
Abstract
Objectives
This study aimed to evaluate the acceptance of home blood glucose monitoring (HBGM) by owners of recently diagnosed diabetic cats, and the impact of choosing HBGM on the quality of life (QoL) changes of cat and owner, in addition to glycaemic changes during 6 months of follow-up.
Methods
Owners of cats diagnosed with diabetes mellitus (DM) and treated with insulin for 6–20 weeks were divided into an HBGM group and a non-HBGM group, based on their ability and willingness to perform HBGM after a standardised instruction session. The HBGM acceptance level and reasons for acceptance failure were documented; a questionnaire evaluated owners’ experiences. For the following 6 months, changes in QoL, measured using the validated DIAQoL-pet quantification tool, and changes in glycaemic control parameters (clinical signs, serum fructosamine, blood glucose curve average/minimal/maximal/pre-insulin blood glucose) were compared between HBGM and non-HBGM groups at months 1, 3 and 6, as well as within the groups between baseline and months 1, 3 and 6.
Results
Thirty-eight cats were enrolled; 28 (74%) entered the HBGM group. There was no significant difference between groups in overall DIAQoL-pet score or glycaemic control parameters at any time point apart from the maximal blood glucose at month 6 (lower in the HBGM group). However, the DIAQoL-pet score, including indicators of owner worry about DM, worry about hypoglycaemia and costs, as well as glycaemic parameters, improved at all time points within the HBGM group but not within the non-HBGM group. Remission occurred in 9/28 (32%) HBGM group cats and 1/10 (10%) non-HBGM group cats (P = 0.236).
Conclusions and relevance
HBGM was adopted successfully by most diabetic cat owners. Despite the extra task, positive changes in QoL parameters occurred in the HBGM group and not in the non-HBGM group. Although no difference was found in glycaemic control between the HBGM and non-HBGM groups during the 6 months of follow-up, significant glycaemic improvements were documented in the HBGM group.
Introduction
The management of feline diabetes mellitus (DM) is complex and is facilitated by cat owners understanding the disease and their active participation in treatment. These factors help achieve the main treatment goals, which include resolution of clinical signs and avoidance of hypoglycaemia and diabetic complications.1,2 However, the daily involvement in the management of their pets’ diabetes can also be perceived as a substantial burden by some owners.3,4 A tool called DIAQoL-pet has been developed and psychometrically validated to qualify and quantify the quality of life (QoL) of diabetic pets and their owners, allowing more specific monitoring of this important aspect of feline diabetes, alongside more traditional glycaemic parameters.3,4
Although not considered a main treatment goal,1,2 some diabetic cats enter diabetic remission. The highest remission rates have been reported in cats where good glycaemic control has been established early in the course of the disease.5,6 The role of home blood glucose monitoring (HBGM) in achieving early good glycaemic control has been widely acknowledged and has been included in the latest guidelines for management of DM in cats. 2 In human medicine, self-monitoring of blood glucose (SMBG) has been an integral part of management of humans with type 1 and insulin-treated type 2 diabetes for many decades. 7 However, although the recommendations for treatment of human diabetes emphasise the utility of SMBG to assess individual responses to therapy and prevention of hypoglycaemia, concerns about the potential impacts of SMBG on QoL, particularly in people with type 2 DM, have been raised.8,9 In veterinary medicine, the difficulties pet owners might encounter and the reasons for reluctance to perform HBGM have been sporadically addressed in previous canine and feline studies.10–13 However, these reports were mostly concerned with biological effects as outcome parameters and merely listed what owners perceived as challenges and benefits of HBGM. A prospective assessment of the possible psychosocial impact of HBGM, using an objective validated measure such as the DIAQoL-pet, in a substantial number of patients with a longer-term follow-up is yet to be reported in veterinary medicine.
The main aim of this study was therefore to evaluate the acceptance of HBGM by cat owners and its impact on QoL changes in diabetic cats and their owners over a 6 month period using the previously validated QoL tool, DIAQoL-pet. 3 A secondary aim was to assess the effect of HBGM on glycaemic changes over the same time period.
Materials and methods
Cats diagnosed with DM ⩽5 months previously and treated with insulin for at least 6 weeks prior to enrolment were recruited for the study between October 2013 and September 2015. The study was approved by the institutional Clinical Research and Ethical Review Board and was performed under Home Office Licence number 70/7393. The diagnosis of DM was made based on a combination of appropriate clinical signs (polyuria, polydipsia, polyphagia, weight loss) and laboratory parameters (hyperglycaemia [blood glucose (BG) >15 mmol/l], glycosuria). Cats were excluded if they received short-acting systemic glucocorticoids in the previous month, depot glucocorticoids in the previous 2 months or progestogens in the previous 6 months. Cats were also excluded if they were diagnosed with diabetic ketoacidosis at initial evaluation, if they were diagnosed and treated for hyperthyroidism (except for cats successfully treated with radioactive iodine or thyroidectomy) or were diagnosed with severe disease that could increase the risk associated with study participation or require long-term medication. All cats were screened for hypersomatotropism and if found positive (based on insulin-like growth factor 1 [IGF-1] >1000 ng/ml) 14 were not included.
On initial presentation, a thorough history was taken and physical examination, including body weight (BW), estimation of body condition score (BCS; 1–9/9) 15 and percentage of body fat (% of BF), 16 were performed. The severity of each cat’s clinical signs at trial recruitment was graded using the validated clinical scoring system (Diabetic Clinical Score) shown in Table 1. 17 Cat owners were also asked to complete the DIAQoL-pet survey to assess the influence of DM and its treatment on QoL. 3 The DIAQoL-pet generated an average-weighted impact score to reflect pet and owner QoL, with more negative values reflecting a more negative impact of DM.3,4
Validated diabetic clinical score used to grade the severity of diabetes-associated clinical signs in participating cats

All cats underwent initial screening tests including complete blood count, plasma biochemistry, full urinalysis (including urine culture) and serum fructosamine, total thyroxine, feline pancreatic lipase immunoreactivity (fPLI), IGF-1 measurement and abdominal ultrasound. A 24 h blood glucose curve (BGC) was performed on each cat after admission, using either a continuous glucose monitoring system for the measurement of glucose in the subcutaneous interstitial fluid (Guardian Real-Time system; Medtronic) or serial BG measurements in capillary blood collected from the ear using a portable BG meter (AlphaTrak 2; Zoetis). In the latter case, BG was measured every 2 h or more frequently if hypoglycaemia (BG <3 mmol/l) occurred. All cats were then transitioned onto a longer-acting insulin type (recombinant human protamine zinc insulin [PZIR (ProZinc; Boehringer Ingelheim)] or synthetic insulin analogue glargine [Lantus; Sanofi]) at an initial dose of 0.2–0.7 U/kg. Cats were fed a low-carbohydrate, high-protein diet (Purina Pro Plan DM; Nestle Purina PetCare [wet or dry, depending on cat’s preference]), which commenced at least 10 days prior to the enrolment visit.
At discharge from the hospital, all cats received a comprehensive introduction to HBGM, which took at least 30 mins. Owners were shown how to obtain a blood drop using the marginal ear vein technique and they practised the technique on their own cat with the clinician. Cat owners were also taught how to use the glucometer for measurement and how to calibrate it. To generate data for a BGC, owners were asked to measure BG every 2 h over a 12 h period, starting just before morning feeding and insulin injection, and finishing just before evening feeding and insulin injection. Owners were asked to record the data and send the results to the research clinic and describe any clinical signs of diabetes that occurred around the time of the BGC. Owners were asked to perform a BCG at the 1 week and 2, 4 and 5 month trial time points, and also 1–2 weeks after any insulin dose adjustments. If owners did not perform HBGM, it was requested that these BGCs were performed at the cat’s primary-care practice. Cats that entered diabetic remission were initially monitored using spot blood glucose checks 2–4 times weekly, but spot blood glucose measurements were not otherwise routinely requested for monitoring.
Re-examinations at the research clinic were performed 2 weeks, 1 month, and 3 and 6 months after joining the trial. At these time points, a full history and physical examination, serum fructosamine measurement, diabetic clinical score (DCS) and a 24 h BGC were performed in all cats. Owners were also asked to complete the DIAQoL-pet survey. Additional monthly to bimonthly re-examinations took place at the referring veterinary practices, depending on the needs of individual cats. During the study, insulin dose was adjusted according to a single, nadir-led protocol, based on BGC results. 17 Diabetic remission was defined as not requiring insulin for more than 4 weeks.
Owners were considered to have successfully adopted HBGM (‘HBGM group’) if they had performed a minimum of two BGCs at home within the first 3 months of enrolment. The remaining owners and their cats were included in the ‘non-HBGM group’. This arbitrary cut-off of two BGCs was chosen, as the investigators explicitly did not want to include owners in the HBGM group if they had successfully performed one curve, and decided against further testing as a result of this experience.
At the end of the study period, owners were contacted by email and/or telephone and asked to complete a questionnaire to describe their experiences with HBGM. The owners of cats included in the HBGM group were asked about their general opinions of HBGM (eg, if their lives were restricted by HBGM; advantages/disadvantages of HBGM), the technique used for generating the BGCs, and difficulties they encountered during HBGM (supplementary material 1). The owners of cats in the non-HBGM group were asked why they decided not to perform HBGM, or, if they performed some monitoring but then discontinued, why they discontinued (supplementary material 2).
Statistical analysis
The data were tested for normality where appropriate (Shapiro–Wilks test). Signalment, BW, BCS, % of BF, fPLI, total number of BGCs performed during the study period, the time on insulin prior to enrolment, insulin type choice (PZIR vs glargine) and the insulin dose at enrolment were compared between cats in the HBGM group and non-HBGM group using Mann–Whitney and χ2 tests, as appropriate. To evaluate the impact of HBGM on QoL changes in diabetic cats and owners, total DIAQoL-pet score and individual item-weighted impact scores (IWIS) for specific questions (Table 2) were compared between the HBGM group and the non-HBGM group at enrolment and 1, 3 and 6 months after joining the trial. Similarly, DCS, twice-daily insulin dose and parameters of glycaemic control (serum fructosamine, average BG, average pre-insulin BG, minimal and maximal BG) were compared between the HBGM and non-HBGM groups at the same time points. Remission rate between groups (HBGM vs non-HBGM group) and the effect of the insulin type used (PZIR vs glargine) on whether owners achieved HBGM were compared using χ2 tests.
Overview of questions (items) of the DIAQoL-pet survey, 3 pertinent with regard to home blood glucose monitoring

Each item was scored according to frequency at which it impacted on owners’ and pets’ lives (all the time [3], often [2], occasionally [1], never [0]) and how important the item was in the individual owner’s and pet’s lives (very important [4], important [3], moderately important [2], low importance [1], not at all important [0]). Item-weighted impact score was calculated for each item by multiplying frequency and importance ratings for each question
DIAQoL-pet score, IWIS for specific questions (as above), DCS, insulin dose and parameters of glycaemic control (as above) were compared within each group to assess changes in QoL and glycaemic control over time. Wilcoxon signed ranks test were used to compare values at months 1, 3 and 6 to baseline (enrolment) values.
Statistical analysis was performed using commercially available statistical software (SPSS version 22; IBM Statistics).
Results
Sixty-three cats were initially screened prior to enrolment in the 6 month trial and 46 cats were enrolled. Reasons for exclusion of the 17 cats were as follows: neoplastic disease/mass lesion (n = 4); probable hypersomatotropism (on the basis of IGF-1 >1000 ng/ml; n = 3); excessively fearful or aggressive cats (n = 3); cats already non-insulin-dependent based on an in-hospital BGC (n = 2); hyperthyroidism (n = 1); gastrointestinal disease (n = 1); clinical signs suggestive of a forebrain disease (n = 1); hypertrophic cardiomyopathy with congestive heart failure (n = 1); and cat owners declining study enrolment due to time constraints (n = 1).
Among the 46 cats enrolled in the 6 month trial, eight were already performing HBGM, leaving 38 cats for study inclusion. Owners of 28 cats (74%) were able to perform HBGM (HBGM group). The remaining 10 cats (26%) were included in the non-HBGM group.
There was no significant difference in the signalment, BW, BCS, % of BF, fPLI, time on insulin, insulin dose prior to enrolment and choice of insulin (PZIR vs glargine) between cats in the HBGM- and non-HBGM groups (Table 3). In the non-HBGM group, 90% cats (n = 9) were male neutered vs 46% (n = 13) in the HBGM group (P = 0.025).
Comparison of the demographic data, DIAQoL-pet score (quality-of-life tool) and parameters of glycaemic control (diabetic clinical score [DCS]; serum fructosamine; average blood glucose based on blood glucose curve) between the home blood glucose monitoring (HBGM) and non-HBGM group at enrolment, and at months 1, 3 and 6

Data are median (range) unless otherwise indicated
Cats in the HBGM group had a median of five (range 2–10) BGCs performed at home, whereas cats in the non-HBGM had a median of 2.5 (range 1–7) BGCs performed at their primary veterinary practices during the 6 month follow-up period. Each cat had an additional four (range 2–4) BGCs performed at the research clinic during the same time period. The total number of BGCs (including curves performed at home, at the primary veterinary practices and at the research clinic) was not significantly different between the HBGM and non-HBGM groups (P = 0.082).
There was no difference between the HBGM and non-HBGM groups with regard to the total DIAQoL-pet score, scores for specific questions, DCS, insulin dose, or parameters of glycaemic control at any time point during the study, except for maximal BG at month 6, which was lower in the HBGM group (P = 0.03; data shown in supplementary material 3 (Figures 1–3, Table 3). Total DIAQoL-pet score was significantly improved at months 1, 3 and 6 compared with baseline in the HBGM group but not in the non-HBGM group (Figure 1, Table 4). There were significant decreases in scores (and therefore positive impact) for general worry about diabetes (‘worry’; months 1, 3 and 6) and worry about hypoglycaemia in particular (‘worry hypo’; months 3 and 6), and worry about costs (months 3 and 6) in the HBGM group. There were also significant decreases in scores (indicating positive impact) for ‘restriction of owners’ activities’ and ‘work restrictions’ (month 6) in the HBGM group (Table 4). Overall, the scores for 6/9 specifically examined QoL areas had improved at month 6 vs baseline in the HBGM group (Table 4) but not in the non-HBGM group (supplementary material 4). There were also significant reductions (ie, improvements) in DCS, insulin dose and most parameters of glycaemic control (fructosamine, average BG, average pre-insulin BG, minimal/maximal BG) at months 1, 3 and 6 compared with baseline in the HBGM group (Figures 2 and 3, Table 5), except for minimal BG at months 3 and 6. In the non-HBGM group, DCSs also decreased at months 1, 3 and 6 vs baseline (P <0.05). Regarding insulin dose and parameters of glycaemic control in this group, only average pre-insulin BG at month 6 and maximal BG at month 1 were significantly different (lower; P <0.05) from baseline (supplementary material 5). Diabetic remission occurred in 9/28 (32%) cats in the HBGM and 1/10 (10%) cats in the non-HBGM group (P = 0.236).

DIAQoL-pet score (quality-of-life tool) in the home blood glucose monitoring (HBGM) and non-HBGM groups over the 6 month study period. Higher scores are suggestive of better quality of life. Circles/squares and error bars represent median and range. Significantly different values (P <0.05) are marked with an asterisk
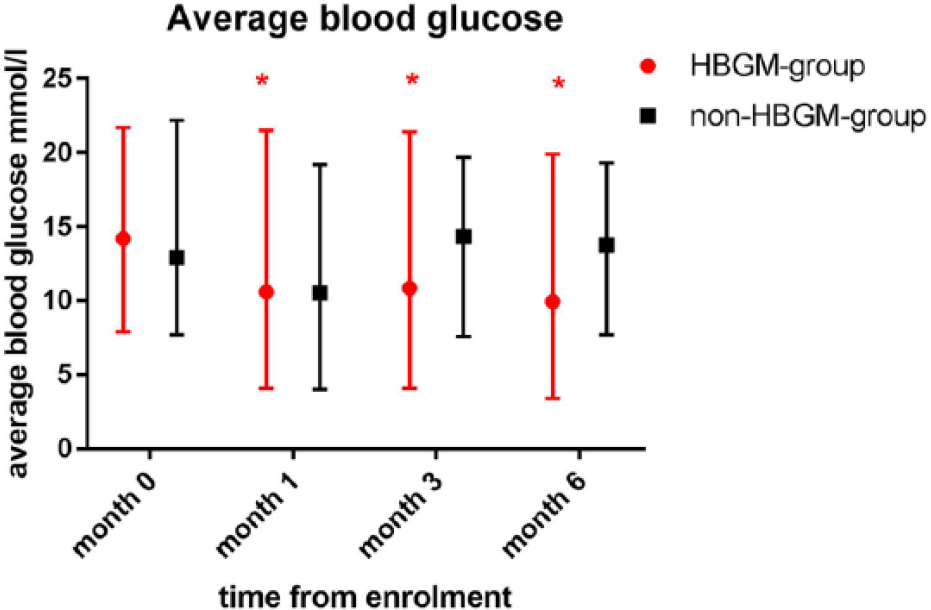
Average blood glucose (obtained from 24 h blood glucose curves) in the home blood glucose monitoring (HBGM) and non-HBGM groups over the 6 month study period. Circles/squares and error bars represent median and range. Significantly different values (P <0.05) are marked with an asterisk. Average blood glucose was significantly lower at months 1, 3 and 6 compared with baseline in the HBGM group but not in the non-HBGM group. There were no significant differences in average blood glucose between the groups at any time point

Serum fructosamine concentration in the home blood glucose monitoring (HBGM) and non-HBGM group over the study period. Circles/squares and error bars represent median and range. Significantly different values (P <0.05) are marked with an asterisk. Serum fructosamine concentrations were significantly lower at months 1, 3 and 6 compared with baseline in the HBGM group but not in the non-HBGM group. There were no significant differences in serum fructosamine concentrations between the groups at any time point
Comparison of DIAQoL-pet (quality-of-life tool), including specific questions (see below), between enrolment and months 1, 3 and 6 within the home blood glucose monitoring group

Value is significantly different from enrolment (month 0) at a level of significance P <0.05
Value is significantly different from enrolment (month 0) at a level of significance P <0.01
Value is significantly different from enrolment (month 0) at a level of significance P <0.001
Value is significantly different from enrolment (month 0) at a level of significance P <0.0001
Comparison of parameters of glycaemic control at different time points within the home blood glucose monitoring group

DCS = diabetic clinical score; BG = blood glucose; BW = body weight
Value is significantly different from enrolment (month 0) at a level of significance P <0.05
Value is significantly different from enrolment (month 0) at a level of significance P <0.01
Value is significantly different from enrolment (month 0) at a level of significance P <0.001
Value is significantly different from enrolment (month 0) at a level of significance P <0.0001
Nineteen (68%) questionnaires were completed by owners of cats in the HBGM group. Ten of the 19 (53%) owners performed >10 BGCs and 17/19 (89%) found HBGM ‘straightforward’ or ‘mostly straightforward’ to perform; 2/19 (11%) respondents described it as ‘difficult’. Technical difficulties (pricking the ear, obtaining sufficient blood) were the most common challenges reported by 10/19 (53%) owners, followed by finding time to perform HBGM (n = 6/19; 32%), and gaining confidence (n = 5/19; 26%). Ten of the 19 (53%) respondents felt that their lives were not at all/not really restricted by HBGM, whereas 6/19 (32%) and 4/19 (21%) reported mild or moderate restriction, respectively. Most owners mentioned several advantages of HBGM; not having to take their cat to the veterinarian (n = 16/19; 84%) or leave the cat at the practice (n = 11/19; 58%) were the most commonly reported. A summary of the advantages and disadvantages of HBGM, and a description of the technique and difficulties encountered during HBGM, can be found in Table 6. Of cats in the HBGM group that were alive at the time of writing, all owners were still performing HBGM.
Summary of advantages and disadvantages of home blood glucose monitoring (HBGM), as well as description of the technique and difficulties encountered during HBGM

Number and percentage of respondents (of 19 returned questionnaires) given in parentheses after the item
Three of 10 questionnaires in the non-HBGM group were completed. Two owners managed to perform a few spot blood glucose measurements but not a whole curve; one owner tried performing curves but did not succeed. The reasons for discontinuing HBGM were stated as lack of assistance (n = 2); a perception that the cat was anxious (n = 3); difficulties obtaining a blood drop (n = 2) or using a glucometer (n = 2); and the perception that he/she was hurting the cat (n = 1). Despite not being successful, one owner expressed a desire to try HBGM again, whereas the other two would ‘probably not’/‘not’ try it again.
Discussion
The main aim of this study was to determine the acceptance of HBGM, and especially its impact on the QoL of diabetic cats and their owners. Although no significant difference in the overall QoL assessed by the DIAQoL-pet tool was found between the HBGM and non-HBGM groups during the 6 months study period, the overall QoL scores improved at all post-enrolment time points in the HBGM group and not in the non-HBGM group. This suggests a possible positive impact of HBGM. The acceptance of HBGM by the owners of diabetic cats was high, with approximately 3/4 successfully adopting HBGM. This proportion is similar or higher than in previous studies evaluating HBGM in diabetic cats.11,12 Importantly, 89% of those performing HBGM found it ‘straightforward’ or ‘mostly straightforward’ and all questionnaire respondents in the HBGM group would recommend HBGM to all or at least some owners of diabetic cats. Based on the questionnaire results, for owners practising HBGM, the benefits clearly outweighed any disadvantages. Notably, about half of the owners in the HBGM group stated that they did not feel their lives were restricted by HBGM. This was in agreement with the results of the DIAQoL-pet assessment, indicating improvement of the overall QoL in the group performing HBGM. Further, owners practising HBGM reported significantly less worry about their cat’s diabetes in general, and particularly about hypoglycaemia, compared with before the trial. This might be owing to feeling more in control because of the ability to check blood glucose at home, as has been previously reported. 11 The scores of specific questions about possible restriction of owners’ lives (‘restrict your activities’, ‘social life’, ‘working life’) did not reveal negative effects associated with HBGM vs the non-HBGM group. The item ‘costs’ also improved over time in the HBGM group, but not in the non-HBGM group, possibly reflecting cost savings because glycaemic checks were performed at home rather than at the veterinary clinic.
The psychometrically validated DIAQoL-pet tool was used to objectively evaluate QoL in diabetic cats and their owners. Although other factors might have contributed to the score, successful adoption of HBGM was the major difference in the diabetes management after enrolment on the study. It is therefore likely that any negative impact HBGM might have had on the QoL would have been reflected in deterioration of the total DIAQoL-pet score or in the scores for the specific questions mentioned above. As an improvement in DIAQoL-pet score occurred, HBGM was considered to most likely have a positive effect on QoL, rather than imposing an additional burden. In fact, owners of cats in the HBGM group reported an improvement in impact on DIAQoL-pet factors relating to life and work restrictions once the trial had started. This improvement was not documented in the non-HBGM group.
Although improvement in QoL was documented in the HBGM group and not in the non-HBGM- group over time, the QoL scores were not different between these two groups at any time point in the study. There might be several reasons for this lack of statistically significant difference. First, the non-HBGM group was smaller than the HBGM group; second, the trial design resulted in cat owners essentially self-selecting group assignments; third, the HBGM group was not absolutely homogenous in terms of the frequency and intensity of performing HBGM. However, the total number of BGCs was not significantly different between the HBGM and non-HBGM groups. Finally, lack of randomisation and owners’ self-assignment to the groups might allow for owner- or pet-related characteristics, intrinsic to the decision to accept or decline HBGM, to confound treatment outcomes. For instance, if owners of cats in the HBGM group were more motivated to do everything possible to control their cat’s diabetes, better treatment outcomes might be expected in that group. Nevertheless, owners in both groups were prepared to follow the other aspects of the clinical trial, which included regular visits to the research clinic, indicating that even the owners in the non-HBGM group were committed to the care of their diabetic cat. Additionally, assigning owners to one of the two groups, and thus forcing some of them to accept HBGM, would not be feasible or ethical. On the basis of direct comparison of QoL and glycaemic parameters, the two groups were very similar at enrolment, further strengthening the validity of the comparisons drawn.
We used a questionnaire to assess the cat owners’ experiences with the HBGM. Although closed-ended questions offering fixed answer(s) were used, the option ‘other’ was included in most of the questions, to enable owners to provide additional free text information. Using open-ended questions might have been more suitable to assess the owners’ opinions on some issues (eg, advantages/disadvantages of HBGM) without introducing bias. However, using open-ended questions is also associated with higher risk of larger item non-response or invalid answers, resulting in missing data. 18 Therefore, we compromised by including the option ‘other’.
The maximal BG at month 6 was significantly lower in the HBGM group compared with the non-HBGM group. Additionally, in the HBGM-group, all glycaemic control parameters (except for minimal BG at months 3 and 6) decreased significantly compared with enrolment values. In contrast, in the non-HBGM group, improvement in only two glycaemic control parameters (maximal BG at month 1 and average BG at month 6) was identified, and there was no consistent pattern for the remaining parameters. Nevertheless, it should also be emphasised that when performing a direct comparison between cats in the HBGM- and non-HBGM groups, a statistically significant difference was not shown at any time point during the study. Superior glycaemic control has been linked with higher remission rates. 19 Also, HBGM was an essential part of management in studies reporting the highest remission rates.5,6 Interestingly, 9/28 (32%) cats in the HBGM group underwent diabetic remission, but this occurred in only 1/10 (10%) cats in the non-HBGM group. However, the difference between groups in remission rates was not statistically significant. Large randomised prospective studies are recommended to further investigate the impact of HBGM on remission rates.
Finally, random assignment of owners and cats to equally sized HBGM- and non-HBGM groups might have yielded superior results in this respect. Given the importance of HBGM suggested in previous studies,5,6 our research group, guided by our ethical committee, considered that it would be inappropriate to not actively offer HBGM to owners as part of best clinical practice. Conversely, forcing owners, who could not or did not want to perform HBGM, to enrol in the HBGM group would not be feasible or ethical either. Although this approach might have introduced selection bias into the study, this situation is more likely to reflect the ‘real-life’ circumstances when, ideally, all owners should be able to make an informed choice about the protocol they use to manage their cat’s diabetes.
Conclusions
Most (n = 28/38; 74%) owners of diabetic cats were able to perform HBGM and the majority (n = 17/19; 89%) considered it to be (mostly) straightforward. Overall QoL evaluated by the validated psychometric tool DIAQoL-pet improved significantly in cats/owners choosing to perform HBGM. Specifically of interest was an owner-reported decrease in worry about the diabetes and particularly hypoglycaemia in the HBGM group, which did not occur in the non-HBGM group. This study adds to the body of peer-reviewed evidence that suggests HBGM is a practical monitoring tool for many owners of diabetic cats and suggests it is associated with a positive impact on QoL in both the diabetic cat and the owner. Further studies are warranted to assess its possible positive impact on glycaemic control.
Supplemental Material
Click here for Supplement 1
Questionnaire about owner’s experience with home blood glucose monitoring (HBGM) – HBGM group
Supplemental Material
Click here for Supplement 2
Questionnaire about owner’s experience with home blood glucose monitoring (HBGM) – non-HBGM group
Supplemental Material
Click here for Supplement 3
Supplementary material to Table 3
Supplemental Material
Click here for Supplement 4
Comparison of DIAQoL-pet at different time points within the non-home blood glucose monitoring group
Supplemental Material
Click here for Supplement 5
Comparison of parameters of glycaemic control at different time points within the non-home blood glucose monitoring group
Footnotes
Acknowledgements
The authors thank all diabetic cats and their owners who participated in this research.
Author note
Part of this study was presented as an oral abstract presentation at the 25th ECVIM-CA annual congress in 2015 in Lisbon, Portugal.
Supplementary material
Supplement 1: Questionnaire about owner’s experience with home blood glucose monitoring (HBGM) – HBGM group.
Supplement 2: Questionnaire about owner’s experience with home blood glucose monitoring (HBGM) – non-HBGM group.
Supplement 3: Supplementary material to Table 3.
Supplement 4: Comparison of DIAQoL-pet at different time points within the non-home blood glucose monitoring group.
Supplement 5: Comparison of parameters of glycaemic control at different time points within the non-home blood glucose monitoring group.
Conflict of interest
This research was supported by Zoetis, which sells glucometers for use in dogs and cats. However, under the Royal Veterinary College’s Code of Research Conduct, the authors performed the research entirely independently, and did not allow external influence over the generation, reporting or interpretation of the results published in this paper.
Funding
This research was supported by funding from Zoetis. The glucometers and home blood glucose monitoring disposables were provided by Zoetis. The research clinic also receives funding from Boehringer Ingelheim and Nestlé Purina PetCare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.