
Abstract
Objectives
This study aimed to compare the under-and-over technique, a type of intracapsular treatment, and the standard fabella–tibial suture, a method for extracapsular treatment, in achieving immediate, postoperative stifle stability after cranial cruciate ligament (CrCL) rupture by using a feline, custom-made limb-press model.
Methods
Cadaveric feline hindlimb specimens (n = 14) were positioned in the limb press at predefined joint angles (stifle joint: 120°; hock joint: 120°), and vertical loads of 5%, 10%, 20% and 30% body weight were applied statically. Mediolateral radiographic views were obtained of the stifles under each load before and after CrCL transection, as well as after treatment with either of the two surgical techniques, and differences in distance between two predefined radiographic points for each radiograph were analysed.
Results
The general linear model showed a significant effect of load (P <0.01) and technique (P = 0.004) and a significant interaction between load and technique (P = 0.006) regarding craniocaudal stifle stability. Distances between predefined tibial and femoral reference points were consistently higher in transected CrCLs than in intact stifles. All standard fabella–tibial suture-treated stifles (n = 7) were stable at all loads tested. Of the seven under-and-over technique-treated stifles, one was unstable at 20% body weight load and three at 30% body weight load.
Conclusions and relevance
Our model, which appropriately reproduced certain aspects of domestic shorthair cat stifle mechanics, indicated that a 40 lb monofilament nylon prosthesis, tightened at 20 N, produces more favourable biomechanical stabilisation of craniocaudal cruciate-related stifle instability than a 0.5 cm wide strip of fascia lata applied intracapsularly.
Introduction
Cranial cruciate ligament (CrCL) rupture in dogs is mainly degenerative, 1 but recent histological evidence indicates that the pathogenesis of injury in cats is different. 2 Although conservative management yields acceptable clinical function in cats, 3 the non-surgical treatments have a higher prevalence of secondary meniscal injuries,4,5 decreased range of motion, muscle fibre atrophy and progression of degenerative joint disease. 3 Canine studies have shown that prolonged stifle instability promotes progression of osteoarthritis,6,7 and that surgically treated cruciate patients experience less pain, faster recovery and better functional results. 8 A plethora of surgical techniques are available for both cats and dogs, including extracapsular sutures,1,4,6,9 intracapsular techniques, 10 cranial closing wedge, tibial plateau levelling osteotomy (TPLO), 11 tibial tuberosity advancement (TTA) 12 and modified Maquet technique. 13
The biomechanical effects of TTA and TPLO have been evaluated in cats,14,15 using a downsized limb press derived from the canine model by Warzee et al. 16 Both studies evaluated the femorotibial shear force by measuring cranial tibial subluxation. Radiographic assessment of feline cadaveric specimens before and after CrCL transection reflected hindlimbs standing at predefined angles while bearing a load of 30% body weight (BW). Postoperative assessments in both studies showed that applying standards of correction in TTA or TPLO may lead to unresolved femorotibial instability in feline patients. However, techniques other than corrective osteotomies are more widely used in cats in everyday practice.
According to canine force plate analyses, extracapsular stabilisation produces similar limb function to TPLO but superior function compared with intracapsular stabilisation at 6 months postoperatively. 17 Mölsä et al found similar results but questioned the use of ground reaction forces as a sole assessment measurement for postoperative limb function. 18 Feline CrCL injury pattern and anatomy differ from canines and, therefore, findings may not be generalisable, highlighting the need for feline-specific studies of the biomechanic-related influences of treatment modality on feline stifles.1,2,19
This study was designed to, first, describe a custom-made limb-press model for cats and, second, to assess direct, postoperative stifle stability produced by two commonly used surgical treatments: under-and-over technique and standard fabella-tibial suture. We hypothesised that an extracapsular nylon suture is superior in neutralising excessive cranial tibial thrust caused by CrCL injuries compared with an intra-articular prosthesis of fascia lata.
Materials and methods
Limb press
A canine limb press was modified for feline use.20,21 Like the original, equally sized rectangular base and top plates were adjoined by four columns affixed at each corner of the base plate (90° angles) and milled holes in the top plate, which allowed the top plate to slide up and down, in a parallel manner (Figure 1). Four fixation screws allowed the top plate to be secured in a certain position (Figure 1). A lockable mount held a copper tube, that the specimen’s femoral shaft had been moulded into using polymethyl methacrylate, at an unchangeable 60° angle to the top plate, mimicking the hip joint. A radiographic plate was attached to the back side of the base plate, parallel to the sagittal plane of the limb. To adapt the original to feline use, the model as described was first downsized to fit domestic shorthair cats. A gap was milled through the top plate to reduce weight, and a mount for the force gauge (Sauter FA-100; Sauter GmbH) was installed to facilitate monitoring the tension of the straight patellar ligament while tightening the rest of the mechanism. A scale (WPT 30F1/K [Radwag Wagi Elektroniczne], scale range: maximum 30 kg; accuracy: d = 1 g) was mounted underneath the base plate to measure directly the weight applied to the cadaveric limb (Figure 1). The ability to compensate for friction loss of applied weight to the sliding top plate, by measuring the load at the bottom, improved precision and promoted reproducibility. Furthermore, measurements under loads <30% BW were possible without needing to reduce the weight of the top-plate beyond stability.
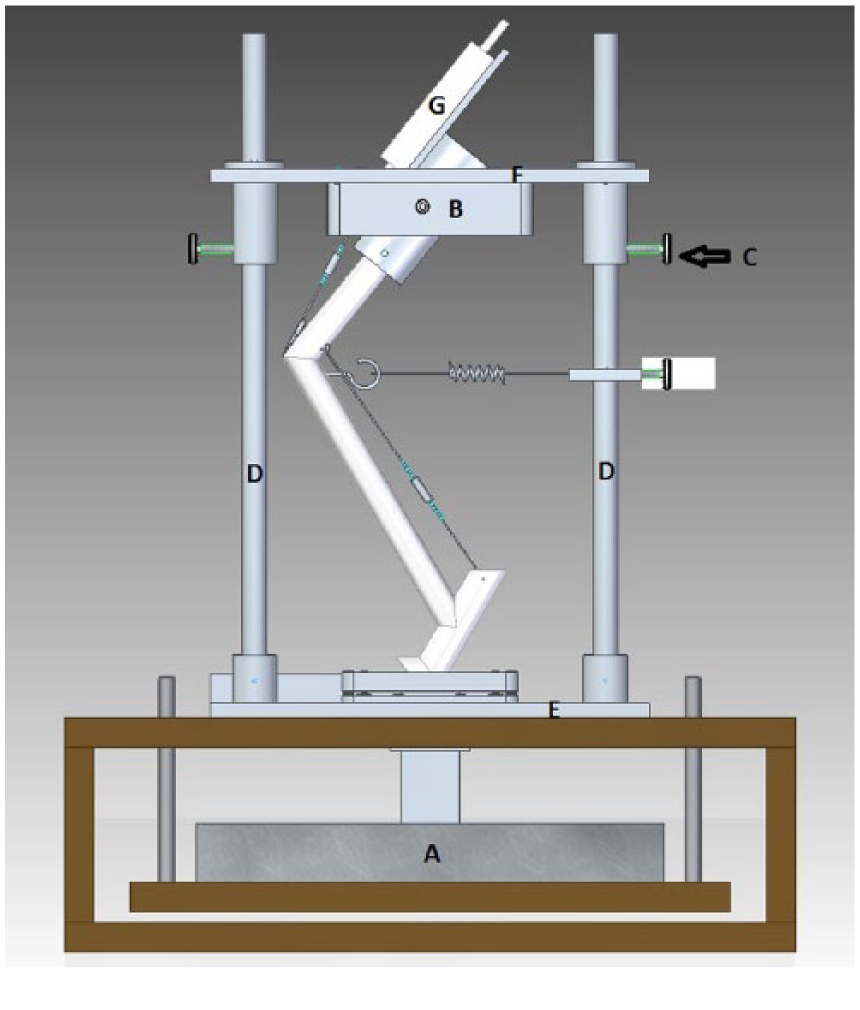
Frontal view of the limb-press model, facilitating a lateral view of the limb. A = scale measuring load transduced; B = femoral mount on top plate; C = fixation screw to lock position of the top-plate; D = columns; E = base plate; F = top plate; G = force gauge to measure patellar tendon force
Limb preparation
Cadaveric hindlimbs (n = 14) from seven domestic shorthair cats (four males, three females; all neutered), euthanased for reasons unrelated to this study, were harvested after recording age (mean ± SD 5.57 ± 1.91 years; range: 3–8 years), BW (mean ± SD 3.62 ± 0.62 kg; range: 2.9–4.2 kg) and tibial plateau angle (TPA, from mediolateral radiographs, 22 mean ± SD 22.63 ± 1.89°; range: 20.12–25.9°).
Specimens were free of stifle pathology, as determined by direct observation and radiography. Excess soft tissues were removed, from the femoral head to the proximal aspect of the metatarsus, but care was taken to preserve the stifle and talocrural joint capsules, patellar tendon, collateral ligaments and the strip of fascia lata that is required to perform the under-and-over technique. All specimens were wrapped in saline (0.9% NaCl)-soaked towels and stored at −20 °C until testing. Limbs were labelled and assigned to the two treatment groups by drawing lots; if one limb of a cadaver was in the first group, the contralateral limb had to be in the second.
Before testing, limbs were thawed at room temperature. Soft tissues were kept moist during the experiment by repeated spraying with isotonic saline solution. A cable was inserted through a drill hole in the centre of the proximal patella and connected to the force gauge with a turnbuckle to simulate the quadriceps mechanism. Another cable was placed through a hole manually centred in the proximal one-third of the calcaneus, and connected to two 2.0 mm cortical bone screws (Securos) placed at the level of the medial and lateral fabellae, with an interposed turnbuckle to simulate the Achilles tendon mechanism. An eye-hook was inserted through a drill hole manually into the caudal tibia, 0.5 cm distal to the joint surface, and connected to a spring-mechanism to remove slack (see Figure 2). 21

Photograph of the limb press with a specimen in position. Stifle and hock were angulated at 120° of flexion. A radiographic plate was fixed at the back of the model and a radiographic magnification marker (*) positioned at the level of the bones, parallel to the detector-plate. S = spring mechanism
Mechanical testing
First, a patellar tendon load (PTL) value was determined for each specimen and load, to be replicated during all of the following evaluations. All 14 specimens were tested before (group 1) and after (group 2) CrCL transection. The repair specimens (group 3) were split into two subgroups for under-and-over technique treatment (group 3a) and standard fabella-tibial suture (group 3b) (see Figure 3).

Flow diagram of mechanical testing. Patellor tendon load (PTL) was evaluated in the beginning and used in all groups tested to standardise load. Distance between X1 and X2 was measured in intact stifles (Ds), stifles with transected cranial cruciate ligaments (CrCls) (Dt) and two repair subgroups, treated with intracapsular technique (Di) or extracapsular suture (De)
PTL values
All left limbs (n = 7) were inserted into the limb press as described, 21 with stifle and talocrural angles of 120 ± 5°. 14 A small K-wire was used to secure the position of the paw on its rest. Angulation of the stifle and talocrural joint was adjusted by tuning the turnbuckles and subsequent radiographic validation. The top-plate fixation screws were loosened and a single static vertical load was applied via the top plate until 5%, 10%, 20% and 30% BW were displayed by the scale underneath the socket holding the paw. PTL, read off the force gauge instantly, was recorded and quadruplicate measurements were calculated as a mean, for each cadaver and load, and rounded to a whole number for application to all subsequent groups, thereby ensuring the same PTL was used for the left and right specimen derived from the same cadaver.
Group 1: ‘intact stifles’
Each specimen (n = 14) was mounted onto the limb press with specified joint flexion angle (hip: 60°; stifle: 120±5°; tarsus: 120±5°).14,15 Fixation screws at the top-plate were fixed to inhibit upward or downward movement of the top plate. Turnbuckles were tightened to achieve the median PTL predetermined for each specimen, and load was applied until the force-plate measured the proper ground reaction force reflecting 5%, 10%, 20% and 30% BW. A radiographic magnification marker (Biomedtrix) was positioned at specimen level and parallel to the radiographic plate (Figure 2). Radiographs (Gierth TR 90/20 Battery, X-ray tube; Toshiba D-0814) were taken and immediately developed digitally (Kodak Point-of-Care CR 260). Joint angles were measured using a proprietary DICOM viewer (dicomPACS view, version 5.2.11). The stifle angle was evaluated by crossing the femoral diaphyseal axis with the tibial functional axis. 23 Because most of the femoral diaphysis was not visible, the caudal contour of the metal pipe holding the femur was used instead. The tarsal angle was evaluated by crossing the functional axis of the tibia with an axis of the tarso-metatarsus, 23 defined by a line parallel to the longitudinal axes of the metatarsal bones three and four. If angles of the stifle or hock on the images exceeded the predefined 120 ± 5°, specimens were repositioned and measurements were repeated.
Group 2: ‘transected CrCL’
Group 1 limbs (n = 14) were removed from the limb press, CrCLs were transected with a #11 blade, and the lateral arthrotomy was closed via interrupted sutures (2-0 polypropylene, PROLENE; Ethicon). After remounting onto the limb press, radiographs were repeated using the previous loads (Figure 4).

Radiograph of a right stifle, loaded at 30% body weight after cranial cruciate ligament transection. KBR = Kreuzbandruptur (cranial cruciate rupture); BW = body weight
Group 3: ‘repair’
Group 2 limbs (n = 14) were removed from the limb press and subgrouped (groups 3a and 3b, n = 7 in each).
Group 3a underwent the under-and-over treatment.24,25 A 0.5 cm wide strip of fascia lata was freed from the thigh laterally but left attached distally. The graft was then passed under the intermeniscal ligament, through the joint and over the top of the condyle–fabellar region laterally. The graft was tightened with the stifle flexed at 100° until cranial drawer was eliminated and then sutured to the fascia, periosteum and lateral collateral ligament. The graft was secured using single interrupted sutures of 2-0 nylon, 25 rather than the originally described spiked washer and screw fixation to avoid interference with landmarks during evaluation of the radiographs. 24
Group 3b underwent standard fabella–tibial suture treatment using a 40 lb monofilament nylon, #40 stainless steel crimp clamp and a Power X crimping device (all from Securos). The nylon was looped around the femorofabellar ligament and through a tibial bone tunnel drilled at the defined point T2 (cranial to the proximal aspect of the extensor groove) 26 from proximal to distal on the lateral surface of the tibia. Then, the crimps were secured after tightening the nylon suture at 20 N with the previously mentioned force gauge while maintaining a stifle joint-angle of 100°. 27
Treated limbs were remounted onto the limb press and radiographs were repeated under the previous loads.
Measurements
After the acquisition of each radiograph, points X1 and X2 were defined by the same assessor using the DICOM viewer (Figure 5). X1 was defined as the cranial edge of the tibial plateau. X2 was defined as the centre of a circle (r = 6 mm) that was superimposed over the caudal contour of the femoral condyles. If a double condyle sign was present, the distance was measured at its widest. If this distance was >1 mm, the specimen had to be repositioned and measurements repeated. Distances of X1–X2 (D) and the distance between the upper edges of the metal beats of the magnification markers were determined; the latter served to compensate for the radiographic magnification effect when all measured distances were divided by the actual magnification factor for a given radiograph. The magnification factor was calculated by dividing the measured distance of the marker’s metal beats on the radiographs by their actual distance of 100 mm.

Magnified projection of Figure 4
Displacement of ‘intact’ group 1 (Ds) and ‘transected’ group 2 (Dt), that is, Dt–Ds, indicated the gain of passive femorotibial instability caused by loss of CrCL restraint. The differences between Ds and the D measurements of the subgroups, that is, Di–Ds for the ‘intracapsular’ subgroup 3a and De–Ds for the ‘extracapsular’ subgroup 3b, indicated the remaining femorotibial instability after the respective treatment. A difference of 0 indicated re-establishment of the original status; differences exceeding 2 mm were considered to indicate instability.
Statistical analysis
Descriptive statistics were calculated for all measured distances using IBM SPSS version 19. The effect of the two surgical techniques on the calculated between-load differences (described above) was analysed using general linear modelling (GLM) for repeated measurements. One-sample t-tests were performed to evaluate the impact of each technique on these differences for each load. Correlation of BW and TPA with the differences between De–Ds and Di–Ds, respectively, and Dt–Ds were calculated using Pearson’s correlation coefficient. Normal distribution was determined by Kolmogorov–Smirnov test. A P value <0.05 indicated significance.
Results
Dt was consistently significantly greater than the corresponding Ds, as reflected by a positive difference for Dt–Ds (Table 1); this difference also increased with higher loads.
Descriptive statistics for all measured distances
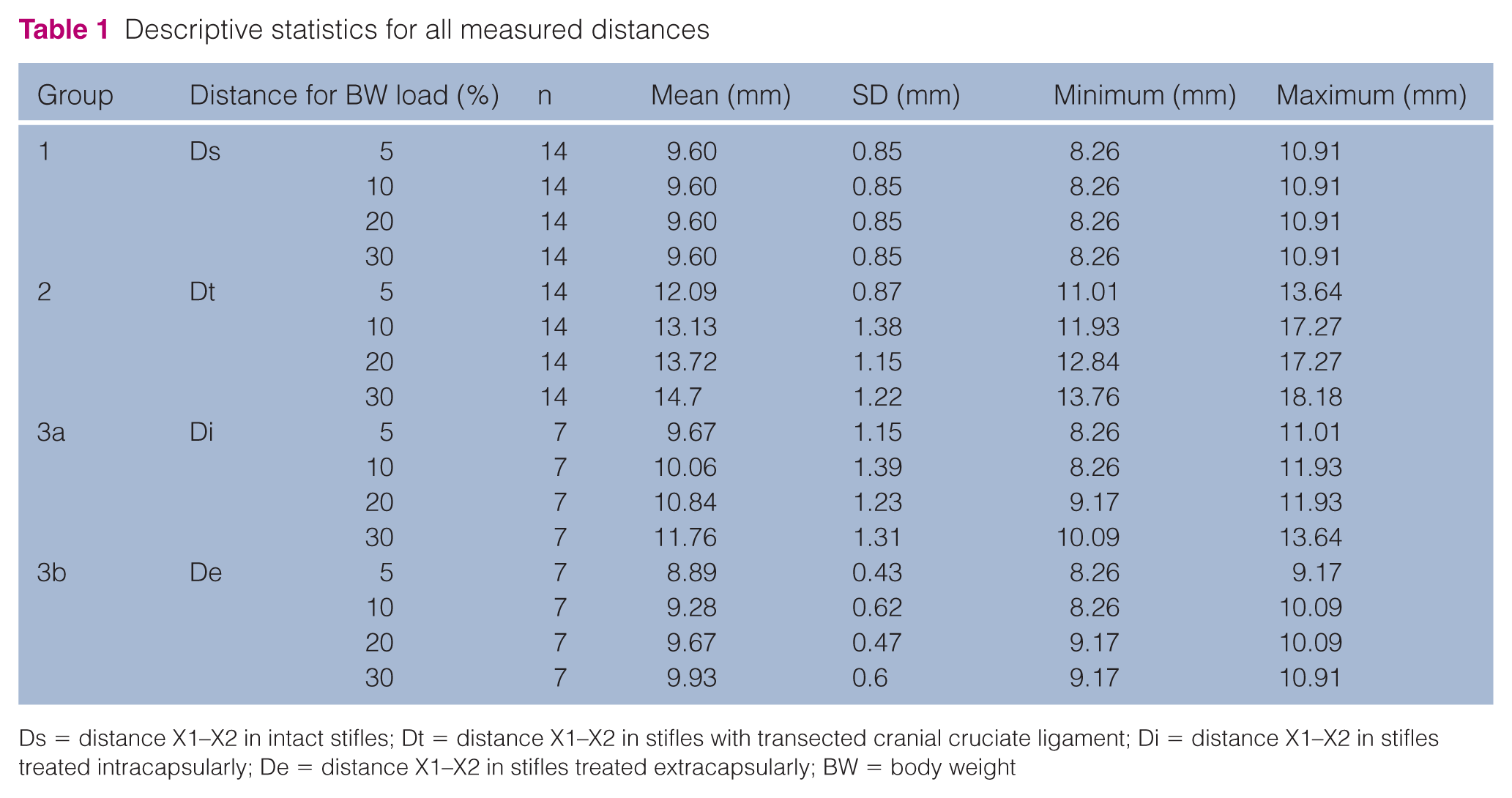
Ds = distance X1–X2 in intact stifles; Dt = distance X1–X2 in stifles with transected cranial cruciate ligament; Di = distance X1–X2 in stifles treated intracapsularly; De = distance X1–X2 in stifles treated extracapsularly; BW = body weight
Mean De values were consistently significantly lower than Di at all corresponding loads. GLM showed a significant effect of load (F = 37.6; P <0.01) and technique (F = 12.4; P = 0.004) on the distances (D) and a significant interaction between load and technique (F = 4.9, P = 0.006). For subgroup 3a, one-sample t-tests showed significant differences from the test value 0 with 20 and 30% BW loads. For subgroup 3b, a significant difference occurred at 5% BW load (Figure 6 and Table 2).

Diagram comparing intra- (subgroup 3a) and extracapsular (subgroup 3b) D-values with intact stifles (dotted zero-line) at measured loads. Di = distance X1–X2 in stifles treated intracapsularly; De = distance X1–X2 in stifles treated extracapsularly; Ds = distance X1–X2 in intact stifles
Calculated differences for each load
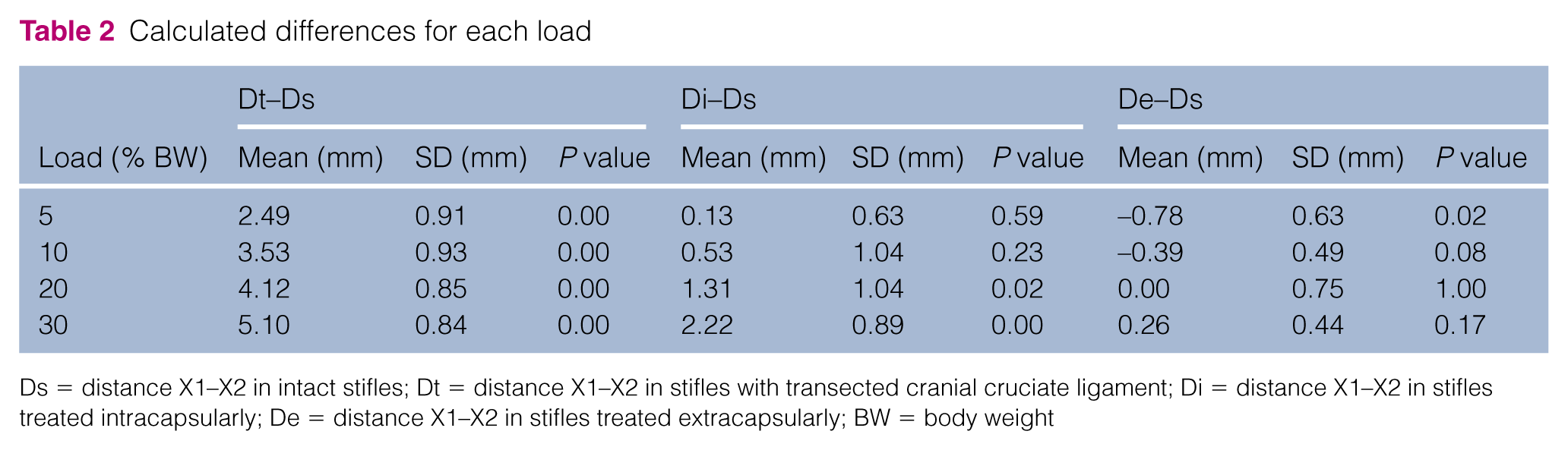
Ds = distance X1–X2 in intact stifles; Dt = distance X1–X2 in stifles with transected cranial cruciate ligament; Di = distance X1–X2 in stifles treated intracapsularly; De = distance X1–X2 in stifles treated extracapsularly; BW = body weight
Pearson’s correlations coefficients of BW and the displacement Di–Ds and De–Ds ranged from r = 0.276 to r = 0.754 for subgroup 3a and from r = −0.2 to r = 0.295 for subgroup 3b. These correlations were not significant at any load, except for that between BW and the Di–Ds difference at a load of 10% BW (P = 0.05). Correlation of BW and TPA ranged from r = −0.441 to r = 0.72 for subgroup 3b and from r = −0.192 to r = −0.659 for subgroup 3a; neither showed significant correlations at any load.
Discussion
Our experimental model confirmed the hypothesis that an extracapsular nylon prosthesis is superior in restricting cranial tibial drawer movement in the CrCL-deficient feline stifle joint compared with the fascia lata graft. Lack of craniocaudal restraint provided by the CrCL results in craniocaudal instability in the affected limb(s) upon weight carrying, 10 which was reproduced in our feline modified limb-press model. Assuming that postoperative D values higher than Ds + 2 mm reflect instability, all CrCL-transected stifles were unstable at all measured loads exceeding 5% BW. We also showed that the cranial drawer increased as greater weight was applied. All extracapsular suture-treated stifles were stable at all tested loads. One intracapsular-treated stifle was unstable at 20% BW load and three at 30% BW load.
Although in vitro models cannot completely reproduce in vivo joint mechanics, limb-press models more adequately reflect nature than the classic load-mounting sets, 27 as the former incorporate other joints and aim to mimic the influence of quadriceps muscle and Achilles tendon. Certainly, in vivo video data (via fluoroscopy) of live cats walking on treadmills, as reported in dogs, 28 would be useful in studying feline stifle mechanics. In our experience, untrained cats do not comply with treadmills. They try to jump off as soon as the treadmill starts to move, refuse to walk a straight line and lower their body centre by flexing their limb joints so that the acquired data do not represent a natural gait on solid ground. Because of this we generated the in vitro model.
Downsizing the canine limb press proved very technically challenging. Friction caused by the aluminium top plate sliding along the columns greatly influenced the discrepancy between weight added to the top plate and the vertical force created by this weight. However, the top plates’ own heavy weight precluded application of 5–20% BW when free sliding; thus, we inserted the scale underneath the specimens’ paws. Also, measuring the applied force at the limb-press bottom via a scale added precision to the vertical force, which could then be dosed by manipulating the four screws securing the top plate. These features are unique in the veterinary literature, and key to limb-press applicability to, and its accuracy for, feline samples.
It is important to acknowledge involvement of muscular structures (eg, hamstring) as they can antagonise the cranial tibial thrust.23,29 As we have removed them from the specimens, this represents a limitation of the model. In our pre-study, excessive PTL led to immediately lower D values. Thus, we defined the PTL values for every cadaver and load prior to the experimental measurements to get comparability between left and right limbs of the same cadaver.
We selected crimping as the nylon line fixation method to maximise reproducibility as crimped nylon loops tend to elongate less than knotted sutures under tension.30–33 A 40 lb monofilament nylon was chosen because it was the thinnest nylon applicable to commercially available crimps. While there is no definitive recommendation for tensile strength of monofilament nylon to treat CrCL-deficient feline stifles, adequate monofilament leader lines should at least withstand the patient’s BW. 34 Veterinary Instrumentation’s step-by-step guidelines advise 10–15 kg BW dogs to be treated with 50 lb monofilament leader lines; 35 as the heaviest cat in our study weighed 4.2 kg, we deemed the 40 lb tensile strength to be acceptable.
No study has previously reported data from feline limb-press testing at 30% BW, or repeated measurements for 5%, 10% and 20% values. We aimed to illustrate how craniocaudal draw on cranial cruciate ligament repair increases up to the well-established 30% BW. 0% BW was technically impossible, as any scale-to-paw contact resulted in loads >0. Therefore, 5% BW served as a reliable compromise for a low value; 10% and 20% increments were selected randomly and did not reflect any specific weight-bearing situations. Tightening the standard fabella–tibial suture at 20 N created a significant overcorrection (Figure 6 and Table 2) 27 by expressing a De below Ds at 5% BW load, but cranial drawer was successfully neutralised at all weights tested. Subgroup 3a did not show an overcorrection of cranial drawer, but failed to counteract cranial tibial translation at 30% BW load, depicting load at normal walking.
Sterilisation technique and cyclic loading exert strong influence on prosthetic nylon strand elongation.31,36 Elongation by cyclic loading may negate the observed advantage. However, our model was not designed for testing the medium- to long-term effects of this phenomenon, which needs to be acknowledged as a significant limitation of the study. Moreover, the effects of rotational stifle instability (by measuring craniocaudal radiographic projections) were not evaluated. Superimposition of the spring mechanism’s metal components would complicate radiographic evaluation, and therefore craniocaudal projections were not included in our study design.
Furthermore, freezing and thawing the specimens, as well as repetitive loading of the same specimen, could have significant influence on the tensile strength of investigated soft tissue. This is a clear limitation to our study, as well as the fact that securing the fascia lata strip using sutures instead of screws and washers could have compromised the results of group 3a in creating more slack.
The limb-press system described herein was incapable of testing high loads as they would be experienced when a cat jumps. Experimentally, we ‘overloaded’ cadaver limbs in a pre-test situation and recognised collapse due to cable breakage or slippage through the fixation crimps. Applying excessive force to specimens may also stretch important soft tissue structures, generating bias in repetitive measures for different configurations; we advise investigating such supposition in pre-tests before attempting to reproduce our study at higher loads.
Another limitation of this study exists because radiographs were just measured by one observer. Also blinding was not possible, because radiopaque crimps clearly marked radiographs of subgroup 3b.
Conclusions
Our model reproduced certain aspects of post-CrCL injury stifle mechanics in domestic shorthair cats. A 40 lb monofilament nylon, tightened at 20 N, produced favourable biomechanical stabilisation of cruciate-related stifle instability directly after surgery. Compared with an intracapsularly applied 0.5 cm wide strip of fascia lata, the standard fabella–tibial suture created an overcorrection of cranial drawer at loads <20% BW but counteracted cranial draw much better at loads reflecting normal walking. Furthermore, the implementation of scale placement at the base of the limb press and predefining PTL values are key elements for adapting these models to feline specimens.
Footnotes
Acknowledgements
Alexander Tichy (Platform Bioinformatics and Biostatistics, University of Veterinary Medicine, Vienna, Austria) for assistance with statistical analysis; Anton Fuchs (Section Sensor Technology, Graz University of Technology, Graz, Austria) and Alexander Volk (Department of Physics, Graz University of Technology, Graz, Austria) for technical support in planning and adapting the limb press; and Harald Marchhart (Roentgenpartner Med Vertriebs- u Service GmbH, Melk, Austria) for supplying radiography equipment for the mechanical testing phase, free of charge.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.