
Abstract
Practical relevance:
Although most skin lesions occur due to diseases primarily affecting the skin, some reflect important systemic diseases. Such lesions may relate directly to the systemic disease, or may occur due to secondary skin diseases that develop because of immunosuppression. Early recognition of skin changes as a marker of systemic disease will maximise patient outcomes.
Clinical challenges:
In older or clearly debilitated cats presenting with skin disease, the potential for underlying systemic disease is often readily apparent. Similarly, cats presenting with severe ulcerative or multifocal nodular skin lesions, or with concurrent signs of systemic illness, will more instinctively prompt systemic evaluation. More challenging is the cat presenting with alopecic, scaling, erythemic and/or mildly crusted skin disease, with or without pruritus; hypersensitivities and infectious dermatoses are the most common considerations, but occasionally systemic disease underlies the skin changes. Knowing when screening laboratory testing, body imaging or other systemic diagnostics are indicated is not always straightforward.
Evidence base:
This article reviews cutaneous presentations of systemic diseases reported in the veterinary literature, and discusses important differential diagnoses. The author draws on clinical experience, published data on disease prevalence and case evaluations, and expert opinions on approach to common systemic problems to provide guidance on when investigation for underlying systemic disease is most appropriate.
Skin is the largest and most accessible body organ, and skin disease is common and readily visualised. Skin disease in cats, as for many mammals, most frequently occurs due to diseases specifically or primarily targeting the skin, but will sometimes reflect important underlying systemic illness. Healthy skin is dependent on good general body health, and any cause of suboptimal health can result in skin and haircoat impairment. In addition, some systemic diseases may produce early or characteristic skin lesions that provide very useful diagnostic clues. However, many skin lesions are non-specific, and occur in a wide range of skin diseases.
Careful screening of history and complete body physical examination in cats presenting with skin disease often provides the most useful clues to the potential for underlying systemic disease. Awareness of the possible role of systemic immunosuppression in the development of some infectious skin diseases is also important. Early recognition of some skin presentations as markers of systemic disease aids optimal patient outcomes.

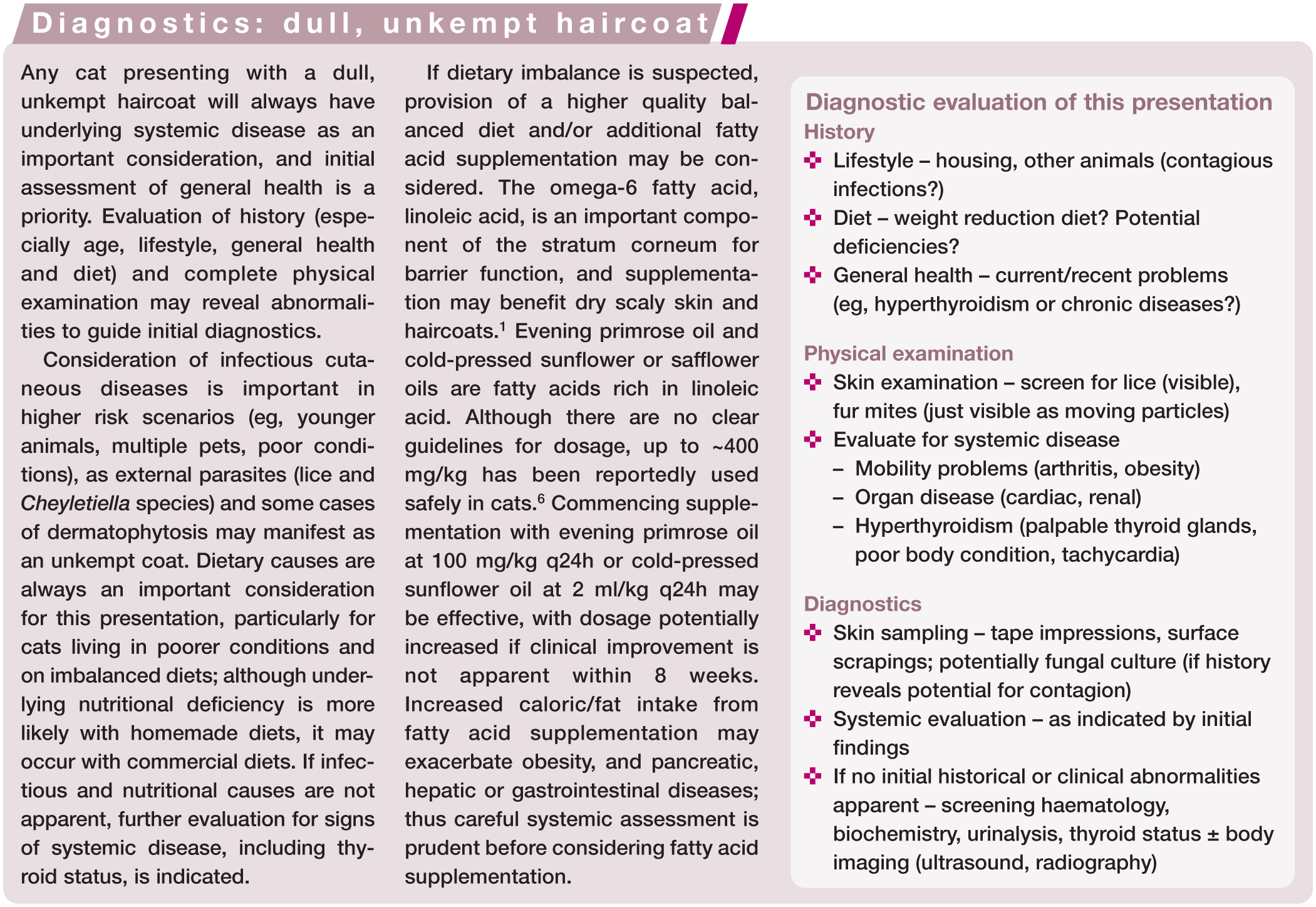
The cat with a dull, unkempt haircoat
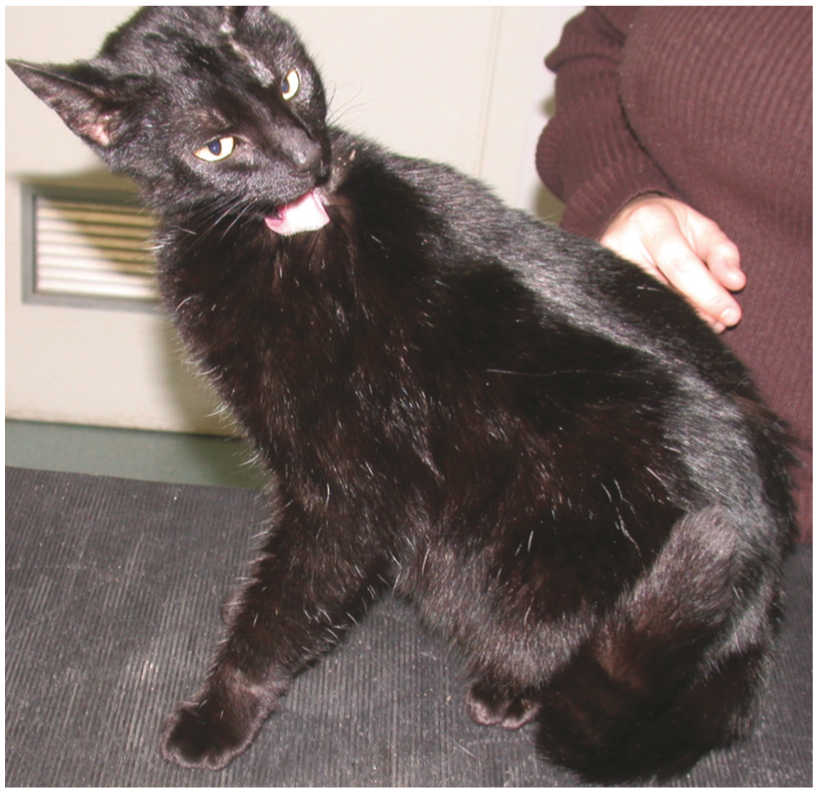
Generalised or regional changes in haircoat quality in a cat with a previously healthy coat frequently reflect systemic problems, and screening for other signs of systemic illness is indicated. Haircoats may be dull (loss of normal sheen) (Figure 1), with variable degrees of oiliness, hair matting, tufts of unshed hair and scaling, reflecting a range of systemic problems.
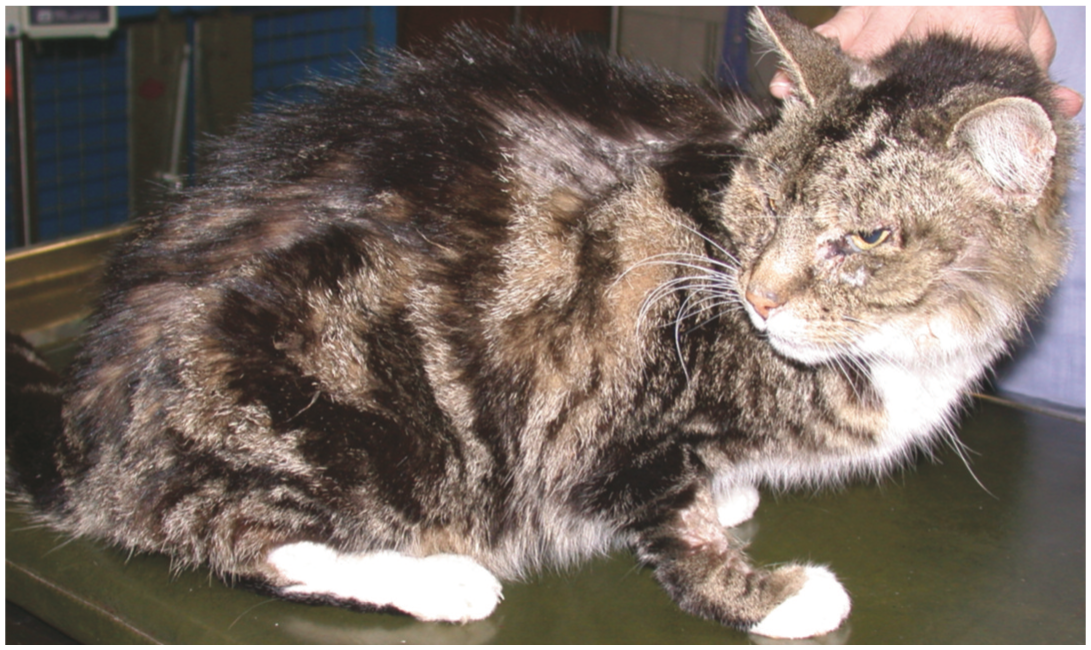
Unkempt (dull, dishevelled and matted) haircoat in a cat
Nutritional deficiencies
Essential fatty acid deficiency can lead to a dull scaly haircoat in cats.1,2 Dietary deficiency can occur with diets that are poorly stored (eg, high temperatures), have inadequate antioxidants to prevent rancidity, or are homemade and imbalanced; deficiency may also be caused by long-term use of commercial weight management diets in some patients, or commercial diets not meeting their nutritional label claims.1,3 Other, very rare dietary deficiencies (eg, protein, vitamin [A, E, B2, B6, biotin] or mineral [zinc, phosphorus]) may result in skin or haircoat changes. 1
Reduced ability to groom
A range of chronic systemic problems can reduce grooming ability, which may impact normal skin and haircoat appearance. Obesity, physical pain (arthritis, oral cavity diseases), and lethargy or malaise from a variety of chronic diseases (eg, cardiac, renal, hepatic) are all considerations.
Hyperthyroidism
Cutaneous changes reportedly occur in 30–40% of cats with hyperthyroidism, 4 although may be under-reported when present along with more prominent signs. An unkempt, matted or greasy haircoat is most common, presumed to reflect reduced grooming activity. Regional or extensive alopecia from excessive grooming is also reported. Prominent claw growth may be apparent. 5 Skin changes are generally subtle, and cats typically present with systemic signs of disease, including weight loss despite polyphagia, behavioural changes/hyperactivity, polydipsia and gastrointestinal signs (vomiting, diarrhoea or voluminous faeces).
Disease may be first apparent in cats presenting for routine health screening/vaccination. Physical examination will often reveal poor body condition, an unkempt haircoat, palpably enlarged thyroid glands (80–90% of cases) and tachycardia (48% cases). 4
Hypothyroidism
Hypothyroidism is increasingly recognised in cats following treatment for hyperthyroidism (surgical or radioactive iodine). Naturally occurring disease is extremely rare (congenital dwarfism in young kittens; one published spontaneous case in an adult cat 7 ). The most common signs are lethargy, reduced appetite, weight gain, and subtle skin changes including dull haircoat with scaling, hair matting and excessive shedding. 8 Regional alopecia affecting pinnae, pressure points and the caudal back is reported. 5 Treatment requires adequate thyroid hormone supplementation.
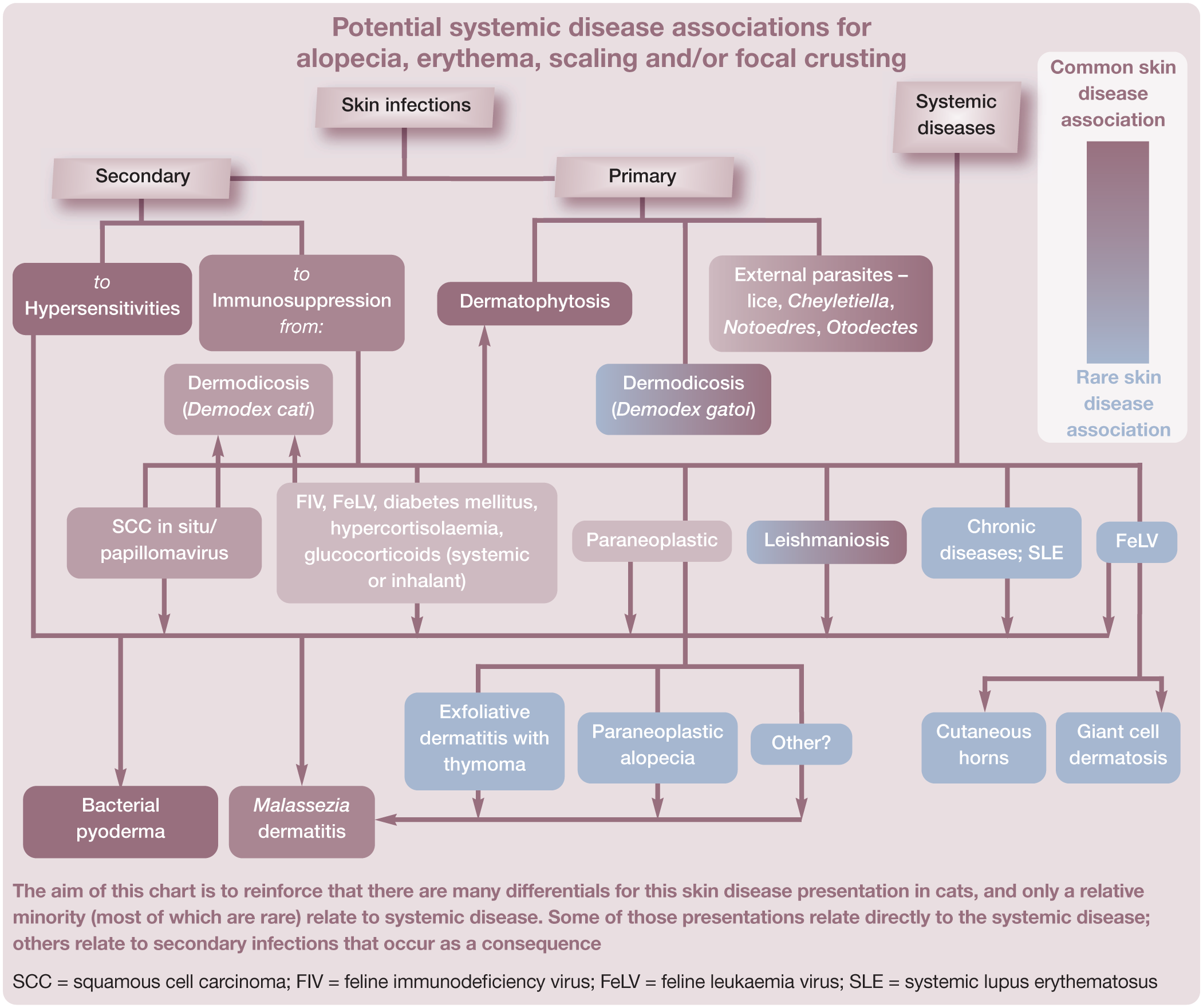
The cat with alopecia, erythema, scaling and/or focal crusting
Skin disease with prominent alopecia, erythema and/or scaling is among the most common cutaneous presentations in cats, and is associated with a wide range of differentials. Mild focal crusting may be present, and variable pruritus (absent/unapparent to severe). Hypersensitivities (see ‘the cat with pruritus’ later) are common causes of this presentation (Figure 2), along with a range of primary and secondary skin infections including those caused by dermatophytes, external parasites (Demodex, Otodectes, Cheyletiella) and secondary bacteria or Malassezia species. Pemphigus foliaceus, the most common autoimmune dermatosis in cats, 9 is another consideration for crusting presentations. Systemic diseases may produce alopecic, erythemic, scaly and/or focally crusted skin lesions, and some distinct presentations are recognised.

Fairly well-demarcated area of alopecia, erythema and focal crusting on the dorsal neck of a Himalayan cat with atopic dermatitis
Secondary bacterial pyoderma and Malassezia species dermatitis
Bacterial pyoderma is now recognised as a common secondary skin disease in cats, particularly with underlying hypersensitivity, but is also associated with immunosuppression from systemic disease or from drug therapies.10,11 Limited assessment of non-allergic disease associations is published to date, but pyoderma in cats is likely to occur with a broad range of naturally occurring or iatrogenically induced immunosuppressive conditions. As in dogs, bacterial pyoderma in cats may present with a wide variety of skin lesions, including alopecia, erythema, scaling, papules, crusted papules (miliary dermatitis), erosions, ulceration and crusting. Distribution is usually multifocal, with the face (Figure 3), neck, ventral trunk and limbs being commonly affected areas. 10 Deep pyoderma occurs rarely in cats, presenting as nodular and draining lesions.

Asymmetrical well-demarcated region of alopecia, erythema and mild focal crusting involving the dorsal nasal planum and adjacent facial skin, due to secondary bacterial pyoderma in a domestic shorthair cat
Malassezia dermatitis is less common in cats than bacterial pyoderma. Although early reports suggested a greater association with systemic diseases, including feline immunodeficiency virus (FIV) infection, thymoma and paraneoplastic alopecia, Malassezia infection is now also well recognised with underlying hypersensitivities. 12 It can present with localised, multifocal or occasionally generalised areas of alopecia, erythema, greasy adherent brown scaling, and red-brown skin discolouration. The face, chin, pinnae, ventral neck, ventral trunk, interdigital areas and claw folds are the more commonly affected sites. 12
With both infections, pruritus may be produced independently of the underlying disease. Initial antimicrobial therapies are important to resolve many established secondary infections, and management of the underlying problem is crucial to ongoing control.
Demodicosis (Demodex cati)
Classical demodicosis, associated with the follicular mite Demodex cati, is rare in cats. However, it is a hallmark for immunosuppression from underlying systemic disease or drug therapies, and has been reported with diabetes mellitus, FIV, feline leukaemia virus (FeLV) infection, systemic lupus erythematosus (SLE), Mycoplasma haemofelis infection, hyperadrenocorticism, and systemic or topical inhalant (fluticasone) steroid therapy.13,14 In contrast, Demodex gatoi is a more recently emerging demodex mite that causes an atypical presentation of demodicosis, producing contagious pruritic dermatitis in some exposed healthy cats without concurrent immunosuppression. 13
Demodicosis from D cati often presents with localised regions of well-demarcated alopecia (Figure 4), but generalised disease also occurs. Pruritus is typically mild to absent. The skin disease is usually readily responsive to miticidal therapy, and relatively inconsequential in many cats, with the underlying disease raising more concern. 13

Well-demarcated asymmetrical region of alopecia beside the nasal planum due to demodicosis (Demodex cati). The small area of erosion dorsally was produced during skin scraping
Paraneoplastic presentations
Exfoliative dermatosis associated with thymoma
Generalised scaling and patchy alopecia, with or without erythema, is reported rarely in cats with thymoma. Scaling is typically prominent, often in large white flakes. Skin changes may precede systemic signs of lethargy, anorexia and weight loss. 15 Pruritus is usually absent, although mild pruritus associated with concurrent Malassezia dermatitis is reported. Histopathology from skin biopsies may provide supportive evidence (interface dermatitis); however, similar clinical and histological findings are reported to be unassociated with thymoma. 16
Resolution of skin lesions has occurred with successful surgical excision of tumours, and in the absence of radiographic evidence of thymoma is reported with glucocorticoid and/or ciclosporin therapy (multiple cases) or spontaneously (one cat). 16
Paraneoplastic alopecia
Feline paraneoplastic alopecia is recognised as a unique cutaneous presentation, typically affecting older cats (>10 years). Cats present with prominent alopecia and characteristic smooth shiny skin (Figure 5). Less readily groomed alopecic regions may have adherent brown scale. The alopecia is typically rapidly progressive over a few weeks, with loss of large clumps of hair, starting from the ventrum and progressing to the legs and face (Figure 6). The dorsum is normally spared, but hair may be dull and thinning.

Extensive smooth, shiny, complete alopecia on the ventral body, limbs and head of a cat with paraneoplastic alopecia

Paraneoplastic alopecia in a cat. (a) Poorly demarcated region of alopecia involving the rostral face and periocular areas, with focal thinner shiny skin on the nasal planum and erosions on the rostral lips. (b) Partial to complete alopecia and focal characteristic shiny skin on the front feet
This presentation is most frequently associated with pancreatic carcinoma, but has also been reported with hepatic neoplasias (bile duct carcinoma, hepatocellular carcinoma, hepatosplenic plasma cell tumour) and, in one case, with metastasising intestinal carcinoma.17,18 The majority of cats have metastatic disease, often involving the liver. The pathogenesis of the skin changes is unknown. The prognosis is guarded; many cats die or are euthanased within 8 weeks of developing alopecia.17,18
Characteristic changes (follicular atrophy with miniaturisation of hair bulbs, compact orthokeratotic and parakeratotic hyperkeratosis) are frequently present on histopathology from skin biopsies; 18 however, evaluation of systemic disease is often more prudent.
Other paraneoplastic presentations
Over 30 non-cancerous dermatoses associated with internal malignancy are recognised in humans, and presentations not classical for currently described veterinary syndromes occur sporadically in cats (and dogs). Alopecia in various forms is a common change, although a variety of lesions may occur, and pruritus may be present or absent. Unexplained or atypical alopecia and/or dermatitis, especially in an older or systemically unwell cat, could be a manifestation of internal neoplasia. 19
Leishmaniosis
Leishmaniosis occurs commonly in humans and dogs in endemic regions of the world. Although feline infections are less common, they are increasingly recognised, and cats may play an important epidemiological role. Skin changes include papules, nodules, ulceration and crusting, but more subtle erythema, alopecia and scaling presentations also occur. The head appears to be the most affected region.
Diagnosis and treatment is often complex, and although successful management of feline cases is reported, prevention strategies are favoured in endemic regions.20,21 (See accompanying article on cutaneous manifestations of infectious disease for further discussion.)
Systemic lupus erythematosus
Scant case reports and anecdotal descriptions of feline SLE recount variable, typically subtle skin lesions, including scaling, alopecia, erosions and crusting. As with SLE in other species, cats may present with malaise, pyrexia, reduced appetite and variable signs of associated systemic (renal, neuromuscular, haematopoietic and/or ocular) disease. Skin histopathology may provide supportive evidence of interface dermatitis, and diagnosis is reliant on sufficient consistent evidence of multi-organ disease. 22
FeLV-associated giant cell dermatitis
A very rare scaling, alopecic and crusting dermatitis, with some pruritus, is reported associated with FeLV infection. The head is generally affected (pinnae, preauricular, perioral), along with variable involvement of feet, footpads and other mucocutaneous areas. Histopathology changes in skin biopsies reveal characteristic ballooning of epidermal and follicular epithelial cells (giant cells). 23 FeLV infection in a cat with unexplained, poorly responsive or atypical pruritic dermatitis may raise suspicion for this differential. (See accompanying article on cutaneous manifestations of infectious disease for further discussion.)

Cutaneous horns
Cutaneous horns – conical or cylindrical collections of keratin – are rare, and most often reported on the footpads, although they occasionally arise on the nasal planum or eyelids. They may be associated with FeLV infection (multiple horns), or may constitute localised cutaneous disease only (single or multiple, due to papillomavirus, actinic keratosis, squamous cell carcinoma [SCC] in situ, SCC, keratinising acanthoma). Screening for FeLV status is warranted in cats presenting with cutaneous horns. 25
Hepatocutaneous syndrome (necrolytic migratory erythema, metabolic epidermal necrosis)
A cutaneous presentation of liver or pancreatic disease occurs sporadically in dogs, and one case has been reported in a cat. 26 This cat presented with painful crusting and excessive scaling of footpads, characteristic of the syndrome in the dog. There were concurrent signs of systemic illness (weakness, anorexia, vomiting). A glucagon-producing hepatic carcinoma was detected. 26
Drug reactions
A wide range of cutaneous drug reactions are sporadically reported in cats, including urticaria/angioedema, erythema with or without scaling, maculopapular lesions, nodules, skin atrophy and self-trauma lesions from pruritus. Many different drugs have been implicated, including antibiotics (B-lactams, sulphonamides), antifungals (griseofulvin), topical medications (skin and ear) and prophylactic vaccines. 27 Systemic signs including malaise, pyrexia and anorexia may be evident. Recent drug administration is a valuable part of clinical history summation for any patient presenting with skin disease, particularly when the presentation is not typical for recognised diseases. Definitive diagnosis of a drug reaction requires withdrawal and provocation testing, which is problematic for severe presentations.
The cat with pruritus
Feline skin disease with prominent pruritus is common, and most typically associated with hypersensitivities (Figure 7) or a subset of infectious dermatoses (eg, bacterial pyoderma, Malassezia dermatitis, D gatoi demodicosis, herpesvirus-associated facial dermatitis). Systemic diseases do not tend to present with prominent pruritus, especially in the absence of obvious areas of dermatitis. Secondary bacterial and/or Malassezia species infections may cause obvious pruritus; however, when associated with underlying systemic disease such pruritus is rarely severe, and more typically manifests as subtle licking, limb shaking, rubbing or excessive grooming.
Pruritic cat with atopic dermatitis and concurrent flea bite hypersensitivity. Pruritus was evident during the consultation. Note the healthy sheen to the coat on the trunk and limbs, and patchy partial alopecia on the head

The cat with skin erosions and ulceration
Aside from eosinophilic plaques with their characteristic clinical appearance, prominent skin erosions and ulceration that are not readily explained by self-trauma from pruritus are relatively rare in the cat. Firm adherent crusts may overlie these epidermal defects; however, cat grooming behaviour will often restrict crust formation. This cutaneous presentation is often less diagnostically challenging, as skin biopsies for histopathology are conclusive for many causes.
There are often systemic disease considerations (Figure 8). Some diseases already discussed, including bacterial pyoderma and leishmaniosis, may at times present with prominent erosion through to ulceration (see earlier discussion of ‘the cat with alopecia, erythema, scaling and/or focal crusting’).10,20,22

Multifocal erosions and ulceration on the clipped ventral abdomen of a cat presenting with concurrent malaise. Superficial cytology and screening haemtology, biochemistry and urinalysis revealed no explanatory abnormal findings. Skin biopsies were declined. Erythema multiforme, paraneoplastic pemphigus, drug reactions (no recent history), cutaneous vasculitis and systemic lupus erythematosus were all considerations
Skin fragility
Skin fragility is a syndrome reported in cats with multiple potential causes. It results in skin tearing associated with even minor skin trauma, producing large regions of skin avulsion/ulceration.
Hypercortisolism
Spontaneous hyperadrenocorticism is rare in cats, affecting middle-aged to older individuals, and associated with pituitary (most commonly) or adrenal neoplasia. Cats are more clinically tolerant of high cortisol levels than dogs, so most common systemic signs of canine disease (polyuria, polyphagia, weight loss) are variable, and often absent unless there is concurrent diabetes mellitus.30,31 Iatrogenic hypercortisolaemia in the cat has been associated with injectable, oral and topical glucocorticoids.
Skin changes are reported in approximately 50% of spontaneously occurring cases, and most iatrogenic cases, and include variable alopecia, and thin, fragile and easily bruised skin. Characteristic curling and alopecia of the ear pinnae may also occur, particularly in iatrogenic disease.5,30
Other skin fragility presentations
Similar skin fragility has been reported in single cats with multicentric follicular lymphoma, 32 disseminated histoplasmosis 33 and hepatic lipidosis, 34 although the pathogenesis in those conditions has not been determined. Cutaneous asthenia (Figure 9) is a differential reported in the Burmese cat, and sporadically in other cats. In contrast to other presentations of acquired skin fragility, it should be apparent from a young age. 35

Himalayan cat with cutaneous asthenia – a congenital cause of feline skin fragility. (a) Irregular scarred and focally ulcerated lesions. (b) The cat pictured at a different presentation, showing large areas of ulceration produced by minimal skin trauma, as is typical with skin fragility syndrome
Papillomavirus infection and SCC in situ in Devon Rex cats
SCC in situ lesions are well recognised in middle-aged to older cats of varying breeds as localised single or multifocal melanotic scaly plaques, progressing to ulcerative and crusted plaques and nodules. 25 At least some forms are associated with papillomavirus infection; however, underlying systemic illness is atypical. An aggressive severe form of SCC in situ is reported in Devon Rex cats (Figure 10), which presents with progressive lesions that develop from a young age; this condition has been associated with internal metastasis of papillomavirus-associated SCC.36,37

Squamous cell carcinoma in situ, associated with papillomavirus infection, in a 10-year-old Devon Rex. (a) Persistent multifocal areas of adherent crusting, with mild focal erythema, on the neck. (b) Well-demarcated erosive and crusting lesions on the medial forelimbs
Paraneoplastic pemphigus
A severely erosive and ulcerative dermatosis consistent with paraneoplastic pemphigus is reported in one cat, occurring 3.5 weeks after surgical removal of thymoma. 38 Extensive lesions were present on the ventral abdomen, inner thighs and ear pinnae. Myasthenia gravis, which has been recognised in humans, dogs and cats with thymomas, preceded the skin signs. The myasthenia gravis and skin lesions resolved after several months, and it was presumed that both were paraneoplastic diseases due to autoantibodies released prior to excision of the thymoma. 38
Erythema multiforme complex and toxic epidermal necrosis
Erythema multiforme (EM) is characterised by multifocal keratinocyte death (apoptosis), resulting in multifocal to coalescing areas of erythema to ulceration of the skin and mucosa. There is a spectrum of severity, from mild erythematous lesions to full thickness ulceration, affecting localised to extensive skin and mucosal areas. Classical ‘target’ lesions, consisting of erythematous macules that spread peripherally and clear centrally, may be present. Concurrent malaise and pyrexia are common. Subclassification as EM minor or EM major is based on the severity and distribution of lesions, and the presence or absence of signs of systemic illness. Disease in cats (and dogs) may vary to that in humans, where EM is most often associated with herpesviral infections, and to a lesser extent with drug reactions. Occasional infectious associations are reported in dogs (bacteria, Pneumocystis species, parvovirus, herpesvirus), although many cases are idiopathic. More severe disease in dogs, and most cases of EM reported in cats, have been drug associated.27,39,40
Toxic epidermal necrosis (TEN) is considered a separate disease that is reported rarely in cats, and appears similar to human TEN. It is characterised by keratinocyte apoptosis affecting the full thickness epidermis/epithelium of skin and mucosae, and resulting in widespread areas of skin and mucosal necrosis. TEN is most often caused by drug reactions, and is a life-threatening disease. 27
Diagnosis of EM and TEN is confirmed by histopathological changes on skin biopsies, in association with consistent clinical signs. Diagnosis should prompt a thorough investigation for potential drug triggers and/or underlying infectious diseases. Removal of disease triggers may lead to disease resolution, and is important prognostically.26,39

The cat with nodules and/or nodular swelling
Deeper skin diseases that produce nodules and nodular swelling generally fall into three main aetiological groups: infectious, inflammatory or neoplastic. Some lesional types and distributions may be more suggestive of certain diagnoses, but many nodular skin diseases appear similar. Optimal treatments, likelihood of systemic involvement and prognosis vary widely, and thus prompt confirmation of diagnosis is important.
Infectious disease
A broad range of infectious agents may produce nodular lesions. Some infectious causes, including staphylococcal bacteria (eg, deep pyoderma of the chin), remain localised. A number of primarily opportunistic pathogens also cause nodular skin disease in the cat, typically when traumatically implanted. Some have important systemic disease associations.
Mycobacteria
The most common feline mycobacterial infections present with slowly progressive, poorly demarcated, irregularly nodular lesions with punctate draining tracts, most typically in the caudal abdominal and inguinal areas. The infectious agents are saprophytic mycobacteria (eg, Mycobacterium fortuitum, Mycobacterium chelonae, Mycobacterium smegmatis) that are widely distributed in the environment, and grow readily in the laboratory. These mycobacteria most often cause localised cutaneous disease in immunocompetent hosts, but occasional dissemination occurs in immunocompromised patients.41,42 More rarely, mycobacteria restricted to certain geographic regions cause more discrete skin nodules, often with dissemination to other body organs.
Widespread dissemination in immunocompromised cats is typical with the classical ‘tuberculous’ mycobacteria (eg, Mycobacterium bovis, Mycobacterium tuberculosis, Mycobacterium microti). These are obligate animal pathogens associated with severe zoonotic potential and, in the case of some environmental species, with more selective pathogenicity (eg, Mycobacterium avium complex in familial young Abyssinian and Somali cats, Mycobacterium genavense in old cats with longstanding FIV, and Mycobacterium visibile). Most cats with these mycobacterial infections have signs of systemic illness (respiratory, gastrointestinal) and lymphadenopathy in addition to typically discrete skin nodules, which may or may not ulcerate. 41
Feline leprosy is caused by fastidious mycobacteria that will not routinely grow on laboratory media (eg, Mycobacterium lepraemurium, M visibile). Infections are rare and most typical in healthy cats with outdoor exposure (often hunters). The reservoir of these mycobacteria is currently unknown; however, infection appears to be associated with rodent bites (M lepraemurium), or traumatic implantation (Candidatus ‘Mycobacterium tarwinense’, M visibile, Candidatus ’Mycobacterium lepraefelis’). Infected cats may present with localised nodules (Candidatus ‘M tarwinense’, M lepraemurium), or widespread nodules (Candidatus ‘M lepraefelis’, M visibile) that occasionally progress to systemic disease.41-45 (See accompanying article on cutaneous manifestations of infectious disease for further discussion.)
Nocardia species
Nocardia species are ubiquitous environmental bacterial saprophytes that very occasionally cause infection in immunocompromised cats, following implantation via skin wounds or inhalation. Progressive irregular nodules and punctate draining sinuses are typical, often with lung infection or widespread dissemination. Infections may start with discrete abscesses that gradually extend. The extremities, ventral abdomen and inguinal areas are typically affected, and lymphadenopathy is common. 46
Environmental fungi
There are multiple environmental fungi that will occasionally cause infections when skin penetration occurs. Although many infections remain localised, some fungal species with varying global distributions cause sporadic but serious disseminated infections in cats that may present as prominent nodular skin lesions. These more pathogenic fungal species include Cryptococcus species and Sporothrix species, found in their preferred environmental niches worldwide, and Blastomyces species, Histoplasma species and Coccidioides species that occur in very restricted geographical locations. Systemic involvement with these infections is common, with the respiratory tract, eyes and central nervous system most frequently affected. Skin nodules tend to occur on extremities (face, pinnae and feet).47-49
Protozoa
Leishmaniosis in cats can present with nodules that may ulcerate, with or without other skin lesions that include alopecia, scaling, papules, erosions and ulceration. Many infections are disseminated. 18 Toxoplasmosis in cats is very rare, usually associated with immunocompromise, and most frequently presents with systemic signs (malaise and fever, with or without respiratory, gastrointestinal, neurological or ocular signs). Skin nodules occur rarely, are typically multiple and may ulcerate. 50
Inflammatory disease
Some nodular lesions in cats are inflammatory in origin, including eosinophilic granulomas and plaques, which are very frequently associated with underlying hypersensitivity. Rare sterile inflammatory lesions may be associated with systemic disease.
Sterile panniculitis
Panniculitis is reported very occasionally in cats, associated with dietary imbalance (vitamin E deficiency with, for example, exclusively fish diets) and as a sterile idiopathic form, but may also be associated with pancreatitis or pancreatic neoplasia. Lesions in all forms are reported more frequently in the ventral abdominal or ventrolateral thorax regions; they appear as single or multiple irregularly nodular regions, with or without draining tracts, that are clinically indistinguishable from infectious causes of panniculitis including mycobacteria and Nocardia species. 51
Xanthoma
Multiple pale yellow to pink plaques through to intact or ulcerated nodules occur rarely in cats with abnormalities in lipid metabolism, including hereditary hyperlipidaemia and diabetes mellitus. Lesions are most frequent on the head and distal extremities, and may be pruritic. 5 One atypical idiopathic presentation has been described with more diffuse irregularly nodular yellowish regions in a normolipaemic cat. 52 These lesions produce characteristic histopathology, and diagnosis of xanthoma from skin biopsies warrants systemic evaluation (Figure 11). 5

Multifocal erythemic plaques on the dorsal periocular areas, pinnae and forehead of a 1-year-old domestic shorthair cat with cutaneous xanthomas due to familial hypertriglyceridaemia
Neoplasia
Neoplastic nodular skin lesions mimic infectious and inflammatory nodules. Although skin neoplasia in cats is more frequently malignant than in dogs, many forms are locally aggressive with a low risk of metastasis. Aggressive forms with a higher risk of metastasis include some mast cell tumours (Figure 12), malignant melanoma and histiocytic sarcomas.24,53

Multifocal discrete nodules, some with focal crusting, in a 12-year-old domestic shorthair cat with histiocytic mast cell neoplasia


Nodule with partial alopecia and mild focal crusting on the lateral tibial region of the cat pictured also in Figure 12. Disseminated infectious causes (mycobacteria, fungae, protozoa) were initial considerations in addition to neoplastic causes. The neoplastic mast cells were poorly differentiated and agranular, and not readily detected on routine staining
Key Points
Skin can be an important marker of general health, and skin and haircoat changes can at times be the first indication of significant systemic disease.
Any cat presenting with skin disease should have screening of both the history and physical examination for clues that are less consistent with common skin-restricted dermatoses and that may raise suspicion for systemic disease. These findings, together with the skin presentation, then guide the most appropriate additional diagnostics.
Careful screening for dietary imbalance, risks of contagious infection and signs of systemic disease are important for the cat presenting with a dull, unkempt coat.
Cytology and skin biopsies are often most important for both nodular and erosive to ulcerative presentations to distinguish between infectious, sterile and neoplastic causes, with their variable systemic disease associations.
For the pruritic cat, although cutaneous hypersensitivities are very common, some secondary and primary infections may mimic allergic causes and be associated with underlying systemic illness. Thus, remaining alert for atypical presentations and cognisant of potential links of infection with underlying systemic disease is important.
Possibly the most challenging dermatological presentation to correctly associate with systemic disease is the cat with variable combinations of alopecia, erythema, scaling and focal crusting; where hypersensititives, infections, autoimmune diseases and systemic diseases are all considerations. In this scenario, a broad knowledge of common dermatoses will help with recognition of less consistent historical or lesional clues to raise the profile of systemic diseases, and accurate cytology skills will help exclude common infectious causes. Both are key to more accurate assessment of the potential for underlying systemic disease.
Footnotes
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.