
Abstract
Objectives
The outcome of radioiodine therapy in hyperthyroid cats is suspected to be influenced by multiple factors. The degree of activity of the thyroid gland, represented by uptake of sodium pertechnetate or tracer activities of radioiodine by the thyroid gland on thyroid scintigraphy, has been suggested in the literature as one of those. Thyroid gland pertechnetate uptake can be represented by (semi-)quantitative factors such as the thyroid to salivary gland (T/S) ratio, the thyroid to background (T/B) ratio and the percentage technetium uptake by the thyroid glands (%TcU). The aim of this study was to investigate a possible relationship between these thyroid scan parameters and radioiodine therapy outcome.
Methods
Sodium pertechnetate thyroid scans of 75 hyperthyroid cats were retrospectively evaluated and statistical analysis was performed with and without correction for injected radioiodine activity. Three different background regions of interest (ROIs) were used to calculate the T/B ratio and %TcU: ‘neck’, ‘circle’ and ‘copy ROI’.
Results
Higher T/S ratios were found to be significantly related to a persistent hyperthyroid outcome in both analyses. For the T/S ratio, a threshold value of 5.4 was determined, with a sensitivity of 73% and a specificity of 59%. An increased risk for persistent hyperthyroidism compared with a final euthyroid outcome with an increased T/Bcircle ratio was only found to be significant without correction for the activity of radioiodine administered. For the %TcU no statistical significance was reached. Regarding a low total thyroxine outcome, no significant relationships with any of the investigated parameters were found.
Conclusions and relevance
The findings of this study suggest that semi-quantification of thyroid gland uptake is best performed using the T/S ratio. A T/S ratio ⩾5.4 is a possible indicator for an increased risk of persistent hyperthyroidism.
Introduction
Hyperthyroidism is a common disease in older cats and radioiodine therapy is an important treatment option.1–4 Research to further optimise the treatment protocol or to detect factors that may affect or predict therapy is difficult, as the therapy shows a generally good outcome of 70–95%. The definition of a successful therapy and follow-up times vary throughout the literature.5–12 However, negative effects associated with a hypothyroid or persistent hyperthyroid outcome, such as daily thyroxine (T4) supplement pilling, possibly decreased renal function or the need for repeated radioiodine treatment, justifies the search for these factors that may predict or influence radioiodine therapy outcome.13,14
In previous work from our department the effect of thyroid volume on radioiodine therapy outcome was investigated. Only an increased risk towards a low total T4 (TT4) outcome was seen with the presence of multiple affected thyroid foci. 15 Aside from thyroid volume or the number of affected foci, thyroid uptake has also been suggested as a factor predicting or influencing radioiodine therapy outcome. Thyroid gland uptake can be estimated by semi-quantitative ratios: the thyroid to salivary gland (T/S) ratio and the thyroid to background (T/B) ratio or by a quantitative measurement – the percentage technetium uptake (%TcU). Pertechnetate (TcO−4) and radioiodine are taken up by the thyroid glands by the same receptors and pertechnetate can therefore be used in the diagnosis of hyperthyroidism and (semi-)quantification of uptake before therapy. 16 Human literature shows conflicting results regarding the predictive effect of radioiodine or pertechnetate uptake in patients with Graves’ hyperthyroidism, although the majority of the authors report an increased number of patients with persistent hyperthyroidism with increased uptake of pertechnetate or radioiodine by the thyroid gland.17–21 In cats, only two studies have been published. Whereas the T/S ratio in cats did not appear to be related to therapy outcome, a relationship was found between increased T/B ratios and persistent hyperthyroidism.10,12 Regarding the predictive value of %TcU, no studies are currently available, to our knowledge.The aim of this study was to investigate a relationship between pre-therapy sodium pertechnetate uptake parameters by the thyroid gland and the final outcome of the radioiodine therapy. The hypothesis was that higher uptake of sodium pertechnetate would result in an increased risk for persistent hyperthyroidism, whereas patients with a less prominently increased uptake would show an increased chance of a euthyroid or low TT4 outcome.
Materials and methods
Demographics
The study included 75 hyperthyroid cats. These cats were diagnosed with hyperthyroidism by the referring veterinarian based on a combination of thyroid palpation, clinical signs and TT4 concentration, and referred to our clinic for radioiodine therapy. Inclusion criteria for the current study were that one or more well-delineated hyperactive foci were seen on the pre-therapy pertechnetate scans and that a control serum TT4 measurement at 6 months post-therapy was available. These control TT4 measurements were performed at a laboratory chosen by the referring veterinarian where the 6 month control examinations were performed. The cats also underwent a thorough physical examination at 6 months post-therapy to exclude occurrence of new disease that could influence the TT4 measurement. None of the cats included received drugs other than antithyroid medication prior to or after the radioiodine treatment.
Diagnostic pertechnetate imaging
The cats were injected intravenously via a catheter with a median activity of 92.5 MBq (range 51.8–148 MBq) pertechnetate into the cephalic vein. Acquisitions were performed 30 mins after the injection on a dualhead gamma camera, with a low-energy, high-resolution collimator positioned underneath the scan bed (GCA 7200A; Toshiba). The patients were anaesthetised with propofol (4–8 mg/kg to effect, IV, Propovet 10 mg/ml [Ecuphar]) and positioned in ventral recumbency with the front limbs pulled forward. A standard, that is, a syringe containing a known, small amount of radioactivity, was placed next to the cat and scanned simultaneously. Zoomed 25.6 × 25.6 cm field-of-view planar images were acquired on counts (200 kcounts), in a 256 × 256 matrix.
Different regions of interest (ROIs) were placed on the images to calculate the following parameters: T/S ratio, T/B ratio and %TcU. ROIs were drawn manually over the hyperactive thyroid lobe focus(foci) and salivary gland(s). Three different background ROIs were placed on the scan: two rectangular, fixed-size ROIs were placed cranial and caudal to the thyroid lobe(s) and averaged (background ‘neck’) (1); a fixed-size circular ROI was placed in the ipsilateral axillary region of the patient (background ‘circle’) (2); and, finally, a copy of the thyroid lobe ROI was placed in the ipsilateral axillary region (background ‘copy ROI’) (3). To calculate the percentage pertechnetate uptake another ROI was drawn manually over the standard activity and a copy of this ROI was placed on the scan as far away from the patient and the standard as possible to correct for background activity. The three described background ROIs were used both for the T/B ratio and the %TcU; however, background correction was only performed for the %TcU. The T/S and T/B ratios were calculated using the mean number of counts per pixel. Drawing of the ROIs and calculations were performed by three observers (VV, EV, KP) using multimodality software (Hermes V5.0; Nuclear Diagnostics AB).
Radioactive iodine (131I) therapy
Following the pertechnetate scans the cats received an intravenous injection of radioiodine (131I). The amount of radioactive iodine administered depended on the severity and duration of clinical signs, the TT4 and the T/S ratio, similar to a previously reported dose-scoring method. 8 In order to correct for this injected amount of radioiodine in the statistical analysis, the cats were divided into three dose categories: (1) 74–148 MBq (n = 49); (2) >148–259 MBq (n = 19); and (3) > 259 MBq (n = 7). All patients were taken off antithyroid medication before the radioiodine therapy for a minimum of 10 days.
Therapy outcome and influencing factors
Follow-up clinical examinations and blood work were performed by the referring veterinarian. To correlate the calculated factors to radioiodine therapy outcome, the cats were divided into three groups according to the 6 month blood result: low TT4, euthyroid or hyperthyroid. The cats were categorised as low TT4 and not hypothyroid as these final outcomes were solely based on a single serum TT4 measurement and a diagnosis of true hypothyroidism could not be guaranteed.15,22 In patients with two or more hyperactive thyroid foci, only the values of the most active focus was used in the statistical analysis.
The statistical analysis was based on logistic regression. In separate analyses, the effect of different imaging parameters on the odds of a low TT4 vs a euthyroid outcome, persistent hyperthyroidism vs a euthyroid outcome and persistent hyperthyroidism vs a low TT4 outcome were assessed and summarised by the odds ratio (OR). Furthermore, the different imaging parameters were compared between the thyroid status groups using the F-test in a linear effects model and the groups were compared pairwise using Tukey’s method to adjust for multiple comparisons. An additional logistic regression analysis was performed using dose category as a covariate. To assess the diagnostic accuracy of the T/S ratio in detecting the risk of persistent hyperthyroidism, receiver operating characteristic (ROC) curve analysis was performed. Tests were performed at the 5% significance level.
Results
Of the 75 hyperthyroid cats included, 36 were male and 39 were female. All patients were neutered and the median age was 12 years (range 6–18 years). Thirty-nine (52%) cats were euthyroid at 6 months after the radioiodine therapy. Eleven cats (15%) showed persistent hyperthyroidism and 25 (33%) showed a TT4 below the reference interval (low TT4).
The scans were subdivided into three different uptake patterns: 24 cats had a single hyperactive focus (unilateral disease), 46 cats showed the presence of two hyperactive foci (bilateral disease or unilateral disease with ectopic thyroid tissue) and five cats showed the presence of more than two hyperactive foci. Although imaging features cannot distinguish benign from malignant disease with certainty, none of the thyroid scans suggested the presence of malignant disease, with features such as heterogeneous radionuclide uptake, irregular thyroid lobe margins and very extensive, possibly multifocal, radionuclide uptake outside the normal thyroid lobe contours. 16 There was also no evidence of pulmonary metastases in any of the cats. The parameters included in the analysis for the complete group of hyperthyroid cats and per therapy outcome group are summarised in Table 1.
Number of hyperactive foci and (semi-)quantitative scintigraphic parameter values for all patients included in the study and for each outcome category

Data are median (range)
T/S = thyroid to salivary gland ratio; T/Bneck = thyroid to background ratio using background neck; T/BcopyROI = thyroid to background ratio using background copy region of interest; T/Bcircle = thyroid to background ratio using background circle; TcUneck = percentage technetium uptake using background neck; TcUcopyROI = percentage technetium uptake using background copy region of interest; TcUcircle = percentage technetium uptake using background circle; TT4 = total thyroxine
Without correction for the administered activity of radioiodine
Significant effects on therapy outcome were only found for the T/S ratio and T/Bcircle ratio, with an increasing probability of persistent hyperthyroidism with increasing values for the T/S and T/Bcircle ratios. The OR of persistent hyperthyroidism vs a euthyroid outcome per unit increase in the T/S ratio equals 1.29 (P = 0.010), and the OR of persistent hyperthyroidism vs a low TT4 outcome per unit increase in the T/S ratio equals 1.28 (P = 0.018). The OR of persistent hyperthyroidism vs a euthyroid outcome per unit increase in T/Bcircle ratio equals 1.09 (P = 0.048), and the OR of persistent hyperthyroidism vs a low TT4 outcome per unit increase in the T/Bcircle ratio equals 1.08 (P = 0.046). Both latter ORs are close to 1 and therefore clinically not relevant.
Comparing the different outcome groups, significant differences were found for the T/S ratio between persistent hyperthyroid and euthyroid cats (P = 0.001) and between persistent hyperthyroid cats and cats with a low TT4 outcome (P = 0.004). This is similar for the T/Bcircle ratio, between persistent hyperthyroid and euthyroid cats (P = 0.003) and between persistent hyperthyroid cats and cats with a low TT4 outcome (P = 0.003). None of the other parameters showed a significant correlation with the therapy outcome. Additionally, the effect of multiple hyperactive foci on the pertechnetate scan vs a single affected thyroid lobe was also included in the analysis, but no significance was reached.
The T/S ratio and T/Bcircle ratio values are presented by box plots per therapy outcome group in Figure 1. For the T/Bcircle ratio a large overlap was observed between the three outcome categories. For the T/S ratio this overlap was also present for low TT4 and euthyroid outcome categories, but to a smaller extent for the persistent hyperthyroid category, and the median T/S ratio in the persistent hyperthyroid group (10.1) was almost double of the median T/S ratio of cats that were euthyroid at 6 months after therapy (5.1). ROC curve analysis, maxi-mising sensitivity and specificity, was carried out for the best performing parameter, the T/S ratio, and is shown in Figure 2. When comparing persistent hyperthyroid cats with cats with a low TT4 outcome, the sensitivity equals 73% and the specificity 72% when using a cut-off of 5.29. When comparing persistent hyperthyroid cats with cats with a successful euthyroid outcome, the sensitivity was 73% and the specificity 59% when using a cut-off of 5.40.

Box plot representation of the thyroid to salivary gland (T/S) ratio and the thyroid to background ratio using background circle (T/Bcircle) for each therapy outcome group. A large overlap is seen between the euthyroid and low total thyroxine (TT4) groups for both the T/S and T/Bcircle ratio. Overlap with the persistent hyperthyroid group is also present for both ratios but to a much lesser extent for the T/S ratio
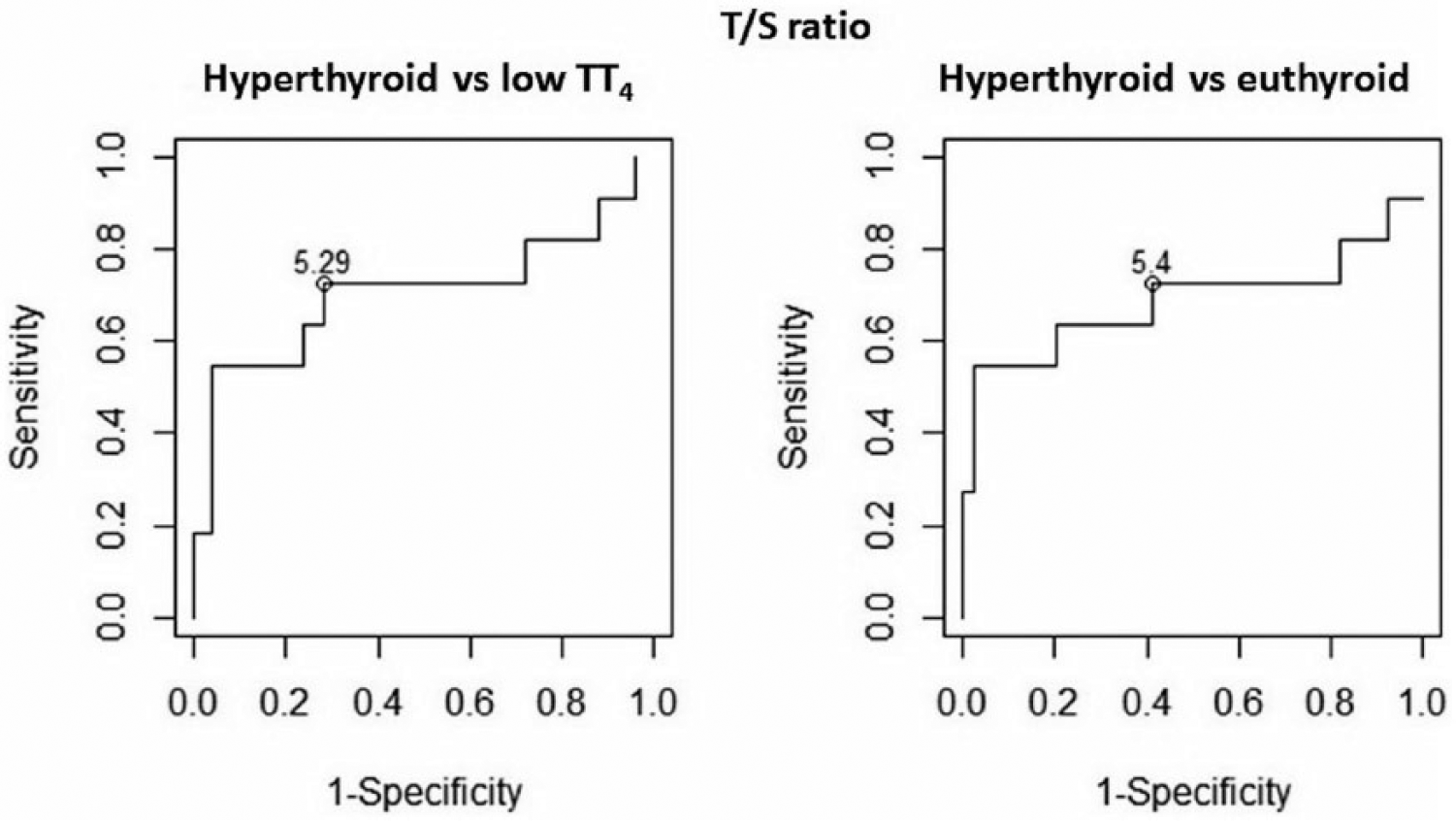
Receiver operating characteristic curves for the thyroid to salivary gland (T/S) ratio. Comparing persistent hyperthyroid cats with those with a low total thyroxine (TT4) outcome a cut-off value of 5.29 was associated with a sensitivity of 73% and a specificity of 72%. Comparing persistent hyperthyroid cats with those with a final euthyroid outcome a cut-off value of 5.4 was associated with a sensitivity of 73% and a specificity of 59%
With correction for the administered activity of radioiodine
When correction for the injected activity of radioiodine was included, the values slightly changed. The OR of persistent hyperthyroidism vs a euthyroid outcome per unit increase in the T/S ratio increased to 1.33 (P = 0.021), and the OR of persistent hyperthyroidism vs a low TT4 outcome per unit increase in the T/S ratio increased to 1.90 (P = 0.018). In contrast, for the comparison of persistent hyperthyroid cats vs those with a final euthyroid outcome, the T/Bcircle ratio no longer showed a significant difference (P = 0.095). Regarding the comparison of persistent hyperthyroidism vs a low TT4 outcome, all three T/B ratio methods were found to be significant. The OR per unit increase for the T/Bcircle ratio was 1.21 (P = 0.009), for the T/Bneck ratio this was 1.3 (P = 0.015) and for the T/BcopyROI ratio this was 1.17 (P = 0.015).
Again comparing the different outcome groups, the differences between persistent hyperthyroid and euthyroid cats (P = 0.004) and between persistent hyperthyroid cats and cats with a low TT4 outcome (P = 0.0003) remained significant for the T/S ratio. The significant difference in T/Bcircle ratio between persistent hyperthyroid and euthyroid cats was lost in this second analysis (P = 0.076), but significance was reached for the three methods of T/B ratio calculation, between persistent hyperthyroid cats and cats with a low TT4 outcome (T/Bcircle ratio: P = 0.001; T/Bneck ratio: P = 0.003; T/Bcopy ROI ratio: P = 0.002).
None of the other parameters, including the number of hyperactive foci, showed a significant correlation with the therapy outcome.
Discussion
The semi-quantitative and quantitative scintigraphic parameters described in this study represent an estimation of thyroid follicular cell activity and the amount of pertechnetate uptake in the thyroid gland. Because pertechnetate and radioiodine are taken up by the same receptors, the diagnostic pertechnetate scan allows a safe and fast estimation of thyroid gland activity that can also be used for the therapeutic radioiodine activity determination.7,8,16,23 The uptake of pertechnetate and radiodine is variable between patients and can be influenced by a number of external factors, such as the use of iodinated contrast media prior to the procedure, the amount of dietary iodine intake or the use of antithyroid medication.16,24–29 None of the cats in this study had recently received iodinated contrast media and all cats were off antithyroid medication for a minimum of 10 days before the diagnostic pertechnetate scan and radioiodine treatment. Neither of these factors were therefore suspected to play a role in our group of hyperthyroid cats. A limitation of the study, however, is that the nutritional iodine intake of these cats is unknown. All cats were on commercial diets prior to and after the study, and these diets may vary in iodine content and bioavailability of this nutritional iodine.30,31 However, this will represent the general feline population that forms the veterinary clientele. Owing to the retrospective nature of this study, another limitation is that both the diagnostic and follow-up TT4 measurements were performed by the referring veterinarian. Therefore, the test methods and reference intervals used for the serum TT4 measurements were not uniform across this group. Reference intervals may vary between different laboratories, and differences in test sensitivity could have affected the outcome categorisation of the cats at 6 months post-therapy. At the same time concurrent non-thyroid-related illness was excluded based only on physical examination and information provided by the owners, and extra tests were not performed. Furthermore, given that the cats’ scans were retrospectively selected, the inclusion criteria may have created bias in the cat selection. The outcome results therefore do not necessarily represent the general outcome of radioiodine therapy in our clinic. Finally, the number of cats included in this study, and more specifically the number of cats in the persistent hyperthyroid outcome group (n = 11), is relatively low.
(Semi-)quantifications using sodium pertechnetate remain, of course, an estimation of the amount of radioiodine activity that will be taken up by the thyroid gland and, unlike radioiodine, pertechnetate will not be incorporated in thyroid hormones. However, using radio-iodine-131 in pre-therapy studies is not only less safe from a radioprotective point of view, but tracer studies intended to calculate the therapeutic radioiodine activity are also associated with limitations such as differences between the delivered radioiodine thyroid dose and the intended dose.17,19,23,32
In accordance with what has been reported in humans with Graves’ disease, the results of this study show a high T/S ratio, representative of high thyroid gland uptake, to increase the risk of persistent hyperthyroidism.17,18,20,21 A higher uptake of pertechnetate suggests there will be a higher uptake of radioiodine by the thyroid gland, and therefore more destruction of the hyperfunctional thyroid tissue could be expected. However, in humans with Graves’ disease an increased turnover of radioiodine has also been reported to result in more patients with persistent hyperthyroidism. 21 An increased turnover will reduce the residence time of radioiodine within the thyroid gland to cause tissue destruction. Also in hyperthyroid cats, an increased turnover of radioiodine has been observed compared with euthyroid control cats. 33 Although a relationship between an increased radioiodine uptake and an increased turnover in hyperthyroid patients has not yet been described, it might explain the findings in this study where a higher T/S ratio will increase the chance of persistent hyperthyroidism.
Wallack et al described a significant relationship between an increased T/Bcircle ratio and a persistent hyperthyroid outcome and suggested an increased radioiodine dose for patients with a T/B ratio ⩾11. 12 The T/Bcircle ratio in this study no longer showed a significant effect on therapy outcome between persistent hyperthyroid and final euthyroid cats when correction for the amount of injected radioiodine was included in the analysis. Even without dose correction the ORs were low, the amount of overlap between the outcome categories was large and ROC curve analysis was therefore not performed for this parameter.
Although the T/S ratio, T/B ratio and %TcU all represent thyroid gland uptake, the results of this study only showed the T/S ratio as having a significant relationship with the outcome of radioiodine therapy in cats; this is in contrast to what has previously been reported in the veterinary literature.10,12 The reason for the discrepancy between the different parameters is unclear, but the aforementioned limitations of this study may have influenced this result. Whereas the two previous studies in cats used a fixed amount of radioiodine, the amount of injected radioiodine was determined using a scoring system in the current study.10,12 A second analysis correcting for this protocol was performed, and confirmed, with an increased OR, the significant relationship of an increased T/S ratio with a persistent hyperthyroid outcome. ROC curve analysis suggested a T/S ratio cut-off value of 5.4 representing an increased risk of persistent hyperthyroidism after therapy. The sensitivity (73%) of this threshold was acceptable, and could be interpreted as a suggestion to increase the activity of radioiodine administered to patients with a T/S ratio ⩾5.4. However, the specificity (59%) was only modest and increased radioiodine activity could consequently lead to a significant number of patients being relatively overdosed. The use of this cut-off value to alter treatment protocols therefore needs a careful approach and future prospective studies are needed to confirm or refute its value.
Using the T/S ratio remains an operator-dependent procedure. No fixed-size ROIs can be used as the size and shape of thyroid and salivary glands vary from cat to cat. However, in a previous study we reported that the T/S ratio shows little inter- and intra-observer variability, and its use in practice is preferred over the T/B ratio or %TcU. 34
As well as being influenced by thyroid gland uptake, the T/S ratio might also be influenced by salivary gland uptake, the denominator of the ratio. The salivary gland percentage technetium uptake in a group of healthy, euthyroid cats showed no relevant week-to-week variation and the amount of uptake was similar to the uptake observed in a study with hyperthyroid cats. It could therefore be assumed that hyperthyroidism as such has little or no effect on the uptake of pertechnetate by the salivary glands.34,35 Moreover, salivary gland disease is rare in cats and its active uptake of pertechnetate may result in less variable uptake compared with the peripheral soft tissues used in the calculation of the T/B ratio.16,26,36,37 In patients with high pertechnetate uptake in the thyroid gland, the patient’s body silhouette may become difficult to visualise on the scan. The active pertechnetate uptake of the salivary glands will be useful as their increased uptake compared with the surrounding tissues will create a better delineation of the salivary glands for drawing the required ROIs.
For cats with a low TT4 outcome no significant relationships with any of the (semi-)quantitative parameters in this study were observed. To our knowledge there are no previous reports on this subject in cats. In the human literature there is a study that, in contrast to most literature, reported a faster progression towards or an increased risk of hypothyroidism with an increased radioiodine uptake. However, turnover of the radioiodine was also not investigated in that study and with a follow-up period of 20 years the outcome is difficult to compare with the group of cats in this study. 38
The therapeutic effect of radioiodine is not only dependent on the uptake of radioiodine or its residence time within the thyroid gland tissue, but also on the excretion from the body. The elimination of radioiodine from the body happens primarily through the kidneys. 26 Thyroid and renal function are closely connected and although renal function was not included as a parameter in this study, chronic kidney disease is a commonly occurring disease in older cats.39,40 The effect of patient renal function on radioiodine therapy outcome could therefore be an interesting focus of future research.
In contrast to previous studies there was no significant relationship between cats affected by multiple affected foci, either bilaterally or bilaterally with additional ectopic thyroid tissue, and a low TT4 outcome.11,15 These latter studies included a similar number of cats and both had more than twice the number of patients than in this study, possibly explaining the difference in results.
Aside from the aforementioned factors, the outcome of radioiodine therapy is suspected to be influenced by multiple factors; for example, thyroid volume, the occurrence of multifocal disease, the pre-therapy TT4 and, potentially, the previous use of antithyroid medication. This complicates the research on this topic and possibly explains some of the contradicting results in different studies.8,9,10,11,15,24
Conclusions
Performing a pertechnetate thyroid scan prior to the radioiodine treatment and processing of the images is fast and easy. The results from this study suggest that the T/S ratio is the preferential method of semi-quantifying thyroid gland uptake and a threshold value of 5.4 is a possible indicator of an increased risk of persistent hyperthyroidism. No significant relationships were found in this study for cats with a low TT4 outcome. Future, ideally prospective, studies are needed to confirm these findings and assess other factors, such as renal function, that might play an important influencing role on radioiodine therapy outcome.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.