
Abstract
Objectives
The purpose of this pilot study was to evaluate the use of an intramuscular (IM) sedation protocol with butorphanol and alfaxalone in cats undergoing blood donation. We hypothesized that this drug combination would provide sufficient sedation to perform phlebotomy without causing hypotension or significant changes in heart rate.
Methods
Six purpose-bred, healthy adult cats were sedated using IM butorphanol (0.4 mg/kg) and alfaxalone (2–3 mg/kg). Pulse and Doppler blood pressure (BP) were recorded at baseline, after sedation and immediately following phlebotomy. Once laterally recumbent, 12 ml/kg blood was collected from the jugular vein. Sedation scores, duration of lateral recumbency and the ability to successfully perform phlebotomy were recorded.
Results
There was no significant change in heart rate post-sedation (median 190 beats per min [bpm], range 160–224 bpm) or post-phlebotomy (median 200 bpm, range 180–220 bpm) compared with baseline values (median 200 bpm, range 180–220 bpm) (P = 0.395). A statistically significant change in BP was detected (P = 0.029), attributed to a difference between post-sedation (median 113.3 mmHg, range 110.7–130.0) and baseline (median 133.3 mmHg, range 130.0–183.3) measurements. Hypotension was not observed in any cat. Collection of at least 80% of the target volume was achieved in 5/6 cats, although all were adequately sedated to allow jugular venous phlebotomy. Median recumbency time was 53 mins (range 43–83 mins). Phlebotomy duration lasted a median of 13 mins (range 5–21 mins).
Conclusions and relevance
The administration of IM alfaxalone and butorphanol provided sufficient restraint for blood donation without causing hypotension or significant changes in heart rate before or after phlebotomy.
Introduction
Maximizing the safety and comfort of the feline blood donor is a high priority and a challenging task for veterinary practitioners. Although sedation is usually required to facilitate blood donation in cats, formal evaluation of only three drug protocols for sedation/anesthesia of donor cats have been reported in the veterinary literature.1 –3 These studies report the use of intramuscular (IM) benzodiazepine-dissociative combinations with or without butorphanol,2,3 or sevoflurane anesthesia via mask delivery.1,2 In our institution, a protocol of an opioid combined with midazolam–ketamine is presently used to sedate client-owned blood-donor cats. With these drug combinations, sedation is occasionally inadequate or associated with violent or slow recoveries. An ideal protocol for feline blood donors would have a fast onset, sufficient depth and duration of restraint, and a smooth and fast recovery, without hemodynamic instability or other serious adverse effects. These precautions are of particular importance as blood donation involves removal of up to 12 ml/kg (or 20%) of feline blood volume. 1
Alfaxalone is a neurosteroid anesthetic drug used as an induction and maintenance agent for cats and dogs. 4 It is known to cause dose-dependent decreases in cardiac output, heart rate (HR) and mean arterial blood pressure (BP) when used intravenously (IV) at high doses. 5 Evidence from two recently published studies suggests that IM alfaxalone can be used as a safe and effective agent for chemical restraint in healthy cats when used alone or combined with butorphanol.6,7 In these studies, no complications or clinically relevant cardiovascular changes were observed with alfaxalone doses up to 5 mg/kg. This work evaluated the drug(s) in normal cats with presumed normovolemia. The cardiovascular effects of a similar drug combination in cats undergoing collection of up to 12 mg/kg whole blood are currently unknown.
The purpose of this pilot study was to evaluate a combined alfaxalone–butorphanol protocol in six purpose-bred healthy adult cats undergoing blood donation. We hypothesized that butorphanol and alfaxalone given IM would produce effective chemical restraint for at least 20 mins without causing hypotension (Doppler BP <90 mmHg) or bradycardia (HR <140 beats per min [bpm]).
Materials and methods
Six purpose-bred adult mixed breed cats were included in the study. The study protocol was approved by the University of Wisconsin-Madison Institutional Animal Care and Use Committee (protocol V005417). After performing a physical examination, complete blood count and chemistry profile, all cats were deemed to be healthy. Any cat that was found to have microcytosis, presumed to be a sign of iron deficiency related to prior blood sampling, was given a 10 mg/kg IM injection of iron dextran (VetOne Products) 2 days prior to entering the study period. 8
Drug protocol
The drug protocol included one IM injection of 0.4 mg/kg butorphanol (Torbugesic-SA; Zoetis), followed by 2 mg/kg alfaxalone (Alfaxan; Jurox) given IM 15 mins later. If the cat was not recumbent within 10 mins of receiving alfaxalone, a single additional IM dose of 1 mg/kg alfaxalone was administered.
Sedation scoring
Sedation scores were assessed before and after administration of drugs according to a previously published scoring system. 7 Each cat received a score of 0–3 in the categories of posture, behavior and muscle relaxation, with a higher score indicating an increased level of sedation. It was expected that a score of at least 2 in each category, indicating lateral or sternal recumbency, minimal response to femoral pulse palpation, and moderate muscle relaxation, would be required to successfully perform jugular venous phlebotomy for blood donation. The time from administration of the first IM dose of alfaxalone to achievement of this target score was recorded. Duration of recumbency, the amount of time until the cat was standing and able to walk, was also recorded.
Phlebotomy
Once recumbent, a 20 G 1 inch IV catheter was placed in the left or right cephalic vein and blood was collected for measurement of packed cell volume (PCV) and total plasma protein (TPP). The planned phlebotomy volume for each cat was 12 ml/kg, up to 52.5 ml blood for cats weighing >4.4 kg. Immediately prior to blood collection, citrate–phosphate–dextrose–adenine anticoagulant (CPDA-1; Fenwal) was added to each collection system (100 ml double-bag syringe set; Animal Blood Resources International) at a CPDA-1 to blood ratio of 1:7. Each cat was then placed in dorsal recumbency and a 3 × 3 cm area of skin overlying the jugular veins was clipped and aseptically prepared for phlebotomy. The predetermined volume for each cat was collected from the left or right jugular vein over no less than 5 mins. The phlebotomy start and end times and actual volume of blood collected were recorded. The ability to perform a successful blood collection was recorded (yes/no), based on adequate depth and time of sedation. Following phlebotomy and collection of immediate post-phlebotomy vital sign measurements, 20 ml/kg lactated Ringer’s solution (B Braun) was administered IV to each cat over 1 h.
Monitoring
Just prior to drug administration, measurements were recorded for each cat, including rectal temperature, HR, respiratory rate, mucous membrane color, capillary refill time, Doppler BP and arterial hemoglobin saturation (SpO2). Doppler BP (Model 811-B; Parks Medical) was measured as previously described, 9 by collecting five measurements, discarding the highest and lowest values, and averaging the three remaining readings. The SpO2 monitor (Radical7; Masimo) sensor was placed on the contralateral plantar metatarsus or over the coccygeal artery. Measurements were again recorded immediately after each cat achieved the target sedation level, and immediately following phlebotomy. The presence or absence of clinically significant hypotension (Doppler BP <90 mmHg) or bradycardia (HR <140 bpm) was recorded at each post-sedation time point. 10 Vital sign measurements were recorded every 15 mins until each cat was ambulatory, then temperature, pulse and respiratory rates were recorded every 6 h for 24 h. PCV/TPP was again measured at 24 h following blood collection.
Statistical analysis
Data were analyzed using commercially available statistical software (Prism version 6.07; GraphPad Software) and summarized with median and range. Testing for data normality was not performed owing to the small sample size, and non-parametric statistical methods were used. 11 Baseline, post-sedation and post-phlebotomy measurements of HR and BP were compared using the Friedman test; then data at paired time points (baseline vs post-sedation and baseline vs post-phlebotomy) were compared using the Dunn’s multiple comparisons test. P <0.05 was considered statistically significant.
Results
Six cats, one intact male and five intact females, with a median body weight of 4.39 kg (range 3.88–4.54 kg) and age of 12 months (range 12–14 months) were included in the study. Results of baseline blood testing were normal apart from mild anemia in two cats (PCVs of 28% and 29%, respectively) and the presence of microcytosis in all six cats. The median PCV and mean corpuscular volume (MCV) in all cats were 35% (range 28–39%; reference interval [RI] 31–51%) and 36.5 fl (range 31–38 fl; RI 39–50 fl), respectively. Mean cell hemoglobin content was normal in all cats: 37.5 g/dl (range 35–38 g/dl; RI 33–36 g/dl). The median absolute reticulocyte count for cats was 0.021 ×106/μl (range 0.015–0.039 ×106/μl; RI 0–0.052 ×106/μl). All cats received iron dextran (10 mg/kg IM) supplementation, without complication.
The target sedation score was achieved in 3/6 cats with butorphanol 0.4 mg/kg and alfaxalone 2 mg/kg IM, and the remaining cats required an additional dose of 1 mg/kg alfaxalone IM to achieve the same level of restraint. Median time from the first alfaxalone injection to recumbency was 11.5 mins (range 6–20 mins) and duration of recumbency was 53 mins (range 43–83 mins) (n = 6).
Phlebotomy was performed in all cats, obtaining a median of 92.4% (range 47.6–100%) of the target volume. Duration and depth of sedation were adequate to allow phlebotomy in all cats, but technical difficulty limited phlebotomy volumes in 2/6 cats. In the intact male cat, the phlebotomy volume was 47.6% of the target volume, and further data analysis of post-phlebotomy HR, BP and PCV/TPP was not performed in this cat. In the remaining five cats, a median of 95.2% (range 80.4–100.0%) of the target volume could be collected, which equaled 11.3 ml/kg (9.7–12.0 ml/kg). The median duration of phlebotomy was 13 mins (range 5–21 mins) (n = 5) and cats were standing by 15 mins following the end of phlebotomy.
All cats maintained pink mucous membranes with capillary refill time <2 s throughout the study period. Monitoring data are presented in Table 1, including baseline, post-sedation and post-phlebotomy values for HR, BP, SpO2%, respiratory rate and temperature. Individual cat HR and BP data are shown in Figures 1 and 2. There were no significant differences in baseline, post-sedation and post-phlebotomy HRs (P = 0.395). There was a significant change in BP comparing baseline, post-sedation and post-phlebotomy values (P = 0.029). Within these values, post-sedation BP was found to be significantly lower than baseline values. BPs were not different between baseline and post-phlebotomy time points. Neither hypotension nor bradycardia were noted for any cats.
Baseline, post-sedation and post-phlebotomy data

Data are presented as median (range). P values <0.05 are considered significant
P value is reported for statistical comparisons (Friedman test), including five cats that completed at least 80% of planned phlebotomy volume
Significant difference compared with baseline value, as determined by Dunn’s multiple comparisons test
bpm = beats per min; brpm = breaths per min; SpO2 = hemoglobin saturation
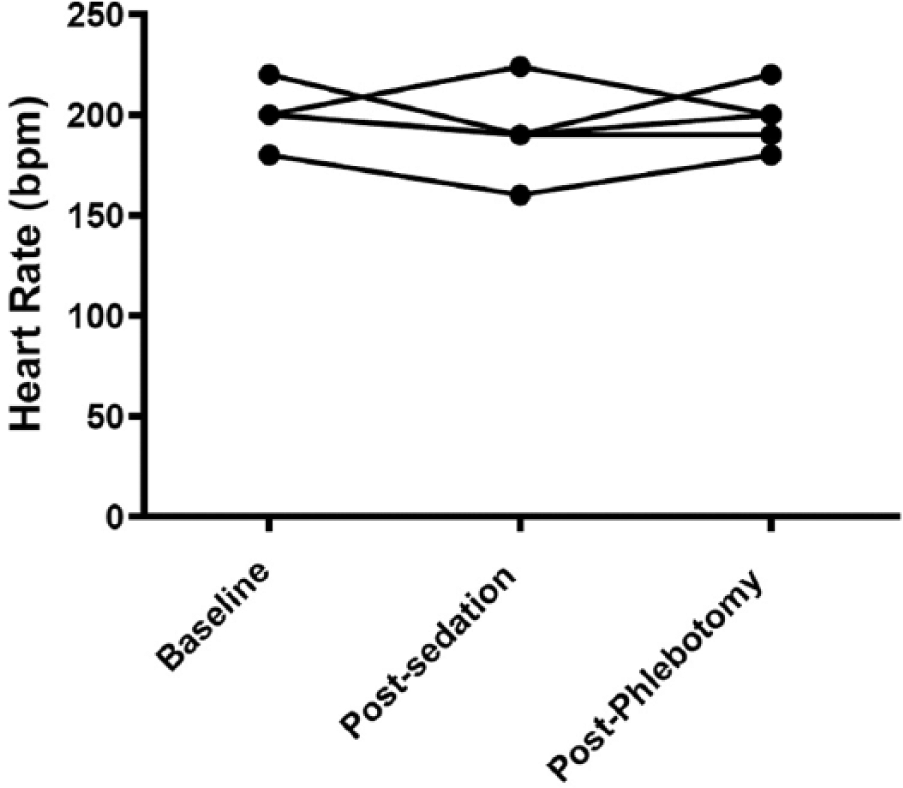
Heart rate data for five cats from which at least 80% of the target phlebotomy volume was collected. bpm = beats per min

Doppler blood pressure (BP) data for five cats from which at least 80% of the target phlebotomy volume was collected. *Significant difference compared with baseline value, as determined by Dunn’s multiple comparisons test
Complications encountered during phlebotomy included difficult venipuncture, slow flow of blood and clotting of blood within the collection set. These complications were attributed to jugular venous anatomy and increased thickness of skin overlying the jugular vein, not sedation. No episodes of rigidity, muscle fasciculation, or signs of aggression were observed in any of the six cats. All cats were eating and drinking and had normal physical examination findings while being monitored for 24 h following phlebotomy. Including only cats that underwent collection of >80% of the target phlebotomy volume (n = 5), the median baseline PCV and TPP were 33% (range 27–40%) and 6.8 g/dl (range 6.0–7.0 g/dl), respectively. The median PCV and TPP at 24 h post-phlebotomy were 28% (range 24–33%) and 6.0 g/dl (range 5.0–6.3 g/dl), respectively (n = 5). Follow-up median PCV and TPP performed 2 weeks later were 35% (range 29–39%) and 7.0 g/dl (range 6.8–7.4 g/dl), respectively.
Discussion
This study reports pilot data which suggests that a sedation protocol using IM butorphanol and alfaxalone is effective for use in blood donor cats, with no adverse effects observed. The combination of alfaxalone (2–3 mg/kg) and butorphanol (0.4 mg/kg) administered IM did not cause significant hypotension or bradycardia. This protocol provided adequate sedation and fast recovery post-phlebotomy. Cats remained in lateral recumbency for a median of 53 mins (range 43–83 mins), which was adequate time to collect a unit of whole blood. A successful donation was completed for 5/6 cats. Although technical difficulties prevented collection of the full unit from the sixth cat, the level of chemical restraint was adequate to permit at least 20 mins of recumbency for phlebotomy in all cats. With this drug protocol, all cats recovered smoothly and quickly and were able to return to normal behaviors such as eating and drinking within 6 h.
The starting doses of alfaxalone were chosen based on the results of previous studies in which alfaxalone was administered IM in healthy, euvolemic cats.6,7,12 As a single agent, Tamura et al 6 studied the sedative and cardiorespiratory effects of alfaxalone in healthy adult cats receiving doses of 1–10 mg/kg IM and 5 mg/kg IV. Cats receiving 2.5 mg/kg alfaxalone IM became laterally recumbent within 7 mins of injection but had no hypotension or significant change in HR. Muscle tremors were observed in 2/6 cats and opisthotonus-like posture occurred in one cat at a dose of 2.5 mg/kg IM, and a higher incidence of hypotension, tremors, opisthotonus-like posture and paddling was observed at doses ⩾5 mg/kg IM. We elected to combine alfaxalone with butorphanol to increase restraint and reduce the incidence of these recovery side effects. Ribas et al 7 demonstrated safe and adequate sedation for cats undergoing echocardiography given IM butorphanol (0.2 mg/kg) and alfaxalone (2 mg/kg). With these doses, cats were laterally recumbent for 36.3 ± 4.4 mins and recovered smoothly. These doses of butorphanol and alfaxalone were tested in one cat prior to this study. This cat failed to allow restraint in lateral recumbency for jugular venous phlebotomy, and the final protocol was adapted to include a higher dose of butorphanol (0.4 mg/kg).
Previous research describing the pharmacokinetics of butorphanol (0.4 mg/kg IM) in cats has demonstrated that the mean time of peak blood concentration (Tmax) was 0.35 h (range 0.25–0.5 h) after IM injection. 13 As alfaxalone produces its peak sedative effect at 10–15 mins after IM injection, 6 we elected to administer butorphanol 15 mins before alfaxalone in order to allow both drugs to reach their peak effect at the same time. This protocol produced a median of 53 mins (range 43–83 mins) of lateral recumbency without episodes of tremors, paddling or rigidity.
Since the sedative and cardiovascular effects of IM alfaxalone were studied only in healthy cats,6,7,12 but not cats undergoing controlled blood loss, the investigators were not comfortable evaluating this drug protocol directly in the donor population. Blood donors at our institution are client-owned cats that are screened for social and calm temperament traits. The purpose-bred cats used in this study were young, healthy and accustomed to human interaction, and were therefore thought to be a close representation of our feline blood donors. Some of the cats were subjectively more active and difficult to restrain than client-owned blood donor cats, which might have led to an increased drug requirement. Differences in personality and required drug doses are expected within a blood-donor population.
Our study demonstrated a significant decrease in BP between the baseline and post-sedation time points, although HR was not significantly different over the same time period. The initially high BP values at the baseline time point (Table 1, Figure 2) are likely related to stress associated with handling and restraint for administering the IM injections. 14 After the cats became sedate, BP decreased significantly to normal values. It is unlikely that the decreased BP is due to hypovolemia, as hypotension was not seen for any cat and HR did not change significantly.
Two cats in this study had mildly reduced baseline PCVs, and all cats demonstrated low MCV prior to inclusion in this study. As the cats had been part of a research colony, it is likely that previous blood sampling had contributed to iron deficiency anemia. Iron-deficient erythropoiesis is common among human blood donors and has also been documented in canine blood donors.15,16 Iron deficiency in feline blood donors has not yet been documented but is suspected to occur. Enteral or parenteral iron supplementation is recommended for cats and dogs with evidence of iron deficiency and for iron-deficient human blood donors.8,15 Cats in this study received a single IM injection of iron dextran to assist in the recovery of red cell mass post-phlebotomy, which would be similar to the treatment approach in feline blood donors with evidence of iron-deficiency anemia.
This study had several limitations. Because no control drug protocol was used, it is not possible to make any conclusions about the relative effects on HR, BP or quality of recovery between the butorphanol–alfaxalone protocol and the standard protocol that is presently in use. An ideal study would compare both protocols using a crossover study design involving double blinding of the investigators and owners of blood donor cats. The sample size was small, with only six cats undergoing sedation and five completing phlebotomy. A power analysis performed prior to this study demonstrated that the use of six cats would detect a decrease in BP of 26 mmHg and an increase or decrease in HR of 30 bpm with 80% power and an alpha level of 0.05. The power of the study was further limited owing to the exclusion of one cat’s HR and BP data because it did not undergo full phlebotomy. The use of non-invasive (Doppler) BP measurement likely limited the accuracy of BP measurements, 17 although the use of gold standard invasive BP measurement did not seem practical in the simulation or the setting of blood donation.
Conclusions
Based on the results of this pilot study, we conclude that the use of 0.4 mg/kg butorphanol IM and 2–3 mg/kg alfaxalone IM appears to provide adequate restraint for cats undergoing blood donation with minimal cardiovascular changes or side effects. It is important to note that all cats in this study were healthy, active and young cats that would likely require higher doses of drugs than might be expected in sick patients. This protocol cannot be extrapolated to cats suffering from critical illness or more severe forms of hypovolemia. Additional studies are required to determine this protocol’s safety in those patient populations.
Footnotes
Acknowledgements
The authors wish to thank Nicole Sinclair CVT, and Kristen Cooley CVT, VTS, for their assistance in completing this research.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.