
Abstract
Objectives
Radioiodine (131I) dose determination using radiotracer kinetic studies or scoring systems, and fixed relatively high 131I dose (ie, 4 or 5 mCi) administration, are effective and associated with prolonged survival times for hyperthyroid cats. The latter method is less complicated but could expose patients and veterinary personnel to unnecessary levels of radiation. The aim of this study was to retrospectively evaluate the efficacy of a fixed 3.35 mCi 131I dose for the treatment of 96 hyperthyroid cats with no length estimation for any palpated goitre ⩾20 mm, assess outcome and identify factors associated with survival.
Methods
Serum total thyroxine concentrations at diagnosis and at follow-up times, survival times and cause of death were recorded. Multivariable Cox regression analysis was used to identify factors associated with time to any cause of death from 131I therapy initiation.
Results
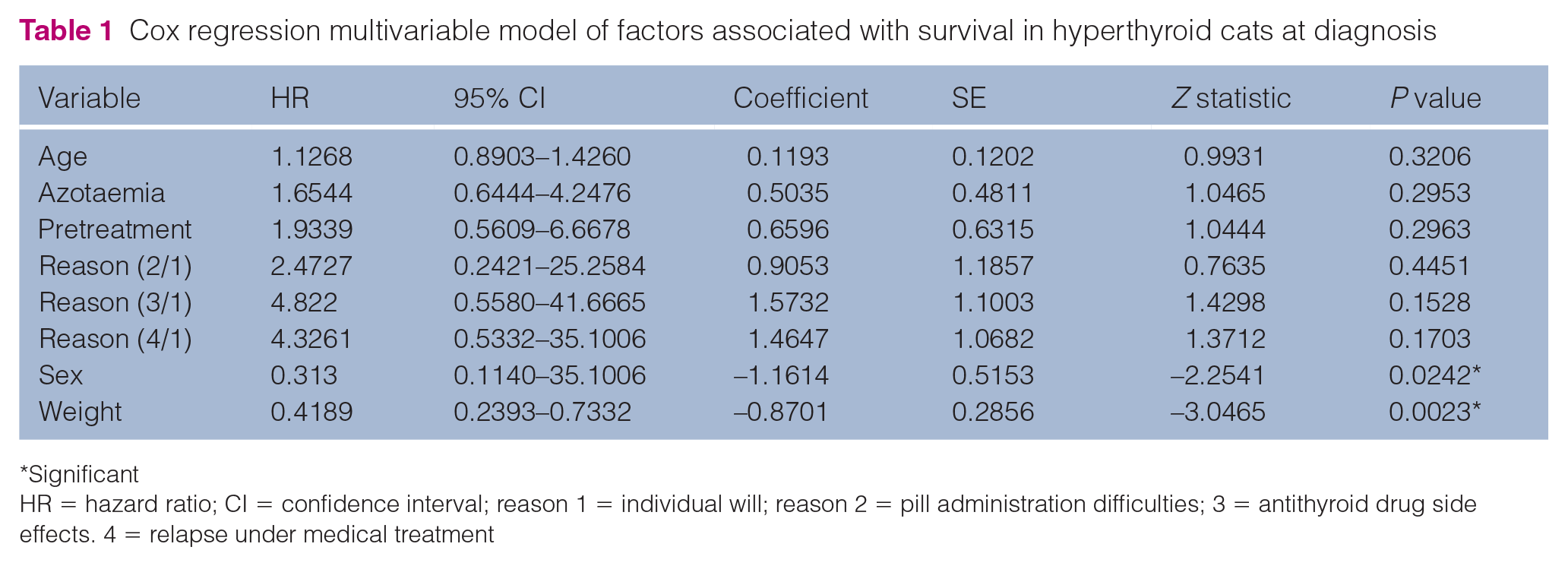
Administration of a median (interquartile range) dose of 3.35 mCi (3.27–3.44 mCi) radioiodine was an effective treatment in 94/96 cats, but two cats remained hyperthyroid. No death related to hyperthyroidism was recorded. Median survival time was 3.0 years; the 1 and 2 year survival rates after 131I therapy were 90% and 78%, respectively. Low body weight (⩽3.1 kg; adjusted hazard ratio [aHR] 5.88; 95% confidence interval [CI] 2.22–16.67; P <0.01) and male gender (aHR 2.63; 95% CI 1.01–7.14; P = 0.04) were independently associated with death, whereas age, prior treatment with antithyroid drugs, reason for treatment and pretreatment azotaemia were not.
Conclusions and relevance
This study suggests that a fixed 3.35 mCi 131I dose treatment is effective for hyperthyroid cats with goitre(s) with a maximal length estimation <20 mm, that long-term survival can be achieved and that low body weight and male gender are significantly associated with shorter survival times.
Introduction
Hyperthyroidism is the most common endocrine disorder in geriatric cats. 1 Several treatment modalities are used for this disease, including radioiodine (131I). Both individual 131I dose determination using radiotracer kinetic studies or scoring systems, and fixed relatively high 131I dose (ie, 4 or 5 mCi) administration have been used.2–11 The latter method is less complicated but could expose veterinary staff and patients to unnecessary levels of radiation, resulting in an increased risk of hypothyroidism. 12 Decreasing the 131I dose would decrease exposure to radiation but raises concerns about a possible impact on efficacy. Only a few reports have documented survival times for hyperthyroid cats treated with radioiodine.7,13,14 None evaluated survival times for cats treated with a fixed 3.35 mCi 131I dose administration.
The aim of this study was to retrospectively evaluate the efficacy of a fixed 3.35 mCi 131I dose for treatment of hyperthyroid cats, to assess outcome and identify factors associated with survival.
Materials and methods
Criteria for selection of cases
Medical records of hyperthyroid cats treated with 131I in a single referral centre between June 2006 and June 2010 were examined. Included were all cats with: (1) a history and a physical examination consistent with hyperthyroidism; (2) no length estimation of any palpated goitre ⩾20 mm (each cat had careful palpation of the neck and thorax inlet for maximal length estimation of each detected goitre – cats with no palpable goitre and cats with one or multiple goitres, each with an estimated length <20 mm were included); (3) a serum concentration of total thyroxine (TT4) above the reference interval (RI); (4) a fixed intravenous 131I dose (3.35 mCi ± 0.1). Exclusion criteria were lack of available data concerning pretreatment or follow-up TT4 concentration, health status at follow-up or before death or pretreatment histopathological analysis compatible with thyroid carcinoma.
Procedures
Signalment, weight, clinical signs and serum TT4 concentrations at diagnosis, prior treatment with antithyroid drugs and reasons for 131I, were recorded for every cat. Urea and creatinine concentrations, alanine aminotransferase (ALT) and alkaline phosphatase (ALP) activities at diagnosis were also recorded when available. All cats underwent a physical examination, including weight measurement and estimation of each palpated goitre length by the same clinician (PF-T).
All cats were treated with a fixed 131I dose (3.35 mCi ± 0.1). The dose within the syringe was controlled using a calibrator and administered as a bolus via a 22 G intravenous catheter, using an injection cap. After 131I dose was administered, the cats were kept in individual stainless steel cages in a designed radiation isolation ward according to the institution’s radiation safety regulations (Autorité de Sécurité Nucléaire). Cats were discharged from the hospital after 13 days.
Serum TT4 concentrations were then collected at a follow-up time occurring between 1 and 3 months after treatment, conducted either at the same centre or at the referring veterinarian facility with instructions to forward serum TT4 concentration, as well as clinical and other clinicopathological data. As several laboratories using different analytical methods and RIs for serum T4 concentration determination were involved, serum TT4 concentration measurements were expressed as the ratio between the actual value and the upper reference limit for each laboratory as previously described. 15
Euthyroidism was concluded in cats with serum TT4 concentration ratio <1 and no hypothyroidism (see below). In case of serum TT4 concentration ⩾1, another reassessment was performed 1 month later. Persistent hyperthyroidism was concluded if clinical signs of hyperthyroidism were still present and the serum TT4 concentration ratio was ⩾1. Hypothyroidism was concluded if clinical signs of hypothyroidism were developed along with serum TT4 concentration lower than the RI.
Long-term follow-up was performed once annually thereafter. Serum TT4 concentration was determined at each follow-up visit. Hyperthyroidism relapse was concluded in case of clinical signs of hyperthyroidism recurrence and serum TT4 concentration ratio ⩾1 after a remission period.
Statistical analysis
Statistical analyses were performed with Epi Info version 3.5.4. Results are reported as median (25th and 75th percentiles) and statistical significance was defined as P ⩽0.05.
Differences between means of continuous variables at diagnosis, initial and last follow-up times were tested using the paired t-test. χ 2 or Fisher tests was used to compare percentages for binary variables. For the survival analysis, the study outcome was death, whatever the cause. If data regarding death were not available, the referring veterinarian or the owner was contacted by telephone to request follow-up information. Time to event was time from the date of 131I initiation to either the outcome or the censoring. Cats were censored if they were still alive at the end of the follow-up period (15 March 2012). Median survival time was determined by the Kaplan–Meier product-limit method. Kaplan–Meier survival curves were plotted and survival times for cats in each group were compared by the log-rank test. A multivariate Cox model was used to investigate independent risk factors for death. The following variables were entered into the Cox model to determine if they were independently associated with survival: sex and age, weight, azotaemic status at diagnosis, prior treatment with antithyroid drugs, reason for treatment and azotaemic status after 131I.
Results
Study population
During the study period (June 2006–June 2010), 164 cats were treated. Sixty-six cats were excluded from the study owing to incomplete medical records (n = 57) or lost to follow-up (n = 5); two cats with thyroid carcinoma and four cats with goitre length ⩾20 mm were also excluded from the study. The study sample included the remaining 96 cats.
Median age of the study population at treatment was 13 years (interquartile range [IQR] 11–14 years; range 5–18 years). Forty of the 96 cats were male and 56 were female. Eighty-four of the 96 cats had a prior treatment with antithyroid drugs. Owners elected for 131I treatment either for the purpose of a definitive treatment (n = 47), considering their cat’s compliance (n = 19), owing to antithyroid drug side effects (n = 19) or secondary to a relapse of the disease despite medical management (n = 10).
Serum TT4 concentration and serum biochemical testing
At diagnosis, serum TT4 concentration ratios were above the RI in 96/96 (median 1.82; IQR 1.41–2.45; range 1.02–5.52) (Figure 1); ALT and ALP activities were above the RI in 52/65 cats and 29/56 cats, respectively. None of the cats had serum creatinine concentrations above the RI at diagnosis. Azotaemia due to urea concentration above the RI was recorded for 17/96 cats.

Box plot of serum total thyroxine (TT4) concentration ratio in study cats at diagnosis, and at initial and last follow-up times. The box represents the population between the first and the third quartiles with the median represented as the horizontal bar through the box, and the whiskers represent the data between the box ± 1.5 times the interquartile range. The maximal outliers are marked with asterisk
For the 84 cats treated medically with methimazole before 131I treatment, duration between diagnosis of hyperthyroidism and 131I treatment was 86 days (IQR 52–253; range 23–1096). Methimazole administration was stopped 4 days (IQR 4–11; range 3–11) before 131I treatment. For the 12 cats treated with 131I without previous medical treatment, duration between diagnosis of hyperthyroidism and 131I treatment was 21 days (IQR 17–29; range 6–81).
Median administered 131I dose was 3.35 mCi (IQR 3.27–3.44). Median initial and last follow-up times were 71 days (IQR 57–80) and 356 days (IQR 200–614), respectively. Median serum TT4 concentration ratios at first and last follow-up times were 0.44 (IQR 0.29–0.71; range 0.03–4.17), 0.34 (IQR 0.26–0.54; range 0.09–1.5), respectively (Figure 1). Median serum TT4 concentration ratios at first and last follow-up times were significantly lower than the median value at diagnosis (P ⩽0.05). Only two cats developed clinical signs of hypothyroidism (lethargy, obesity and dermatological signs) diagnosed at 50 and 75 days after 131I treatment, respectively. Their TT4 values at diagnosis were 167 nmol/l and 81 nmol/l, respectively. Both received oral supplementation with L-thyroxine. Last follow-up information was available 9 and 15 months after treatment, respectively. The first cat was well substituted with no clinical signs but had an IRIS stage 2 chronic kidney disease; the second cat was not well controlled owing to the cat’s compliance and was still lethargic at last follow-up with creatinine concentration above the RI. Two cats had persistent hyperthyroidism, and two cats relapsed with hyperthyroidism 1.6 years and 3.4 years after 131I treatment, respectively.
ALT activity at initial and last follow-up times were above the RI in 2/34 cats and 4/33 cats, respectively. ALP activities at initial and last follow-up times were above the RI in 1/27 cats and 2/27 cats, respectively. Serum creatinine concentration above the RI was identified only in 6/53 cats and 8/47 cats at initial and last follow-up times, respectively.
Survival time
Median survival time for all 96 cats was 3.0 years from 131I therapy initiation (Figure 2). The 1 and 2 year survival rates after 131I therapy were 90% and 78%, respectively.

Kaplan–Meier curve of survival times for 96 cats with hyperthyroidism treated with a fixed a 3.35 mCi radioiodine dose (interquartile range 3.27–3.44)
Male sex and low body weight (⩽3.1 kg) were independently associated with death (Table 1, Figure 3). Age, prior treatment with antithyroid drugs, reason for 131I and pretreatment azotaemia were found in multivariate analysis not to be significantly associated with survival time (Table 1).
Cox regression multivariable model of factors associated with survival in hyperthyroid cats at diagnosis
Significant
HR = hazard ratio; CI = confidence interval; reason 1 = individual will; reason 2 = pill administration difficulties; 3 = antithyroid drug side effects. 4 = relapse under medical treatment

Kaplan–Meier curves of survival times for the same 96 cats grouped according to their body weight at treatment. CI = confidence interval; BW = body weight
Discussion
To our knowledge, this is the first study to evaluate the efficacy of a fixed 3.35 mCi 131I dose (IQR 3.27–3.44 mCi) for treatment of hyperthyroid cats with goitre length estimation <20 mm, assess outcome and identify factors associated with survival. The optimal method to determine the 131I dose for effective hyperthyroidism treatment remains to be decided. In theory, the accurate 131I dose to be administrated, adjusted for every hyperthyroid cat, would be the one to prevent both treatment failure and iatrogenic hypothyroidism. Such a dose could be estimated either through tracer kinetic protocols and thyroid gland size, or calculated according to clinicopathological scoring systems. However, to date, efficacy of these methods has not been demonstrated to be superior to the unchallenging use of a relatively high (4–5 mCi) fixed 131I dose. Thus, the two strategies are nowadays still employed in human and veterinary medicine with a trend to use fixed, relatively high doses.2–8,16–18 In the largest survey evaluating the efficacy of 131I treatment for hyperthyroid cats using a variable clinicopathological score system to determine the dose to be administrated, euthyroidism was achieved in 87% of cats, despite 131I doses <3.40 mCi in 50% cats. 7 Consequently, fixed doses higher than 3.40 mCi may expose both patients and veterinary personnel to unnecessary levels of 131I, at least in some cases. However, damage from radiation exposure following contact with 131I-treated patients has not been shown in caregivers to humans or animals; reducing 131I doses to the lowest effective levels is recognised as a paradigm for this treatment. 19 The present cohort study reveals that a fixed 131I dose of 3.35 mCi is effective, with only 2/96 cats remaining hyperthyroid. These results are similar to previous studies using variables or fixed higher 131I doses.2–11,13,14
Intravenous and subcutaneous routes are commonly recommended for 131I treatment.20,21 The two routes are considered to be efficient, but subcutaneous administration has been shown to be safer for medical staff in two previous studies,22,23 even if the intravenous administration modalities (no injection cap, direct intravenous injection without catheter for some cats) differed from the process used in the current study. Generalising the present results obtained after intravenous injection to subcutaneous routes remains to be determined.
Treatment efficacy was assessed mainly through serum TT4 concentration assessment. TT4 was measured at diagnosis and during follow-up but not just prior to 131I treatment, as a clinicopathological scoring system comprising TT4 concentration for determining the injected 131I dose was not used. Because of the retrospective design of the study, biochemistry data, including TT4, were measured using different assays and this heterogeneity could have hampered the results. At diagnosis and during follow-up, the measurements were compared with their own RR qualitatively (ie, below, within or above the RI) limiting the impact of this heterogeneity. Likewise, for TT4 concentration, the impact of this heterogeneity is limited by good correlation of the results obtained with the assays generally used in the veterinary field. 24 This correlation drove us to report TT4 concentrations as continuous pooled after normalisation by their own upper reference limit, as previously described. 15
Sensitivity of serum TT4 concentrations to diagnose hyperthyroidism is not perfect and treatment failure might have been underestimated. ALT and ALP activities generally normalise after successful treatment of hyperthyroidism. 25 In the present study, ALT and ALP activities both within the RI were recorded in 22/25 cats and 23/27 cats during initial and long-term follow-up times, respectively, supporting treatment efficacy in most of the cases. Nevertheless, most of the cases were followed-up by the referring veterinarians, hampering the accurate reporting of follow-up clinical data, such as standardised body weight measurement, for instance, and this represents a major limit of the study.
Iatrogenic hypothyroidism was documented in 2/96 cats. This result suggests the possibility, at least in these cases, of having used a lower dose of 131I. In a recent study focusing on cats with mild-to-moderate hyperthyroidism, cats treated with even a lower dose of 131I (ie, 2.0 mCi) were significantly less likely to develop long-term hypothyroidism (evaluated at 3 and 6 months after 131I treatment) compared with cats treated with a higher dose of 131I (ie, 4.0 mCi) with no significant difference in persistent hyperthyroidism between the two groups. 11 The relevance of generalising the use of a fixed lower dose to a less selected hyperthyroid cat population has still to be demonstrated.
In a recent large cohort study evaluating thyroid scintigraphy examination, huge goitres (defined as spheres with length × width² ⩾1.9 cm3) and suspected carcinomas (based on multifocal areas of increased thyroid uptake that extended beyond the margins of the thyroid tumours) were identified in 2.3% and 1.7% of the cases, respectively. 26 The population of the present study was obtained excluding huge goitres (defined as any goitre ⩾20 mm) and confirmed carcinomas representing 3.9% and 1.9% of the cats, respectively. These findings suggest the possibility that the majority of hyperthyroid cats could be treated with a fixed dose of 3.35 mCi 131I.
Iatrogenic hypothyroidism was diagnosed in 2/96 cats in the present study. Only hypothyroid cats with both serum TT4 concentration below the RI and clinical signs consistent with the disease were detected. As TSH concentrations were only occasionally measured via canine thyroid-stimulating hormone (cTSH) assay, during the study period, subclinical hypothyroidism (ie, cats without clinical signs but serum TT4 concentration below RI and cTSH concentration above the RI) may have been missed. In one study, the serum cTSH concentration was above the RI in 10/12 cats at 3–6 months after 131I treatment, but the 131I administrated dose was not documented. 27 In another study, focusing on a large cohort of cats treated with variable 131I doses ranging from 1.7–27.0 mCi, subclinical hypothyroidism was diagnosed in 7% of the cats with overt hypothyroidism only documented in 3% of the cases. 28 Subclinical hypothyroidism can be self-limiting (decreasing serum cTSH concentration to RI without any medication) 28 and the impact of having possibly missed subclinical hypothyroid cats in the present study is not clear.
The median survival time for cats in this study was 3 years. In none of the cases was an association between death and hyperthyroidism or its treatment suspected. However, this assessment is speculative in geriatric and often multi-morbid cats and the lack of an age-matched control population precludes any definitive conclusion. Moreover, most of the cats died at home or at the referring veterinarian facility and information regarding the cause of death was missing in few cases. Median survival time for cats treated with 131I was estimated in few previous surveys and ranged from 1 to 3 years.6,7,13
None of the cats enrolled in the present study had a creatinine concentration above the RI at diagnosis. During the follow-up period, 17% of cats had creatinine concentrations above the RI. As most of the follow-ups were carried out by referring veterinarians, information concerning urine specific gravity was often lacking and we may have missed, both before and after treatment, IRIS stage 2 chronic kidney disease. Previous studies reported similar results (incidence ranged from 7–30%).10,29–33 In one study, no difference was identified between the survival of cats reaching euthyroidism with azotaemia in parallel, and those reaching euthyroidism without azotaemia. However, a shorter survival time was identified in cats developing both hypothyroidism and azotaemia after treatment. 27 The creatinine concentrations of the two hypothyroid cats of the present study were equal to 23 mg/l (RI 6–15 mg/l) and 26 mg/l (RR 8–24 mg/l) at hypothyroidism onset, respectively. Both cats were alive at the end of the study 9 and 15 months, respectively, after treatment.
The present study found that male cats treated with a fixed, low 131I dose had shorter survival times than female. Similar results were previously reported. 13 The reason for this association remains unexplained. Results in the present study also suggest that cats with a body weight ⩽3.1 kg before 131I therapy had shorter survival times than cats with a body weight >3.1 kg. Although objective and accurate, body weight only partially reflects body condition and, more importantly, muscle condition changes in hyperthyroid cats. 34 No record of muscle condition score was made for cats included in the present study precluding the use of the variable in the Cox model. A single veterinarian examined all cats in the study and low body weight was not identified as correlated to comorbidity. Despite this, concurrent occult disease could not be excluded, and residual confounding factors may persist.
Azotaemia prior to treatment was not significantly associated with death in the present survey, similar to a previous study. 35 Azotaemic cats at diagnosis had urea concentrations above the RI but creatinine concentrations within the RI. For most of these cases, repeated renal parameters measurements or urine specific gravity were missing. Therefore, these findings could suggest either pre-renal or renal azotaemia. Referring vets might have recommended 131I treatment less often for azotaemic hyperthyroid cats, considering the potentially shortened life span in this context and such advice may have biased our study population towards patients with no or mild chronic kidney disease.
Conclusions
This study suggests that a fixed 3.35 mCi 131I dose treatment is effective for hyperthyroid cats with goitre(s) of a maximal length estimation of <20 mm and without a definitive diagnosis of thyroid carcinoma. Choosing a fixed 131I dose is less complicated than using radiotracer kinetic studies or scoring systems. In addition, decreasing the 131I dose administration decreases the exposure of patients and veterinary staff to unnecessary levels of radiation. This study suggests that long-term survival can be achieved with this method and that body weight ⩽3.1 kg and male sex are associated with shorter survival times. Comparative data between efficacy of fixed 3.35 mCi 131I doses and variable low ones are still warranted.
Footnotes
Author note
Part of this work was presented at the 23rd ECVIM-CA Congress in Liverpool (UK) in September 2013.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.