
Abstract
Objectives:
The main aim of the study was to describe the features and diagnoses of a population of cats referred with pyrexia. Other aims were to report and evaluate the utility of clinical investigations performed, and describe any effect of treatment before referral on temperature at presentation and ability to make a diagnosis.
Methods:
Clinical records of cats with pyrexia (⩾39.2°C) documented at least twice were retrospectively reviewed. Cases were assigned to disease categories (infectious, inflammatory, immune-mediated, neoplastic, miscellaneous and no diagnosis [pyrexia of unknown origin, PUO]) based on diagnosis. The overall value of clinical investigations was assessed by classifying them as ‘enabling’, ‘assisting’ or ‘no assistance’ in achieving each diagnosis. The effect of treatment before referral was assessed for any association with temperature at presentation and ability to make a diagnosis (PUO vs other disease categories).
Results:
One hundred and six cases were identified. The most common cause of pyrexia was feline infectious peritonitis (22 cats, 20.8%) and the largest disease category was infectious (41/106, 38.7%). Inflammatory conditions were found in 19 (17.9%) cats, neoplasia in 13 (12.3%), miscellaneous causes in 11 (10.4%) and immune-mediated disease in six (5.7%). No diagnosis was reached in 16 (15.0%) cats, often despite extensive diagnostic investigations. Cytology and histopathology most often ‘enabled’ or ‘assisted’ in obtaining a diagnosis. Most cats (91, 85.8%) received treatment before referral, with antimicrobial treatment given to 87 (82.1%). Prior treatment before referral was not associated with temperature at presentation nor with success in establishing a diagnosis.
Conclusions and relevance:
This is the first study investigating causes of pyrexia in cats. Infectious diseases were most common and immune-mediated diseases were comparatively rare.
Introduction
Pyrexia (fever) is an increased body temperature secondary to the release of pyrogens and a raised thermoregulatory set point in the anterior hypothalamus. 1 It is part of the nonspecific adaptive response of the body to disease and is thought to confer a significant evolutionary advantage. However, there are disadvantages of pyrexia and these tend to outweigh the benefits when pyrexia becomes more severe or prolonged. 1
Pyrexia that remains undiagnosed despite investigations is referred to as pyrexia of unknown origin (PUO). Over 200 diseases have been associated with PUO in humans. 2 Precise definitions of PUO vary. Extrapolating from human medicine, PUO in dogs and cats has been defined as a temperature ⩾39.2°C (102.6°F) of at least 3 weeks’ duration in which no obvious cause is found following at least three visits to the veterinary surgeon and/or 3 days of hospitalisation (including basic evaluation of history, clinical signs, physical examination and diagnostic testing [complete blood count, serum biochemistry, urinalysis]). 1 Recommendations regarding the diagnostic approach to pyrexia have been described in cats,1,3,4 but as no studies investigating the causes of pyrexia have been published in cats, such recommendations are experience-based rather than evidence-based. It has been stated that infectious diseases are the most common causes of feline pyrexia3,5 but no published evidence exists. Immune-mediated disease is known to be the most common cause of pyrexia in dogs.6–8
The aims of the present study were to describe the population characteristics of cats with pyrexia referred to two veterinary referral centres and to identify the causes of pyrexia. Further objectives were to report the clinical investigations performed and evaluate their usefulness in obtaining a diagnosis, and to describe treatments given before referral and their possible effect on temperature at presentation and ability to reach a diagnosis.
Methods
The clinical databases of feline patients referred to the Small Animal Hospital, University of Bristol, UK, and the Small Animal Hospital, University of Glasgow, UK, from January 2011 to June 2015 were retrospectively searched to identify cats with pyrexia. Databases and clinician case logs were searched using the terms ‘pyrexia’, ‘pyrexic’, ‘PUO’ and ‘fever’. Case records were then retrospectively reviewed (SS) and appropriate details entered into a spreadsheet (Excel for Windows, Microsoft). Details regarding signalment, history, physical examination and minimum database were obtained for all cats. Peak temperature documented by the referring veterinarian within the previous month and temperature at presentation to the referral centre were recorded (Figure 1). Further diagnostic investigations were performed depending on clinical presentation and the attending clinician’s discretion. To be included, pyrexia (rectal temperature ⩾39.2°C [102.6°F]) had to have been documented at least twice (to help rule out cats with stress hyperthermia), including at least once at the referring veterinary practice. Cases were excluded if records were inadequate.

While the cats in this study had their temperature measured rectally, recent work has shown a close correlation between rectal and axillary temperature in cats 9
The study was approved by the University of Bristol’s Animal Welfare and Ethical Review Body (veterinary investigation number [VIN] 16/019) and the University of Glasgow’s Research Ethics Committee (37a/16).
Treatment before referral
Any drug administered by the referring practice after the initial documentation of pyrexia was recorded. As this included a large range of drugs, individual agents were grouped into therapeutic classes: non-steroidal anti-inflammatory drugs (NSAIDs), antimicrobials, corticosteroids, opioid analgesics, ‘supportive’ gastrointestinal medications (eg, antiemetics, antacids) and miscellaneous drugs.
Diagnostic investigations
Investigations performed by the referring veterinarian and at the referral centre were recorded. For the purpose of analysis, neutrophilia was graded as mild (12 to <20 × 109/l), moderate (20 to <30 × 109/l) or severe (⩾30 ×109/l); neutropenia was defined as <4 × 109/l. Anaemia was classified as mild (packed cell volume 20 to ⩽24%), moderate (15 to <20%) or severe (<15%). Increases in alanine aminotransferase (ALT) were graded as mild (<2 times upper reference interval [RI]), moderate (⩾2 to 3 times upper RI) or severe (>3 times upper RI). Hypoalbuminaemia was classified as mild (20 to <24 g/l), moderate (16 to <20 g/l) or severe (<16 g/l).
Imaging techniques included ultrasonography, radiography, CT, MRI and endoscopy. Cytological examination was performed on fine-needle aspirates from any abnormal masses or enlarged lymph nodes. Feline immunodeficiency virus (FIV) antibody and feline leukaemia virus (FeLV) antigen testing was initially performed using PetChek ELISA (IDEXX) or FeLV/FIV SNAP (IDEXX), with PCR testing and/or virus isolation performed if results were positive.
Each diagnostic investigation was retrospectively categorised as ‘enabled’ a diagnosis, ‘assisted’ a diagnosis, or of ‘no assistance’. 7 In cases where a negative result contributed to a diagnosis, the test was reported as ‘assisted’ a diagnosis. A complete blood count and serum biochemistry were performed in all cats; their usefulness in obtaining a diagnosis was not examined.
Cause of pyrexia: disease groups
Cats were retrospectively assigned to one of the following disease groups based on final diagnosis: infectious, inflammatory, immune-mediated, neoplasia, miscellaneous and no diagnosis reached (PUO). Where more than one disease process from different categories was diagnosed, the disease attributed to be the cause of the pyrexia was classified. When this was unclear, cases were defined as miscellaneous.
Outcome
Whether cats survived to discharge, were euthanased or died was recorded.
Statistical analysis
Statistical analysis was performed using SPSS for Windows v23 (IBM Corp). Descriptive statistics were prepared for all evaluated variables. Kolmogorov–Smirnov tests were used to test for normality; continuous variables were reported as means and standard deviations if normally distributed, and as medians and ranges if not normally distributed.
Overall treatment before referral (yes/no) was assessed for association with temperature at presentation using a t-test. Treatment was assessed for association with success in making a diagnosis (ie, PUO [no diagnosis] vs all other disease categories [diagnosis reached]) using a X2 test. Significance was defined as P <0.05.
Results
One hundred and six cats met the inclusion criteria.
Signalment
Of the 106 cats, the most common breed was domestic (69 [65.1%]; 64 [60.4%] domestic shorthair, five [4.7%] domestic longhair); the remaining 37 (34.9%) cats were pedigrees. These comprised seven (6.6%) Ragdolls, six (5.7%) Bengals, six (5.7%) British Shorthairs, five (4.7%) Birmans, four (3.8%) Maine Coons, three (2.8%) Siamese, and one each (0.9%) of Balinese, Devon Rex, Korat, Oriental, Persian and Russian Blue. Median age was 4.0 years (10 weeks to 15 years).
History and treatment before referral
Diagnoses were known or suspected at the time of referral in 11 (10.3%) cats; these tended to be infectious (eg, pyothorax, pyelonephritis, cellulitis), lymphoma (two cats) or structural disease (eg, ureteral obstruction, intestinal intussusception). Two of 22 referring veterinarians mentioned feline infectious peritonitis (FIP) as a possible diagnosis at referral.
Ninety-one cats (87.5%) received treatment before referral; treatment data were unavailable for two cases. Treatment had been given within 24 h of referral in 77 (74.0%) cats. Antimicrobials were administered in 85 cats (81.7%) (Table 1); of these, 52 received one antimicrobial, 28 received antimicrobials from two different classes, and five received antimicrobials from three or more different classes. Almost two-thirds of cats received NSAIDs (67/104, 64.4%) and approximately one-quarter received corticosteroids (25/104, 24.0%). Opioid analgesia was administered to 30 cats (28.8%), 26 cats (25.0%) received gastrointestinal support medication, and 20 cats (19.2%) received other, miscellaneous drugs.
Antimicrobials administered before referral in a population of 106 cats with pyrexia

AC = amoxicillin-clavulanic acid; TMPS = trimethoprim sulfonamide
Mean (± SD) peak temperature documented before referral was 40.1°C (± 0.5°C). Pyrexia was reported to be present for a median of 4 days (1–168 days) before presentation. Eighty-one cats (76.4%) were pyrexic at referral and mean temperature at presentation was 39.7°C (± 0.6°C). Overall, treatment before referral was not associated with temperature at presentation (P = 0.543), nor with success in reaching a diagnosis (P = 0.999). As pyrexia associated with FIP is expected to be refractory to treatment, the association of treatment before referral was also assessed in non-FIP cats only, and no significant association was found (unpublished data).
Diagnostic investigations
The number of cats in which diagnostic investigations were performed and the usefulness of investigations in obtaining a diagnosis are shown in Table 2. Complete blood count and serum biochemistry were performed in all cats (results were unavailable in two cases). The most common findings were neutrophil abnormalities and anaemia on complete blood count, and increased ALT and hypoalbuminaemia on serum biochemistry (Table 3).
Utility of diagnostic investigations performed in 106 cats with pyrexia

FeLV = feline leukemia virus; FIV = feline immunodeficiency virus; PLI = pancreatic lipase immunoreactivity; GI = gastrointestinal; FCoV = feline coronavirus; FCV = feline calicivirus; FHV = feline herpesvirus
Most common complete blood count and serum biochemistry abnormalities detected in 104 cats with pyrexia

Neutrophilia: mild (12 to <20 × 109/l), moderate (20 to <30 × 109/l), severe (⩾30 × 109/l). Neutropenia: <4 × 109/l. Anaemia: mild (packed cell volume 20 to ⩽24%), moderate (15 to <20%), severe (<15%). Alanine transaminase (ALT): mild (<2 times upper reference interval [RI]), moderate (⩾2 to 3 times upper RI), severe (>3 times upper RI). Hypoalbuminaemia: mild (20 to <24 g/l), moderate (16 to <20 g/l), severe (<16 g/l)
Disease categories
Final diagnoses and disease categories are listed in Table 4. Infectious disease represented the largest category (41/106, 38.7%). Within this category, FIP was diagnosed in 22 cases (20.8%) (Figure 2). Inflammatory (non-infectious) disease comprised the second-most common disease category (19/106, 17.9%) and neoplastic disease third (13/106, 12.3%). Pyrexia was attributable to miscellaneous conditions in 11 cats (10.4%). Immune-mediated disease was the smallest disease category (6/106, 5.7%). No diagnosis (PUO) was established in 16 cases (15.1%). The median ages of cats in each disease category are described in Table 5.
Final diagnosis and disease category classification for 106 cats with pyrexia
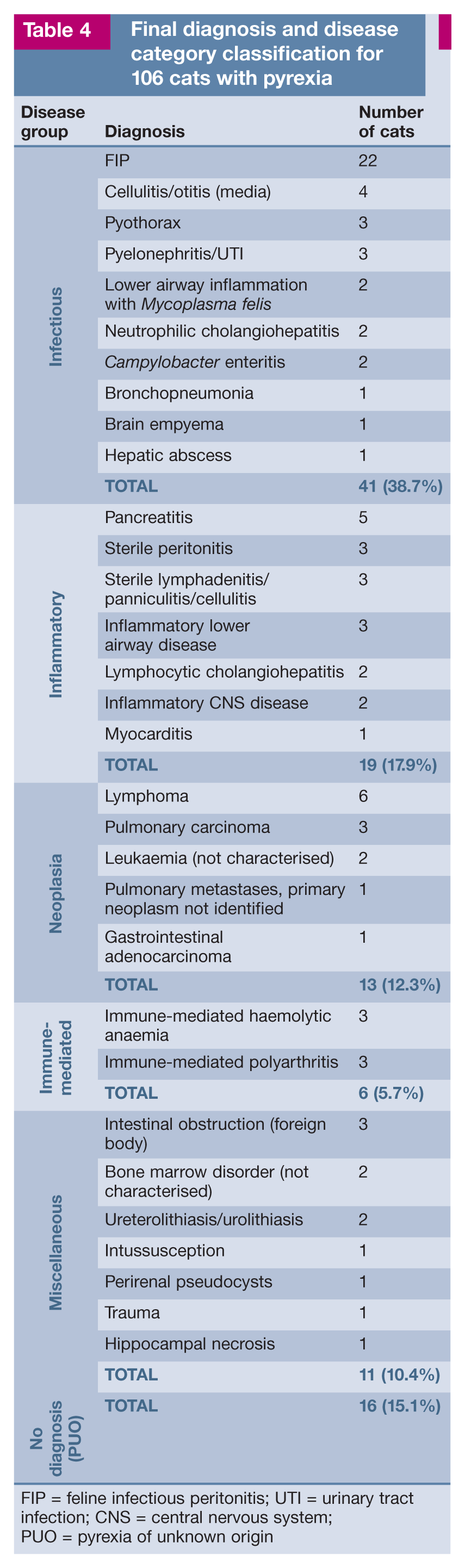
FIP = feline infectious peritonitis; UTI = urinary tract infection; CNS = central nervous system; PUO = pyrexia of unknown origin

Peritoneal fluid from a cat with feline infectious peritonitis (FIP). FIP was the most common condition diagnosed in this study (20.8% of cases)
Median age of 106 cats with pyrexia, as classified by disease category

PUO = pyrexia of unknown origin
Outcome
Cats were hospitalised for a mean of 5.0 days (± 3.2 days). Over two-thirds of cats (71/106, 67.0%) survived to discharge, 31 (29.2%) cats were euthanased and four (3.8%) died during hospitalisation.
Discussion
This is this first published survey describing causes of pyrexia in referred cats. To the authors’ knowledge, there are no similar surveys of pyrexic cats in first-opinion practice. Our study will therefore provide a useful comparison for future, ideally prospective, studies of pyrexic cats in both the first-opinion and referral setting. Using the same grouping system previously described in a canine study, 7 we found infection to be the most common disease category. In contrast, immune-mediated disease was most commonly diagnosed in referral populations of pyrexic dogs.6,7 Infection is the most common cause of pyrexia in people. 2
In terms of specific conditions, FIP was the most common diagnosis. Diagnosis was based on compatible clinicopathological findings and histopathology or positive feline coronavirus immunostaining.10,11 Intermittent fever is one of the earliest signs of FIP, 10 and in one study body temperature exceeded 39.5°C in 81% of cats with FIP, and exceeded 40°C in almost half of the cases. 11 FIP remains a difficult disease to definitively diagnose, perhaps in part due to the fluctuating nature of pyrexia, meaning fever and clinical signs may falsely appear to respond to antimicrobials, delaying investigation and/or diagnosis. The high prevalence of FIP in this population where so many cats had received antimicrobials (± NSAIDs) highlights the condition as being the most common cause of pyrexia refractory to empirical treatment. It is important to note that the prevalence of FIP may be abnormally high as the participating institutions actively participate in FIP research, possibly resulting in a biased population; it has been suggested that differences in disease category prevalence in canine studies has been in part due to particular interests of the authors.6,12
Apart from FIP, few other specific infections were diagnosed in this study, despite FIV/FeLV testing, Toxoplasma gondii serology and other infectious disease PCR tests being commonly performed. This likely reflects the low prevalence of specific infectious diseases in the UK, especially at referral level, although it may also reflect inappropriate test selection by the clinician. The poor overall diagnostic value of routine serological and immunological tests is well recognised in human medicine and there is debate over the minimal serological tests indicated in PUO patients, due to the low prevalence of implicated diseases. 2
Inflammatory (non-infectious) conditions comprised the second-most common disease category in pyrexic cats, and, interestingly, were almost as common as infectious causes when FIP cases were not considered. The widespread use of antimicrobials in this population may have resulted in infectious causes being incorrectly classified as inflammatory (eg, sterile vs non-sterile cellulitis, bacterial vs non-bacterial cholangiohepatitis). This is a limitation inherent in the retrospective nature of the study and may have resulted in an underestimation of infectious disease prevalence.
Neoplasia as a cause for pyrexia was seen in 12.3% of cats, comparable with figures described in pyrexic dogs (9.5% 6 and 7.6% 7 ). Unsurprisingly, as the most common feline neoplasm, lymphoma was the most prevalent neoplasm in this study. Primary pulmonary tumours were the second-most frequent, found in three cats; they have previously been reported to cause pyrexia, 12 likely because of their propensity to become necrotic due to their often large and solid nature.
Immune-mediated disease appears to be a less common cause for pyrexia in cats than in dogs,6–8 with only immune-mediated haemolytic anaemia and immune-mediated polyarthritis diagnosed in our population.
Despite often extensive investigations, a definitive diagnosis was not reached in 15% of cases, comparable to canine studies.6,7 We hypothesise that cats with PUO had selflimiting infections or transient inflammatory foci. In the present study, although most cats were referred without a known diagnosis (and often referred to as having PUO by the referring veterinarian), a cause was found in 85% of cases. The term ‘PUO’ should therefore be reserved for cases where extensive diagnostics have failed to identify the cause. Not all cases of PUO in this study met the definition proposed by Ramsey and Tasker, 1 as only four out of 16 cats had a duration of illness of more than 3 weeks. This is perhaps not surprising as investigations and treatment are likely to be instigated much earlier than 3 weeks in order to reduce patient morbidity.
Due to the retrospective nature of the study and assessment of survival data to discharge only, it was not possible to assess if PUO was associated with outcome. Overall survival to discharge (67.0%) was comparable, however, with a high (70%) survival rate reported in dogs with miscellaneous causes for pyrexia. 6 The majority of humans with PUO will eventually spontaneously recover. 13
No association between treatment and success in reaching a diagnosis was found. Treatment before referral was not associated with temperature at presentation, in contrast to dogs where prior treatment reduced the prevalence of pyrexia at the time of referral. 7 That study also reported that the treatment of pyrexia was associated with a longer time to diagnosis. 7 Because of this, and the proposed protective benefit of pyrexia, it has been recommended to reserve antipyretic drugs for animals where body temperature exceeds 41°C or clinical signs attributable to fever are severe. 1
Broad-spectrum antimicrobials are widely recommended for all cases of unexplained pyrexia in dogs and cats,1,3,12 and, in keeping with this recommendation, antimicrobials were the most commonly administered drugs before referral in this study, given to over 80% of cats. Furthermore, nearly one-third of all cats had received drugs from multiple antimicrobial classes by the time of referral. The prevalence of bacterial infections as a cause of pyrexia in first-opinion veterinary practice may be sufficiently high to warrant such treatment, although no evidence exists to support this. Witholding antimicrobials in stable patients where fever is acute and mild is recommended in human medicine. 13 Of note, despite infections being regarded as (and shown to be in this study) the most common cause of feline pyrexia, almost one-quarter of cats had received corticosteroids before referral.
A wide range of diagnostic investigations were employed to discern the cause of pyrexia. Complete blood count and serum biochemistry were performed in all cases, but the most common abnormalities found (neutrophilia, increased ALT, anaemia and hypoalbuminaemia) were non-specific. Abdominal ultrasonography was the most commonly performed diagnostic procedure that ‘enabled’ or ‘assisted’ with a diagnosis (in over half of the cats in which it was employed). Thoracic imaging (radiography [Figure 3] and/or CT) was performed in over half of cats and appeared to be less useful than abdominal ultrasonography. Echocardiography was performed in approximately one-third of cats, but only assisted with diagnosis in one cat (diagnosed with myocarditis); indeed it was seemingly performed in the majority of cases to assess for concurrent cardiac disease through the detection of a heart murmur or gallop sounds, as well as to assess for endocarditis. Our data suggest that diagnostic imaging selection in pyrexic cats should depend on localising signs (eg, MRI of the brain ‘assisted’ or ‘enabled’ a diagnosis in all cases presented with neurological signs), rather than seeking abnormalities without appropriate localisation.

Lateral thoracic radiograph of a cat diagnosed with pyothorax after presenting with pyrexia. Pyothorax was diagnosed in 2.8% of cases in this population
Fluid (pleural or peritoneal) analysis was a highly useful diagnostic test when performed, likely due to its importance in aiding FIP diagnosis. Cytology (Figure 4) and histopathology were widely employed and were very useful diagnostic procedures, in agreement with canine studies.6–8 Bacterial culture (eg, of fluid, tissue) ‘enabled’ or ‘assisted’ with a diagnosis in approximately one-third of cases in which it was performed, although false-negative results may have occurred due to previous antimicrobial therapy or difficulty in culturing certain organisms (eg, Mycoplasma species). Interestingly, blood culture was performed in only one cat and, even though this test is often recommended when investigating feline pyrexia,3,12 it does not appear to be a principal test required for diagnosis. Feline pancreatic lipase immunoreactivity was performed in over a quarter of cats, likely due to its widespread availability as a bench-side test and due to the non-specific clinical signs of feline pancreatitis (anorexia, lethargy). Its usefulness in obtaining a diagnosis was fairly low, however, perhaps due to pancreatitis being an uncommon cause of pyrexia, and/or due to the test’s limitations in diagnosing chronic or mild forms of the condition. 14

Cytology from a cat diagnosed with renal lymphoma. Cytology was a commonly employed diagnostic test in this study (performed in 40.6% of cases)
The study’s population comprised referral cases and therefore likely contained cases where fever did not spontaneously resolve or respond to empirical treatment, where localising signs were absent, where simple diagnostic tests failed to identify a cause, or alternatively where a diagnosis was known but intensive management was required. Ultimately, many patients were found to have relatively common conditions (eg, pancreatitis, lymphoma, cellulitis) and merely had an unusual or early manifestation of these diseases that hindered diagnosis prior to referral.
Limitations of this study are largely due to its retrospective nature. Future studies should focus on a prospective cohort of cats being referred with pyrexia. A larger number of cases would also enable statistical tests to be performed to further investigate features of the different disease categories and the diagnostic investigations performed. Appropriate cases may have been missed due to the search methods employed (eg, misspelling of pyrexia) and incomplete records meant that some cases had to be excluded. Interpretation of records was required in some instances to determine the final diagnosis and disease category classification. Follow-up data were limited in that only survival to discharge was known in the majority of cases. Finally, despite the endeavour to exclude hyperthermic cats, it is still possible that some cases (particularly cats with respiratory impairment) may have been hyperthermic. Furthermore, a few conditions diagnosed in this study have not been previously associated with pyrexia (eg, renal pseudocysts, uroliths, gastrointestinal foriegn bodies); while it is feasible that pyrexia may occur in these conditions due to inflammation and/or associated infection, hyperthermia cannot be fully excluded. Rectal temperature in healthy cats can reach 39.3°C in the veterinary consultation room due to stress. 15 The inclusion criteria of two or more documented episodes of increased rectal temperature was used in an attempt to exclude cases with stress hyperthermia.
Key Points
This is the first descriptive study investigating cases of feline pyrexia.
A diligent search for an infectious cause, particularly FIP, remains a priority in the investigation of cats with pyrexia.
In contrast to dogs, immune-mediated disease is a rare cause of feline pyrexia.
Abdominal ultrasonography and cytology are likely to be useful and readily available diagnostic procedures.
The administration of more than one antimicrobial class was common in this population.
Footnotes
Acknowledgements
The authors wish to thank Tally Nan and Nora Romero for their help with data collection.
Author note
This paper was presented in part at the 2016 ECVIM-CA Congress.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Date accepted: 26 July 2017