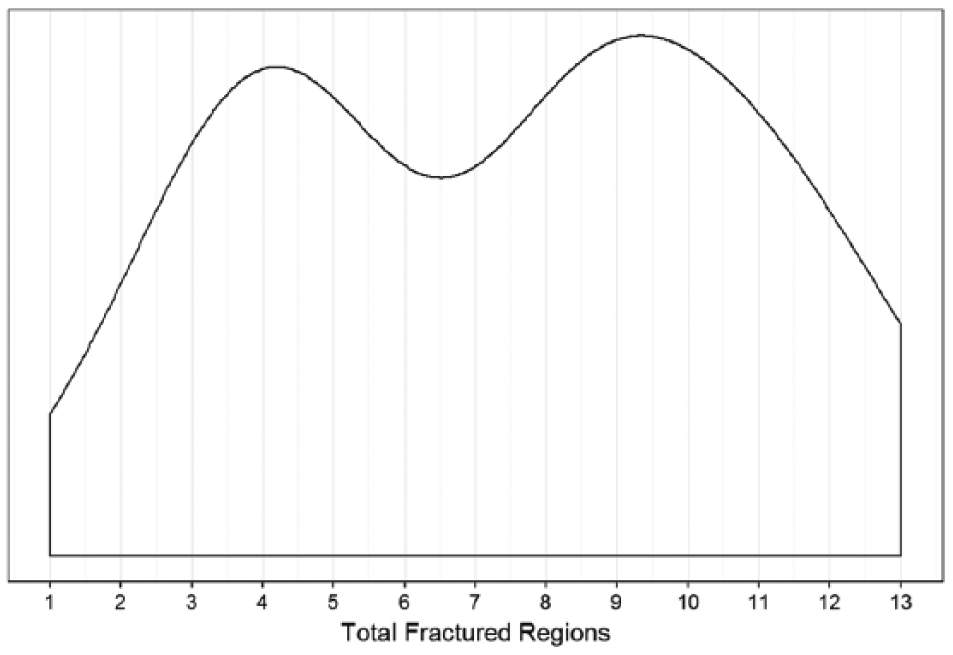
Density plot showing the distribution of the total number of fractured regions per cat. The most likely number of fractures is 9–10, closely followed by 4
Pearson’s correlation coefficient was calculated for all pairs of regions and tested for significance against 0. A P value <0.05 shows that correlation is evident above noise in the data, and a correlation coefficient >0.7 indicates a strong relationship and >0.5 a moderate relationship (Table 2). The heat map demonstrates correlation of fractures between different functional regions (Figure 4). Values >0.5 indicate a moderate to strong correlation and illustrate that the strongest correlation exists in the ‘mid-face’ region of the maxilla.
Twenty-nine of 45 cats had dental injuries (uncomplicated or complicated crown fractures) associated with skull fractures
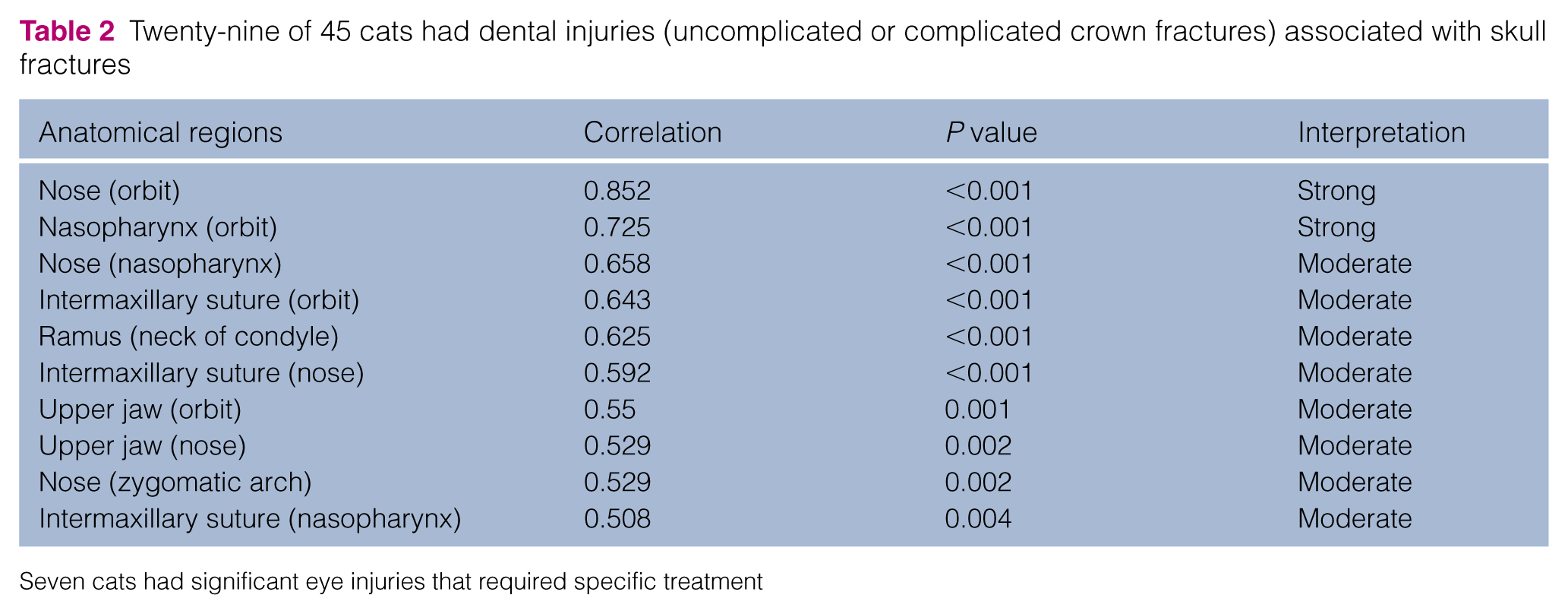
Seven cats had significant eye injuries that required specific treatment
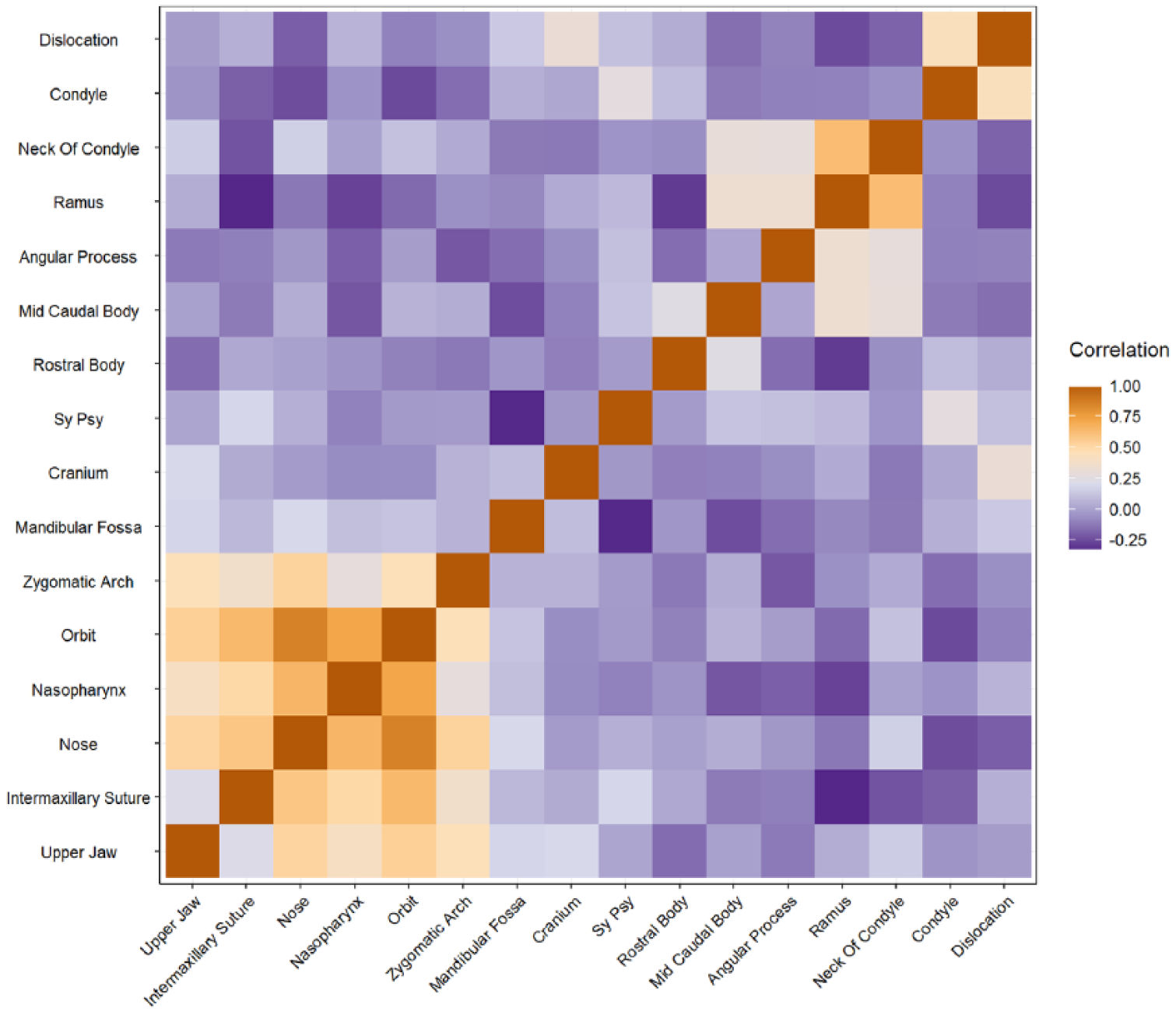
Heat map of estimated correlation between all pairs of skull fracture regions, relating to Table 2. Correlation values >0.7 indicate strong correlation and >0.5 indicates moderate correlation. The lower left corner, from lower jaw to zygomatic arch, is almost entirely >0.5, indicating that fractures in this entire region are correlated
Eight of the 45 cats were treated prior to referral with circum-mandibular wire used to stabilise a symphyseal separation or parasymphyseal fracture. All of the 26 cats in this study that presented with a symphyseal separation or parasymphyseal fracture had additional fractures.
To investigate parasymphyseal fractures and symphyseal separation further, the likelihood of other mandibular and maxillary fractures, in the presence of a parasymphyseal fracture or symphyseal separation, was modelled. The results (Figure 5) show that in the presence of a symphyseal separation or parasymphyseal fracture the probability of another fracture occurring is significantly greater than 50% (random chance). In the case of the mandible there is an 84.6% chance of another fracture (P = 0.0017) and there is a 73.1% chance of a fracture in the skull (P = 0.0239).

Estimated probabilities of mandibular and maxillary fractures, in the presence of parasymphyseal fractures or symphyseal separation, with 95% confidence intervals. P values <0.05 indicate that the probability is significantly different from 0.5; ie, random chance
Discussion
The results of the previous study by Umphlet and Johnson of mandibular fractures showed 49/62 cats (79.0%) had a single mandibular fracture and 13/62 cats (21.0%) had multiple fractures. 5 Symphyseal ‘fractures’ were most common (73.3%), followed by fracture of the body of the mandible (16%), condyle (6.7%) and coronoid process (4%). In our study, 39/45 cats had at least one mandibular fracture. Of the 39 cats with mandibular fractures, 29 (74.4%) had two or more mandibular fractures and only 12 cats (30.8%) had a single mandibular fracture.
If the mandibular fractures identified in our population of cats had been allocated to regions using the system described by Umphlet and Johnson, 5 there were 25 (64.1%) symphyseal ‘fractures’, 15 (38.5%) fractures of the mandibular body, 22 (56.4%) condylar fractures and 17 (43.6%) ramus fractures. Our data show both a much higher incidence of multiple mandibular fractures and a different fracture distribution with caudal fractures being more common. The greater incidence of multiple mandibular fractures in our study may be accounted for by the superiority of CT over radiography for the diagnosis of CMF fractures. 4 CT allows better radiological examination of the complex anatomy of the CMF region without the superimposition of bone structures.
The method used in this study of recording fractures in predetermined anatomical regions means that parts of individual skull bones may be represented in more than one functional region; for example, the frontal bone is represented both as part of the brain case and orbit. It is clear that the clinical implications of skull fractures are different in these two regions and therefore recording a fracture as simply a fracture of the frontal bone provides information of limited clinical significance.
The average number of anatomical regions containing at least one fracture was 7.24 and as our data were qualitative rather than quantitative it is likely that the average number of fractures per cat was higher than this. The highest incidence of fractures occurred in the nasopharynx (68.9%) and orbit (68.9%), with symphyseal separation and parasymphyseal fractures occurring in 55.6% of cases
We saw eight cats that had treatment of single jaw fractures (usually symphyseal or parasymphyseal) prior to referral. The mandibular symphysis is the fibrocartilage and connective tissue structure that joins the left and right mandibles rostrally. Injuries causing tearing and disruption of this structure are called symphyseal separation and fractures of the mandibular bone adjacent to the symphysis are called parasymphyseal fractures. Subsequent CT scanning revealed previously undiagnosed fractures of the skull or mandible, which had rendered the original fixation inadequate. Our data show that cats rarely present with single jaw fractures and that conventional radiography may not be sufficiently sensitive to diagnose many of the less obvious fractures.
With the exception of the symphyseal separation and parasymphyseal fractures, fractures to the ‘mid-face’ region were most common. This includes the nasopharynx (68.9%), orbit (68.9%), nose (51.1%), upper jaw (51.1%), intermaxillary suture (44.4%) and zygomatic arch (33.3%). Statistical analysis demonstrated that fractures in these mid-face regions are likely to occur together (Figure 4). Fractures to the bones surrounding the brain (‘brain case’) were relatively rare (4.4%). It has been postulated that in humans the bones of the mid-facial skeleton act as a ‘crumple zone’, thereby reducing the transmission of force to the intracranial contents. This has been supported by the work of Lee et al, 7 who demonstrated that the paranasal sinuses and nasal cavity provide a ‘crumple zone’, reducing the transmission of energy and fracture to the posterior cranial fossa. The distribution and incidence of fractures in our study suggest that the mid-face region may act as an energy-absorbing region in cats, thus reducing the impact on the brain and protecting the bones immediately surrounding the brain from fracture.
Although the incidence of fractures in the nasopharynx and nose was high, the clinical significance of these fractures is not immediately obvious and repair or stabilisation is not required or feasible in most cases. Further analysis of clinical data is required in order to evaluate whether there is a correlation between the presence of nasopharyngeal and nasal fractures and post-traumatic morbidity.
Seven cats in our study had clinically significant eye injuries that varied from intraocular haemorrhage to rupture of the globe. Three of these cats did not have orbital fractures. Twenty-five of 29 cats with orbital fractures did not have clinically significant eye injuries. These results suggest that all cats with head trauma should have a detailed ocular examination and sight evaluation. Some of the bones of the orbit (especially on the nasal side) are thin and fragile. The incidence of fractures is high and the fractures are often multiple and complex. It is possible that the energy absorbed by the orbital bones prevents more significant eye injury.
The pattern of mandibular fractures is not as predictable as for maxillary fractures and apart from the neck of the condyle and the ramus there is a low correlation between fractures in different regions. Fractures of the rostral mandibular body and angular process are rarely bilateral (4.3% and 2.2%, respectively) and bilateral fractures are more common in the caudal mandible.
TMJ ankylosis is a potential sequel to TMJ fracture. 8 Twenty-seven (60.0%) cats in our study had fractures affecting one or both TMJs (mandibular fossa, condylar neck, condyle). It is therefore important to diagnose these fractures accurately to provide appropriate treatment and allow a realistic prognosis to be provided to the client and recommend CT assessment owing to its superior ability to diagnose these fractures over conventional radiography.
The incidence of tooth fracture in our study was 64.4%, which is similar to previously published findings. 9 Because of the clinical significance of the accompanying skull fractures, treatment of these injuries may not be an immediate clinical priority. However, where possible, a thorough dental and oral examination, recorded on a dental chart, should be part of the initial assessment of all feline patients with head injuries. Appropriate treatment, if not performed during the first anaesthetic, should be planned for a later date.
Limitations to this study include that it involved a relatively small number of cats from a referral population, which may represent more severely injured individuals and that cats with brain case injuries are more likely to have died prior to presentation and therefore will not be accurately represented in our data. Equally, the number and distribution of fractures in this study reflect the fact that most trauma was associated with RTA. It is possible that the number and distribution would be different for other causes such as ‘high-rise syndrome’. 2 A dental chart recording details of a full dental examination was present in 43/45 cats in the study.
Conclusions
The findings of this study indicate that there is a common and predictable pattern of distribution of fractures affecting the skull in cats following head trauma. There is a high incidence of mid-face and TMJ fractures. Mid-face fractures tend to be bilateral.
The pattern of mandibular fracture is less predictable, although single CMF fractures are uncommon. Cats presenting with symphyseal separation or parasymphyseal fractures commonly have other mandibular and skull fractures when imaged with CT rather than plain radiographs.
Along with thorough evaluation of skull and mandibular fractures and a thorough neurological assessment, ophthalmological and dental examination is necessary.
Further clinical data analysis is required to evaluate the significance of the distribution of skull fractures in making clinical decisions regarding appropriate fracture fixation techniques and the recovery of patients following injury and subsequent treatment.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.