
Abstract
Objectives:
This paper, the first in a series of three on ‘feline leprosy’, provides a detailed description of disease referable to Candidatus ‘Mycobacterium tarwinense’, the most common cause of feline leprosy in Victoria, Australia.
Methods:
Cases were sourced retrospectively and prospectively for this observational study, describing clinical, geographical and molecular microbiological data for cats definitively diagnosed with Candidatus ‘M tarwinense’ infection.
Results:
A total of 145 cases of feline leprosy were scrutinised; 114 ‘new’ cases were sourced from the Victorian Infectious Diseases Reference Laboratory records, veterinary pathology laboratories or veterinarians, and 31 cases were derived from six published studies. Forty-two cats were definitively diagnosed with Candidatus ‘M tarwinense’ infection. Typically, cats were between 3 and 11 years of age, with no gender predilection, and were generally systemically well. All had outdoor access. Most cats underwent surgical resection of lesions with adjunctive medical therapy, often utilising a combination of oral clarithromycin and rifampicin for at least 3 months. Prognosis for recovery was generally good. Resolution of lesions was not observed in the absence of treatment, but a number of untreated cats continued to enjoy an acceptable quality of life despite persistence of the disease, which extended locally but did not appear to disseminate to internal organs. Preliminary results of draft genome sequencing confirmed that the species is a member of the Mycobacterium simiae complex.
Conclusions and relevance:
Candidatus ‘M tarwinense’, a fastidious member of the M simiae complex, is capable of causing feline leprosy with a tendency to produce lesions on the head, particularly involving the eyes and periocular skin. The disease has an indolent clinical course and generally responds favourably to therapy despite lesions often containing large numbers of organisms. Detailed genomic analysis may yield clues as to the environmental niche and culture requirement of this elusive organism. Prospective treatment trials and/or drug susceptibility testing in specialised systems would further inform treatment recommendations.
Introduction
‘Feline leprosy’ is a skin condition caused by a variety of fastidious mycobacterial species, which, by definition, will not routinely grow on synthetic media in the laboratory. The disease was first described in 1962 in urban-dwelling cats from Auckland, New Zealand, which presented with subcutaneous nodules containing acid-fast bacilli (AFB). 1 In the first decade or so after the initial report, cats with what appeared to be the same condition were reported in eastern Australia,2,3 western Canada, 4 the United Kingdom (UK),5,6 southwestern USA 7 and the Netherlands. 8 More recently, the condition has been identified in cats domiciled in France,9,10 New Caledonia, 10 Italy, 11 the Greek islands 12 and Japan. 13
Based on rodent inoculation studies,3,8,14 and delayed-type hypersensitivity skin reactions between feline ‘lepromin’ and Mycobacterium lepraemurium, 15 it was long assumed that this latter organism was the sole causative agent of feline leprosy. Hughes and colleagues, 16 in a seminal paper, demonstrated that the aetiology of feline leprosy was heterogeneous and could not be ascribed to M lepraemurium alone. That, and subsequent studies by this present group and others in North America, identified the involvement of at least three other fastidious species of mycobacteria:
A novel mycobacterial species we propose be provisionally called Candidatus ‘Mycobacterium tarwinense’, 17 related to the Mycobacterium simiae group;
A second novel mycobacterial species related to Mycobacterium leprae and Mycobacterium lepromatosis, which we propose be provisionally called Candidatus ‘Mycobacterium lepraefelis’, found along the eastern coast of Australia and both islands of New Zealand9,16,18,19 (and perhaps Canada 20 );
Mycobacterium visibile (erroneously called Mycobacterium visibilis), documented in cats from western Canada, and the states of Idaho and oregon in the Pacific Northwest of the USA. 21

The last organism is phylogenetically similar to Candidatus ‘M lepraefelis’, although no further reports of the disease have emerged since the studies in the 1990s, so the species remains largely uncharacterised. Infections caused by members of the Mycobacterium avium complex, 22 Mycobacterium ulcerans 23 and other slow-growing mycobacteria can resemble feline leprosy in some respects, but with careful specimen collection and handling it is possible to isolate these organisms by culture in liquid or on solid mycobacterial media in vitro.
Progress in unravelling the epidemiology of fastidious mycobacterial infections in cats has been hampered by the requirement to access the technological expertise and finances to establish a definitive diagnosis via molecular methodologies. Indeed, in a large case series concerning feline mycobacteriosis in the UK, the causative agent was only established in 47% of cases, principally because molecular methods were not used to augment traditional mycobacterial culture and identification methods. 24
Previous studies of feline leprosy have yielded preliminary insights into the epidemiology of this disease, although these investigations were limited by small case numbers and relatively short periods of follow-up. This paper, the first in a series of three, seeks to extend those findings by providing a detailed description of feline leprosy cases referable to Candidatus ‘M tarwinense’, the most common cause of this condition in Victoria, Australia. Subsequent papers will concern M lepraemurium and Candidatus ‘M lepraefelis’ (see right).

Materials and methods
Case recruitment, demographics and data retrieval
Cases were identified by a review of the record database of the Mycobacterium Reference Laboratory of the Victorian infectious Diseases Reference Laboratory (VIDRL) from 1998–2015. During the period 2008–2014, active case recruitment was carried out by contacting veterinarians and veterinary pathologists, and via notification in a variety of newsletters and other publications (eg, Journal of Feline Medicine and Surgery, Control & Therapy Series of the Centre for Veterinary Education), as well as via e-mail groups and direct mail. Prospective clinical and/or necropsy data were retrieved with owner consent from case records of the primary veterinarians, where possible. Historical cases from the literature were sourced via online resources (PubMed, Web of Knowledge, CAB Abstracts, Medline and Google Scholar) using the search terms ‘cat or cats or feline’, ‘leprosy’ and ‘mycobacteri*’. Cases were only included in the study if the causal species had been definitively identified using molecular methods.
Where available, data such as estimated age at time of diagnosis, gender, breed, geographical location of domicile (postcode), lifestyle and/or other potentially contributing factors (eg, fight wounds, immunosuppressive drug therapy), anatomical location and nature of lesions (single vs multiple, ulcerated vs intact nodules), results of necropsy examination (including cytology and/or histopathology), retroviral status (where available), treatment (drug therapy and/or surgery) and outcome were recorded.
Clinical disease was classified as: few (one to two) or multiple (three or more) nodules, generally affecting one or more of the following anatomical regions: head, forelimbs, hindlimbs, body and tail/perineum. Cats with innumerate nodules covering many areas of the body were classified as having generalised nodular skin disease.
Many cats were treated with at least some input from the authors concerning case management. Unfortunately, cats were not treated in a consistent manner, as each cat/client situation required a different approach; vis-à-vis requirement for once daily therapy vs twice daily therapy, surgery allowed vs not permitted, cat difficult to medicate, owner financially constrained, and so forth.
Cytology/histology
In most cases, fine-needle aspirates from representative lesions were stained using Ziehl–Neelsen (ZN) and/or a rapid modified Romanowsky stain (eg, Diff Quik, Rapid stain), and the presence of mycobacteria was suggested by the observation of AFB or ‘negatively stained bacilli’ (NSB), respectively. Biopsy specimens were fixed in formalin for 12–48 h, embedded in paraffin, cut to 5 μm thickness and stained using haematoxylin and eosin (H&E) and either ZN or Fite’s stain, and examined using conventional light microscopy. Such cytological and histological preparations were also used to harvest material suitable for PCR testing (see later). 25
Enumeration of AFB/NSB was performed on either cytological or histopathological samples and the following categories of bacterial index (BI) 26 ascribed:

The terms ‘paucibacillary’ and ‘multibacillary’ have been used in previous publications to describe bacterial numbers in lesions;19,27 however, to avoid confusion the authors have elected not to use these terms in this series of papers. These classifications have been expanded in the human leprosy field to include reference to the number and type of lesions observed, whether involvement of peripheral nerves is a feature, the presumed ‘infectiousness’ of a patient and the recommended duration and type of therapy. 28 These classifications do not apply for feline patients.
As the availability, type and degree of detail of reported cytological and histopathological data varied widely for each patient, these data were not included in the results.
Molecular microbiology methods
DNA was extracted from fresh tissue, methanol-fixed stained and unstained cytology samples (typically aspirates of cutaneous nodules), or de-waxed paraffin-embedded tissue, using methods described elsewhere.17,25–29
Initial identification of the aetiological agent was generally performed by amplification and sequencing of the internal transcribed spacer (ITS) region, using a nested PCR protocol described previously. 17 Some later cases were identified via multiplex real-time (qPCR) assay using the following protocol (this was typically confirmed via subsequent sequencing of the ITS region). The 20 μl PCR reaction contained 10 μl of SensiFAST Probe Lo-Rox mix (Bioline Reagents) forward and reverse primers at a concentration of 8 μM (1 μl each), probe at a concentration of 2 μM (1 μl), 3.6 μl of nucleotide-free water (NFW) and 1 μl of DNA template. Internal positive control reagents (TaqMan Exogenous internal Positive Control Reagents; Applied Biosystems) were used in the following amounts per reaction: 2 μl 10x Exo IPC Mix, 0.4 μl 50x Exo IPC.
The primers for the conventional and real-time PCR assays are shown in Table 1. Amplification and detection were performed with the ABi Prism 7500 Fast Real-Time PCR system (Applied Biosystems) using the following programme: one cycle of 95°C for 5 mins and 40 cycles of 95°C for 10 s and 60°C for 30 s.
Details of primers used in the PCR methods

Amplification of the hsp65, rpoB and sodA regions was also performed using the primers listed in Table 1 and under the conditions described by Devulder and colleagues, 35 except for sodA, which was run as a nested PCR. Briefly, 5 μl of template DNA was added to 20 μl of the first-round PCR mixture containing 5 μl 10x PCR buffer with 1.5 mM MgCl2, 10 μl Q solution (Qiagen), 200 μM deoxynucleoside triphosphates (dNTPs), primers Z205 and Z212 (at 2 μM each), and 0.25 μl of Taq DNA polymerase (Qiagen) and 10.75 μl NFW. The amplification was performed with a Mastercycler gradient (Eppendorf) using the following profile: 95°C for 5 mins, followed by 38 cycles of 94°C for 1 min, 62°C for 1 min and 72°C for 1 min. The second-round PCR mixture contained 2.5 μl of the first-round PCR product in a final 50 μl volume containing PCR buffer with 1.5 mM MgCl2 (Qiagen), 200 μM dNTPs, primers ‘Tarwin long sodAF’ and ‘Tarwin long sodAR’ (at 2 μM each), and 0.25 μl Taq DNA polymerase (Qiagen). After mid-2013, MyTaq Mix (Bioline) was used, as per the manufacturer’s instructions, instead of the Qiagen reagents in conventional PCR assays. Negative extraction controls were included in each instance.
Genetic analysis
DNA sequencing was performed as previously described 17 using the primers listed in Table 1. Negative PCR controls were used in each instance. Sequence data were edited and analysed using either the Bionumerics v4.0 (Applied Maths) or MacVector v14.0.4 (MacVector) programs. Sequences were aligned using ClustalW and curated manually from chromatographic data.
Mycobacterial culture
Attempts at culture of this organism have been described previously. 17 In summary, fresh tissue samples were homogenised in bead bottles with Ringer’s solution and were decontaminated with an equal volume of 2% sodium hydroxide, incubating at room temperature for 15 mins and neutralising with 10% orthophosphoric acid (modified Petroff method). Samples were centrifuged at 4000 rpm for 20 mins and pellets resuspended in 2 ml Ringer’s solution. A quantity of 400 μl of the decontaminated suspension was used as an inoculum for a variety of liquid and solid media, including Mycobacteria Growth Indicator Tube (MGIT) broths with PANTA added according to the manufacturer’s recommendations (BD), Löwenstein–Jensen medium (with and without a 1% ferric ammonium citrate supplement), Brown and Buckle medium, chocolate agar, 7H10 slopes with antibiotics (25 μg/ml piperacillin, 50 μg/ml amphotericin, 25 μg/ml vancomycin, 800 mg/ml actidione, 4 μg/ml aztreonam) and buffered charcoal yeast extract medium. Cultures were incubated aerobically, and in some cases microaerophilically, at 31°C, 36°C and 43°C and were monitored weekly for up to 12–16 weeks.
Statistical analysis
Two-tailed Fisher’s exact and X2 tests were used to assess associations between categorical variables, and the Mann–Whitney test was used to compare continuous variables, using an online epidemiological statistical resource (OpenEpi). P values <0.05 were considered significant.
Results
Clinical data
A total of 145 cases of feline leprosy were scrutinised as part of this study; 114 cases were sourced from the VIDRL records, veterinary pathology laboratories or veterinarians, with an additional 31 cases derived from six published studies.10,12,16,17,19,20 Of this total, 42 cats were infected with Candidatus ‘M tarwinense’. Twenty-seven were ‘new’ cases, while 15 had been previously reported, all by the current group of authors. For the 15 previously reported cases, the follow-up obtained for this case series was more detailed and of a much longer duration (15 years in one instance).

Median age at diagnosis was 6.8 years (range 1–18). Where gender was recorded, 17/39 (44%) Candidatus ‘M tarwinense’ cases were male. Where breed was recorded, 25/36 cats were domestic shorthair, 1/36 was a domestic mediumhair, 6/36 were domestic longhair, and there was one each of Burmese cross, Abyssinian cross, Russian Blue cross and Ragdoll. Geographical location data were recorded for 37 cats (Figure 1), revealing that all but two were domiciled in a restricted area of south-eastern Victoria. The two discordant cases were from Lane Cove, Sydney, and the Central Coast of New South Wales (NSW), near Gosford. 37

Geographical distribution of feline infections caused by Candidatus ‘M tarwinense’ (shown in green). All except for two cases in New South Wales (one in a suburban area of Sydney, another on the Central Coast near Gosford; arrows) are clustered in south-eastern Victoria. No cases were encountered in New Zealand, Tasmania or anywhere else in the world
Where lifestyle was recorded, all cats had unsupervised outdoor access and many were known hunters and/or fighters. only one cat (case 8) had previous immunosuppressive drug therapy prior to the diagnosis of feline leprosy. Feline immunodeficiency virus (FIV) status was only recorded in seven cases, with 3/7 cats being antibody positive. As far as could be ascertained from the case records, none of the FIV-positive cases had received prior FiV vaccination. No cats were tested for feline leukaemia virus antigen.


Where clinical features and clinical course were well documented in the available case records, 30/40 (75%) cats with Candidatus ‘M tarwinense’ infection had only a few localised nodular lesions. These were predominantly (33 cases) located on the head (specifically in ocular and periocular locations in 13 cases; Figures 2 and 3) and forelimbs (12 cases; Figure 4). Four cats had intraoral lesions (Figure 5). Eight cases had multiple lesions, often at disparate anatomical sites, with two cats having generalised nodular cutaneous disease (one of these cats was recorded as FiV negative). There was no difference in age within this cohort between cats with a few lesions (median 6 years, range 1–17) vs those with multiple nodules (median 6.5 years, range 3–14) (P = 0.58232). There also did not appear to be an association between the number of lesions and the likelihood of resolution of disease with therapy (P = 0.3544, data not shown).
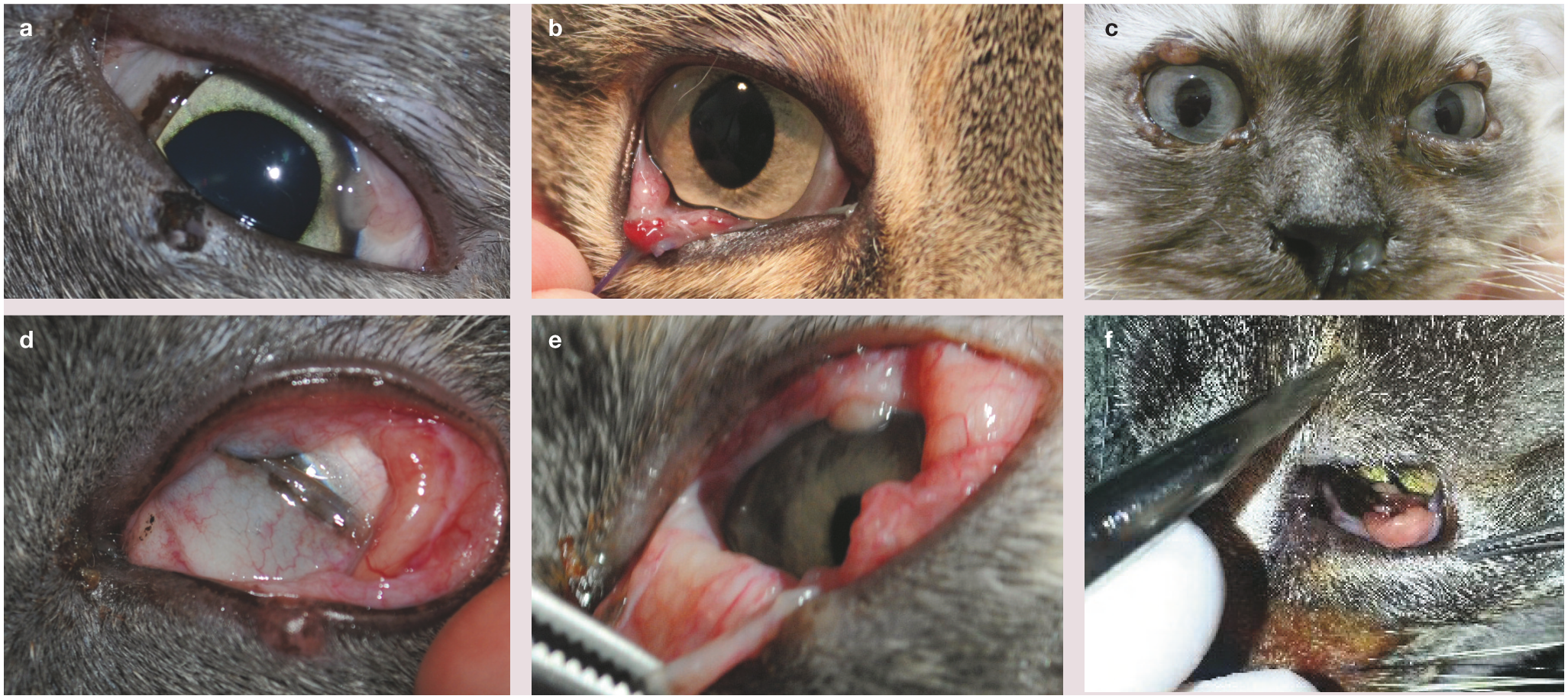
Representative photographs of Candidatus ‘M tarwinense’ infection in cats fromVictoria, Australia, chosen to illustrate the occurrence of lesions near the eyes. These six photographs of different patients emphasise the propensity of lesions to occur on ocular structures, including the nictitating membrane (a), conjunctiva (b,d–f) and eyelids (c)

Representative photographs of Candidatus ‘M tarwinense’ infection in cats fromVictoria, Australia, chosen to illustrate the presence of lesions on the oculonasal skin. These six photographs of different patients illustrate the range of lesions that may be encountered, including an ulcerated lesion on the nasal planum (a), involvement of the bridge of the nose (b,c) and lips (d,e), and a lesion adjacent to the naris (f). (a) Image courtesy of Dr Robert Hilton; reproduced from Malik et al, 27 with permission; (d) reproduced from Little, 38 with permission

Representative photographs of Candidatus ‘M tarwinense’ infection in two cats fromVictoria, Australia, illustrating the presence of lesions on the distal forelimbs

Representative photograph of Candidatus ‘M tarwinense’ infection in a cat in Victoria, Australia, illustrating the presence of a lesion on the gum. Reproduced from Little, 38 with permission
The influence of bacterial number in lesions and clinical presentation, disease course and outcome could not be assessed due to a paucity of cases classified as having ‘low BI’ lesions.
One cat in the study cohort underwent necropsy examination (case 5). The cat had been diagnosed with the disease 8 years previously and had received no treatment. Histological examination of all internal organs, excluding the central nervous system, failed to demonstrate any evidence of systemic mycobacteriosis (ie, infection was limited to superficial structures, with no involvement of the chest or abdomen).
Treatment and outcome data
As there are no published guidelines concerning the management of fastidious mycobacterial infections in cats, treatment protocols varied widely and often were influenced by practical considerations such as owner finances and commitment, and patient temperament.
Where it was possible to implement medical therapy, protocols typically included several months of treatment with one or more of the following drugs: rifampicin, clarithromycin, clofazimine, a fluoroquinolone (enrofloxacin, marbofloxacin or moxifloxacin) and doxycycline. Most cases also underwent surgical resection of most, if not all, lesions (often as the initial procedure used to establish a diagnosis).
Reliable follow-up was available for 18 cases (range 1–15 years, mean 5.6 ± 4.6). In the 13 cases where treatment was successful, rifampicin plus clarithromycin (with or without surgery) was utilised most commonly (six resolved cases); clarithromycin plus moxifloxacin with surgery was utilised in two resolved cases, and clarithromycin monotherapy (with or without surgery) was utilised in three resolved cases. Clofazimine monotherapy plus surgery was also successful in one case. one cat was treated successfully with surgical resection alone (albeit in two attempts when more lesions developed). overall a combination of surgical resection (often with incomplete margins due to the anatomical location of the lesions) and follow-up medical therapy was used in 10 cases. Medical therapy alone was used in three cases.
Among the 18 cases with follow-up data, at least two cats went on to have complete clearance of lesions despite having multiple cutaneous lesions persisting at the time when medical therapy was discontinued. Also, four cases had persistent disease where therapy was either declined or suboptimally administered.
Five treated cases had no follow-up data and were not included in the results above. Unfortunately, case numbers were not sufficient to undertake statistical comparison of treatment protocols and outcome.
The overall outcome was typically favourable, with complete resolution of lesions in 68% of cases where follow-up was available. Even if lesions did not resolve completely (or at all), two cats continued to live for a relatively long time (8 and 10 years) (Figure 6). Where cats were euthanased because of the disease, this was typically due to progressive or persistent cutaneous lesions, rather than evidence of systemic illness, such as lethargy, anorexia or weight loss. Sadly, two cats in the study were also euthanased at the time of diagnosis due to (likely erroneous) perceived zoonotic risks.

Demonstration of the unrelenting progression of lesions in a cat (case 35). Infection was initially diagnosed in 2006 (a) and over the subsequent 8 years only poor attempts at therapy were made. Images (b) and (c) were obtained in 2014. This cat was apparently still alive at the time of writing. (a) Reproduced from Fyfe et al, 17 with permission
A summary of data concerning age, gender, anatomical distribution of lesions and outcome for cats infected with Candidatus ‘M tarwinense’ is provided in Table 2.
Detailed case data for 42 cats infected with Candidatus ‘Mycobacterium tarwinense’




F = female; FN = female spayed; M = male; MN = male castrated; ? = neuter status unknown; DSH = domestic shorthair; DMH = domestic mediumhair; DLH = domestic longhair; NSW = New South Wales; VIC = Victoria; FIV = feline immunodeficiency virus; FeLV = feline leukaemia virus; +ve = positive; −ve = negative; NR = not recorded; CLFZ = clofazamine; RIF = rifampicin; CLM = clarithromycin; DOXY = doxycycline; ENFLX = enrofloxacin; OFLX = ofloxacin; MOXIFLX = moxifloxacin; LTFU = lost to follow-up
Microbiological and molecular data
All attempts at isolation, including use of MGiT and solid media, were unsuccessful.
Fresh tissue, and fixed cytological and paraffin-embedded samples from 38 cases underwent DNA extraction, PCR amplification and sequencing. Mycobacterial DNA derived from fresh biopsy tissue from case 30 underwent draft genome sequencing during the course of the study. The methods and results of these investigations will be published in full separately (C o’Brien et al, manuscript in preparation).
Limited multilocus sequence analysis demonstrated that this organism was clonal, with 100% genetic homogeneity at all five loci examined (V3 region of 16S rRNA, ITS region, rpoB, hsp65, sodA). Known acquired mutations in the rpoB gene conferring rifampicin resistance in other mycobacterial species39–41 were not found in any of the isolates in this study.
Discussion
This study greatly extends the body of knowledge concerning Candidatus ‘M tarwinense’ infections in cats. The original paper on this pathogen involved a small number of cases, with limited and often incomplete follow-up. 17 The inclusion of many ‘new’ cases in this study cohort, as well as the original cases (with longer and generally more complete followup), gives a better picture of the disease associated with this organism.
Geographical distribution
While the original cases were from the Tarwin region of rural south-eastern Victoria, subsequent cases have had a wider geographical footprint; although on a national or global scale cases are still remarkably restricted (a 900 square kilometer area of coastal Victoria, with two isolated cases in coastal NSW). The number of infections that have been encountered per year has increased progressively since the first identification of this organism as a cause of feline leproid lesions (Janet Fyfe, unpublished observations), suggesting either that this is an emerging infectious disease, or that small animal clinicians and veterinary pathologists are more aware, and thus more adept, at identifying these cases and submitting appropriate material for definitive molecular diagnosis. The ability to use methanol-fixed Romanowsky-stained slides as a source of DNA 25 has greatly facilitated the cost-effective and timely diagnosis of this condition in practice, as there is no requirement to re-sedate or anaesthetise the patient to obtain additional material for molecular diagnostics.
The strong propensity for cases to be domiciled in Victoria is reminiscent of the situation in people and other animals with M ulcerans infection. However, a close examination of the location of feline Candidatus ‘M tarwinense’ cases and M ulcerans cases in people, dogs, 42 horses, 43 alpacas 44 and possums 45 show them to occur in somewhat different specific regions within the broader area of southern Victoria, although there is a significant overlap of endemic range on the Mornington Peninsula. 46
Anatomical predilection
More than any other feline mycobacterial pathogen, this organism has a predilection to involve structures about the head, especially the ocular tissues (conjunctiva, cornea, eyelids, nictitating membrane), and nasal and periocular skin and subcutis (Table 3). This poses some unique problems therapeutically, as the cornea is a difficult area in which to obtain adequate concentrations of many antimicrobials, and hence surgical and topical therapy is needed in such patients to effect a cure.
Summary data concerning age, gender, anatomical distribution of lesions and outcome for cats infected by Candidatus ‘M tarwinense’

BI = bacterial index
The preponderance of lesions located on the face suggests a cat scratch injury or a bite/ scratch from prey as a potentially important antecedent event.47,48 Furthermore, the propensity for cats to dig with the forelimbs prior to defecation affords the opportunity for many saprophytes to be present on the claws, and cat scratches provide the break in integrity of the cutaneous epithelial barrier to permit saprophytes to establish infections in this location. 47 Alternatively, the habit of cats to groom the face with the front paws provides a potential route for the inoculation of organisms, especially into the periocular area.
Signalment
The age range of affected cats is wide and the ratio of affected males to females is not too disparate to the age/gender pyramid of healthy cats. 49 Likewise, the breakdown of domestic crossbreeds vs pedigree cats is in accord with their ratio in the overall Australian cat population. 49 (No equivalent data are available for cats domiciled in New Zealand.) There were too few cats subjected to retroviral testing to draw any firm conclusions, but it may be that 43% FIV positivity (3/7 cats) is higher in this group of affected cats when compared with the overall prevalence of FIV infection in Australian cats, which is in the order of 8%. 50 This might be an epiphenomenon, reflecting the tendency of cats with outdoor access and which fight to acquire FiV or Candidatus ‘M tarwinense’ through independent mechanisms.
Clinical course
The clinical course of Candidatus ‘M tarwinense’ infection in cats could perhaps be described as indolent, with lesions tending to progress inexorably in the absence of therapy. There appears to be little tendency for spread via the bloodstream or lymphatics, given there was no suggestion of internal organ involvement in any cat based on clinical criteria, nor in the one cat that underwent necropsy with microscopic examination of representative tissues.
Organism biology
This behaviour is consistent with an environmental saprophyte not adept to living at mammalian body temperature, with cats being an incidental ‘dead end’ host. Although the preferred temperature range for growth is not known, it is possible that this organism is not capable of replicating at the higher core temperature of the internal organs; as a result infection is limited to the skin and subcutis. If this is the case, the local application of heat might represent a useful adjunct to systemic antibacterial therapy, as it is in the management of Mycobacterium marinum and M ulcerans infections in human patients,51,52 although this may be practically difficult in cats.
The inability of Candidatus ‘M tarwinense’ to grow using traditional mycobacteriological methods remains a mystery, although it is hoped that detailed examination of the draft genome will yield some clues to the metabolic requirements of this organism. Analysis of several gene targets has demonstrated that all the clinical isolates that have been so examined are remarkably clonal, with 100% homogeneity at the five different loci studied. If this homogeneity is carried over the entire genome, the variation in clinical severity from cat to cat is perhaps a reflection of inoculum load and/or variability in the innate and acquired immunological response of the feline host. This genetic homogeneity is reminiscent of another fastidious mycobacterium – the unnamed agent of the canine leproid granuloma syndrome, which appears to be clonal over its far more extensive geographical range (Janet Fyfe, unpublished observations). 27

Treatment and outcome
As is typical in an observational study, treatment regimens were not consistent and case numbers in any category were not large enough to draw robust conclusions as to the effectiveness of a particular treatment strategy, although some inferences can be made via general inspection of the data (see box above).
Despite these limitations, favourable outcomes were obtained for approximately 70% of patients, and it would be reasonable to state that the prognosis is good for most cats, especially when a timely diagnosis is made at a point when lesions are small both in size and number. Importantly, even where therapy was not successful and lesions persisted, most cats could live a near-normal life for a substantial period, as the pathogen had no apparent propensity to disseminate haematogenously or via the lymphatics. Spontaneous resolution was never observed; that said, two cases were noted to have resolution of disease despite obviously suboptimal medical treatment. It is conceivable, however, that the above-mentioned residual lesions contained nonviable organisms only.
Risk of contagion
To date, there has been no instance of spread from cat to cat, or from cat to human. In the authors’ view, the risk of contagion from cats is slight; perhaps no greater than from other environmental sources harboring this organism (eg, soil). As the lesions are generally not ulcerated, organisms are more likely to be inoculated from a cat’s claws, than from intact subcutaneous nodules. it is fascinating that, to date, infections have not been seen in dogs or native animals. Very likely this species-specific disease association may eventually provide an insight into the environmental niche of this mycobacterium.
Key Points
Candidatus ‘M tarwinense’, a fastidious member of the M simiae complex, causes high Bl ‘feline leprosy’, with a tendency for lesions to consist of intact nodules present on the head, especially in proximity to the eyes and periocular skin, with an indolent clinical course and a generally favourable response to therapeutic interventions.
The best management approach consists of complete surgical resection of easily accessible lesions, and debulking of lesions in difficult anatomical locations, in combination with antimicrobial therapy using two or more agents with known activity against slow-growing mycobacteria, possibly including topical therapy for lesions involving the cornea and/or conjunctiva.
Further genomic analysis may yield clues as to the environmental niche and culture requirement of this elusive organism. Prospective trials and/or drug susceptibility testing in specialised systems, such as the microplate Alamar blue assay, are needed to further inform treatment recommendations.
Footnotes
Acknowledgements
Thanks go to the staff of the Mycobacterium Reference Laboratory, VIDRL, especially Caroline Lavender, for technical assistance, and the many veterinarians and veterinary pathologists who contributed case material and other assistance to this study, especially Laura Brandt, Bronwyn Smits, Catherine Harvey, Rob Fairley, Richard McCoy and Sergio Sanchez Picado of Gribbles Pathology, and Adrienne French, Catherine Williamson, dawn Seddon, Geoff orbell and Cathy Harvey of New Zealand Veterinary Pathology.
Date accepted: 7 March 2017
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported in part by a grant from the Feline Health Research Fund. Carolyn o’Brien was supported by an Australian Government Research Training Program Scholarship. Richard Malik was supported by the Valentine Charlton Bequest administered by the Centre for Veterinary Education, The University of Sydney.