
Abstract
Objectives
The purpose of this study was to solicit and compile data from practicing veterinary specialists regarding their use of toceranib in cats with mast cell neoplasia and to provide initial assessment of possible clinical benefit and adverse events.
Methods
The American College of Veterinary Internal Medicine and Oncology listservs were used to solicit data pertaining to cases in which toceranib was used in the treatment of feline mast cell neoplasia. Cases were included if the following data were received: signalment (age, sex, breed), diagnosis of mast cell neoplasia by either cytology or histopathology, anatomic classification of disease (cutaneous, splenic/hepatic, gastrointestinal, other), previous and concurrent treatment, toceranib dose (mg/kg) and schedule, duration of therapy, best response and documentation of adverse events.
Results
Case data from 50 cats with cutaneous (n = 22), splenic/hepatic (visceral) (n = 10), gastrointestinal (n = 17) or other (n = 1) mast cell neoplasia were received. Clinical benefit was seen in 80% (40/50), including 86% (19/22) with cutaneous, 80% (8/10) with visceral and 76% (13/17) with gastrointestinal involvement. A majority of cats (n = 35) received glucocorticoids during toceranib treatment. Median duration of treatment in cats experiencing clinical benefit was 36 weeks (range 4–106 weeks), 48 weeks (range 12–199 weeks) and 23 weeks (range 13-81 weeks) for cutaneous, visceral and gastrointestinal cases, respectively. Toceranib was administered at a median dose of 2.5 mg/kg (range 1.6–3.5 mg/kg); in 90% (45/50) the drug was given three times per week. Treatment was generally well tolerated with 60% (30/50) of cats experiencing adverse events. The majority of these events were low-grade (grade 1 or 2) gastrointestinal or hematologic events that resolved with treatment break and/or dose adjustment.
Conclusions and relevance
Toceranib appears to be well tolerated in feline patients with mast cell neoplasia. Biologic activity of this drug is evident in the studied cats; however, further prospective studies are needed to elucidate fully its role in treatment of this disease.
Introduction
Feline mast cell neoplasia can encompass several different clinical presentations, including cutaneous, splenic or gastrointestinal primary sites. Cutaneous mast cell tumors (MCTs) are the second most common cutaneous neoplasm in cats. 1 Typically, they have a benign behavior and cats are generally well when they are presented for evaluation. Survival times for cutaneous MCTs are prolonged, and even incompletely excised tumors may not recur. 2 In contrast, cats with splenic (the most common cause of splenic disease in the cat) or intestinal MCTs are often ill at presentation, and clinical staging may reveal involvement of the liver, abdominal lymph nodes and bone marrow. 3 Especially for those cats with intestinal MCT, survival times are often short.4–6
Surgery is generally recommended for feline MCTs, where amenable. In the case of splenic MCTs, this recommendation may be made despite heavy metastatic burden. 6 However, adjunctive therapy for this disease is poorly understood, and there is currently no standard for postoperative recommendations in feline MCTs of any type. Anecdotally, various cytotoxic chemotherapy agents have been utilized, popular among them vinblastine, chlorambucil and lomustine (CCNU). Retrospectively, lomustine was assessed to be well tolerated, with evidence of biologic activity in both cutaneous and extracutaneous feline MCTs. 7 However, in another report, various chemotherapeutic agents were utilized without apparent survival benefit over untreated cats. 3 To improve local control, radiation therapy of previously excised cutaneous MCTs has shown promise. In two reports, cutaneous MCTs treated with strontium-90 irradiation demonstrated median survival times >900 days.8,9 However, these studies were small, and further investigation of cytotoxic chemotherapy and radiation therapy in feline MCTs is needed.
Small-molecule inhibitors have been of recent interest in the treatment of feline MCTs. One target of particular interest is KIT, a proto-oncogene encoding the receptor tyrosine kinase (RTK) c-Kit. Mutations resulting in c-Kit’s independence from its ligand stem cell factor and resultant constitutive activation are important in tumorigenesis in some canine MCTs, which, when carrying such mutations, behave more aggressively and carry a poorer prognosis than those MCTs without these mutations. 10 Several studies describe KIT mutations in feline MCTs with prevalence ranging from 56% to 85% of samples.11–13 Cats showing gain-of-function mutations in c-Kit in either cutaneous or visceral MCTs have subsequently demonstrated positive responses to treatment with imatinib mesylate (Gleevec; Novartis), a tyrosine kinase inhibitor (TKI).12,14 Despite the rarity of mast cell neoplasia in humans, a gain-of-function mutation in c-Kit in human systemic mastocytosis has been reported; the affected person responded dramatically to imatinib. 15 Dasitinib (Sprycel; Bristol-Myers Squibb), midostaurin and nilotinib (Tasigna; Novartis), TKIs in development or use in human oncology, have shown in vitro, dose-dependent growth inhibition of feline MCT lines. 16 Masitinib mesylate (Kinavet; AB Science), a TKI marketed for veterinary use, previously held conditional Food and Drug Administration (FDA) approval for treatment of non-resectable grade II and III canine MCTs. 17 While masitinib may be safe to give to healthy cats, 18 and has been anecdotally utilized in treatment of feline MCTs, adequate evidence of efficacy was not demonstrated in dogs with MCTs during the conditional licensing period; consequently, masitinib is no longer available for use in the USA. Masitinib is approved for use under the trade name Masivet (AB Science) in the European Union, where its label indications are for treatment of non-resectable grade II or III canine MCTs with confirmed mutated c-Kit tyrosine kinase receptor. 19
Toceranib phosphate (Palladia; Zoetis) is a TKI that inhibits signaling at c-Kit, as well as a variety of other RTKs in the split kinase family, such as vascular endothelial growth factor receptor, platelet-derived growth factor receptor and Flt-3. 20 This promiscuity results in both direct antitumor and antiangiogenic effects in a variety of solid neoplasms of the dog. 21 Toceranib is FDA-approved for treatment of canine MCTs, and those tumors with constitutively activating mutations in c-Kit demonstrate a greater response rate than canine MCTs without such mutations. 22 Given the high prevalence of KIT mutations in feline MCTs, toceranib is an attractive drug for use in this population, albeit it is not labeled for use in the cat. While recent literature has evaluated toceranib use in feline oral squamous cell carcinoma and feline injection site sarcoma, to our knowledge there have been no published studies evaluating toceranib in the treatment of feline MCTs.23–25 The purpose of this study was to solicit and compile data from practicing veterinary specialists regarding their use of toceranib in cats with mast cell neoplasia and to provide initial assessment of possible clinical benefit and adverse events (AEs).
Materials and methods
Case selection and response to therapy
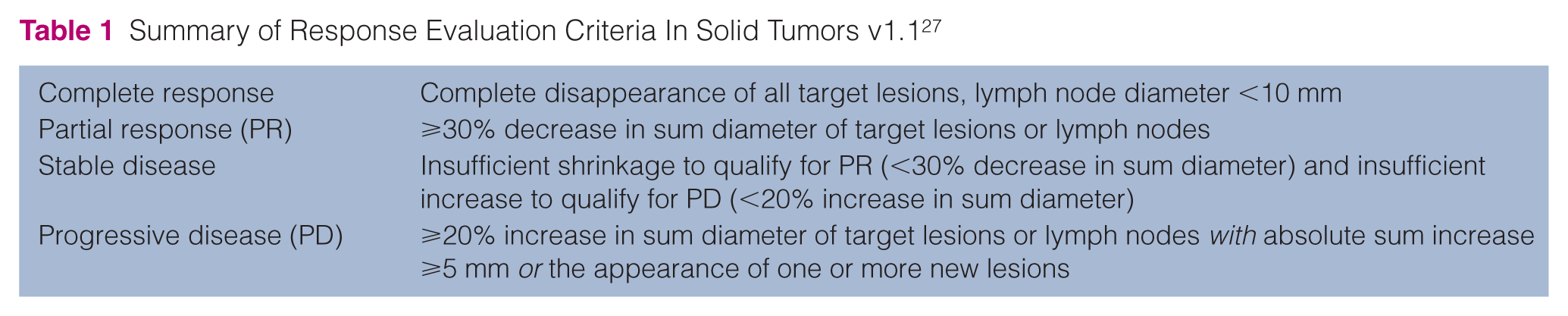
This study was performed as a multicenter retrospective analysis. The American College of Veterinary Internal Medicine Oncology and Small Animal Internal Medicine listservs were used to solicit cases in which clinicians had treated feline mast cell neoplasia with toceranib. To be eligible for analysis, the following case data were required: signalment (age, sex, breed), pathologist-confirmed diagnosis of MCTs by either cytology or histopathology, anatomic classification of disease (cutaneous, splenic/hepatic, gastrointestinal, other sites), previous and concurrent treatment, toceranib dose (mg/kg) and schedule, duration of therapy, best response and documentation of AEs (toxicity). Cats were excluded if these data were not available, or if they were treated with concurrent cytotoxic chemotherapy other than glucocorticoids, or with concurrent radiation therapy. AEs were reported by the attending clinician according to the Veterinary Cooperative Oncology Group Common Terminology Criteria for Adverse Events v1.1 (VCOG-CTCAE v1.1). 26 Primary AE category (gastrointestinal/constitutional, hematologic or metabolic) was defined by highest VCOG grade. Individual responses were defined by the attending clinician using the Response Evaluation Criteria for Solid Tumors (RECIST v1.1) (Table 1). 27 Best response to toceranib could be categorized as a complete response (CR), a partial response (PR), stable disease (SD) at least 10 weeks in duration, SD <10 weeks in duration or progressive disease (PD). As in previous publications describing the use of toceranib in dogs, clinical benefit (CB) was determined by best response to therapy and was defined as a CR or PR of any duration, or SD at least 10 weeks’ duration.21,22 Animals experiencing SD <10 weeks in duration or PD as their best response to toceranib did not achieve CB.
Summary of Response Evaluation Criteria In Solid Tumors v1.1 27
Data analysis
While data were primarily descriptive in nature, limited statistical analysis was performed. The variables of disease location (cutaneous, visceral, gastrointestinal), previous use of possibly cytoreductive medical treatment (glucocorticoids, chemotherapy or TKIs, radiation therapy) and concurrent use of glucocorticoids were examined to determine their influence on the probability of experiencing CB, best response experienced and treatment duration (weeks). Duration and response variables were analyzed using the Kruskal–Wallis test. The CB variable was analyzed using a logistic procedure. A P value <0.05 was considered statistically significant (SAS version 9.4).
Results
Demographic information, diagnosis and prior treatment
Fifty cases complied from 10 sites had sufficient data for inclusion in the analysis. Cats were primarily domestic breeds (n = 45); case data for Siamese cats (n = 3) and Maine Coon cats (n = 2) were also received. Thirty castrated male cats and 20 spayed female cats were evaluated.
Diagnosis of MCTs was made in 21 cats by cytology and in 29 cats by histopathology. Cats were stratified based upon anatomic classification of disease: cutaneous tumors only, splenic and/or hepatic (visceral) involvement, any gastrointestinal involvement or other sites. This resulted in categorization of 22 cases of cutaneous MCTs, 10 cases of visceral MCTs, 17 cases of gastrointestinal MCTs and one case involving a different site (nasopharyngeal).
Treatment prior to toceranib was diverse and is summarized in Tables 2 and 3. Fourteen cats (28%) did not receive any therapy for their MCT prior to receiving toceranib, while the remaining 36 cats received a variety of therapies at the discretion of their attending clinician. Consequently, time between MCT diagnosis and initiation of toceranib therapy varied widely (median 7 weeks, range 1–260 weeks). Of the three cats treated with other TKIs (masitinib [n = 2], imatinib [n = 1]) prior to toceranib, two of these cats experienced progressive disease and were switched to toceranib. The third cat experienced suspected masitinib toxicity (vomiting) and its owner had difficulty administering this medication daily. The cat was consequently switched to toceranib given three times weekly.
Cytoreductive treatment of studied cats prior to toceranib therapy
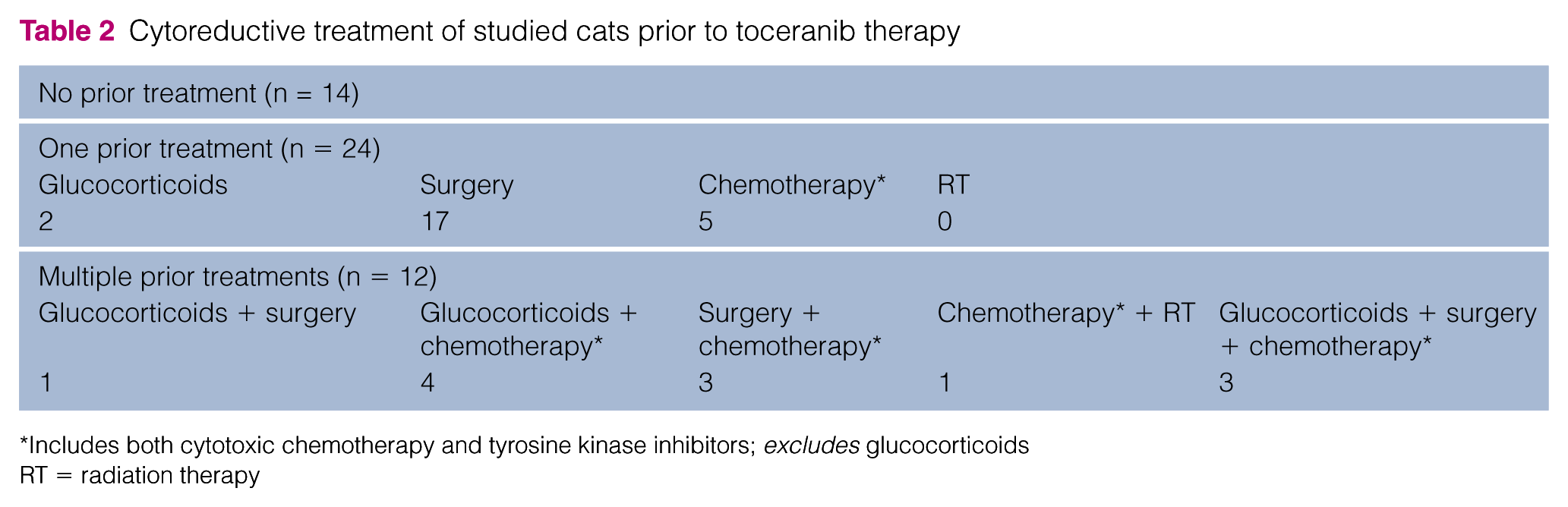
Includes both cytotoxic chemotherapy and tyrosine kinase inhibitors; excludes glucocorticoids
RT = radiation therapy
Antineoplastic agents utilized prior to toceranib therapy (total cats exposed to prior chemotherapy = 16)*
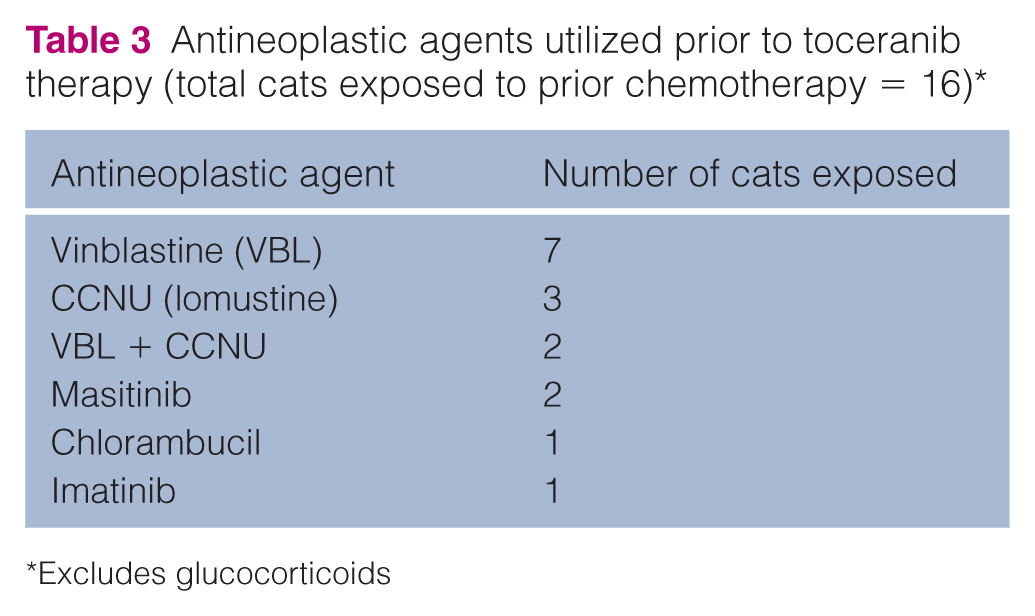
Excludes glucocorticoids
Toceranib treatment
Toceranib was administered orally to studied cats at a median dose of 2.5 mg/kg (range 1.6–3.5 mg/kg). Nearly all cats (90%; 45/50) received the drug three times per week. The remaining cats received toceranib every other day. A majority of cats (70%; 35/50) received concurrent glucocorticoid therapy, either daily (n = 12) or every other day (n = 23).
CB was observed in 80% (40/50) cats, including 86% (19/22) cats with cutaneous (seven CR, 10 PR, two SD), 80% (8/10) with visceral (three CR, four PR, one SD) and 76% (13/17) cats with gastrointestinal (three CR, eight PR, two SD) involvement; full response data are given in Table 4. Median response duration in cats experiencing CB was 32 weeks (range 5–199 weeks), with cutaneous disease responding for a median of 29 weeks (range 5–96 weeks), visceral disease responding for a median of 46 weeks (range 12–199 weeks) and gastrointestinal disease responding for a median of 24 weeks (range 8–84 weeks). Six cats experiencing CB were still responding to toceranib at the time of data submission. Median duration of treatment in cats experiencing CB was 36 weeks (range 4–106 weeks), 48 weeks (range 12–199 weeks) and 23 weeks (range 13–81 weeks) for cutaneous, visceral and gastrointestinal cases, respectively. Results of the statistical analysis are summarized in Table 5; no statistical significance was found.
Best response to toceranib therapy in studied cats

Based upon Response Evaluation Criteria for Solid Tumors criteria 27
Includes both splenic and hepatic mast cell tumors; excludes any cat with gastrointestinal involvement
This cat had a nasopharyngeal tumor
P values after statistical analysis*

A P value <0.05 was considered significant
Includes both splenic and hepatic mast cell tumors; excludes any cat with gastrointestinal involvement
Includes glucocorticoids, cytotoxic chemotherapy, tyrosine kinase inhibitors and radiation therapy
CB = clinical benefit; GI = gastrointestinal; MCT = mast cell tumor
AEs and case outcomes
Thirty studied cats (60%) experienced 82 possible AEs. Of these 30 cats, 23 (77%) experienced two or fewer AEs, while seven (23%) experienced more than two AEs. The majority of AEs (71/82; 87%) were low-grade (grade 1 or 2) gastrointestinal or hematologic events. Full AE profiles are summarized in Table 6.
Summary of reported adverse events observed in cats receiving toceranib

BUN = blood urea nitrogen; ALT = alanine aminotransferase; ALP = alkaline phosphatase
In particular, rare increases in alanine aminotransferase (ALT) and alkaline phosphatase (ALP) activities were noted. Five cats (three with cutaneous MCTs, two with gastrointestinal MCTs) experienced increases in either ALT (n = 4) or ALP (n = 1) activity. A summary of the characteristics of these cats is presented in Table 7. All affected cats experienced CB (two CR, two PR, one SD) during treatment.
Summary of changes in liver enzyme activity during toceranib treatment

EOD = every other day; ALT = alanine aminotransferase; G = glipizide; M = methimazol; S = steroid (glucocorticoid); MWF = Monday, Wednesday and Friday; ALP = alkaline phosphatase
In 20/30 cats experiencing AEs, dose adjustment was performed at the discretion of the attending clinician. In four cats, toceranib therapy was discontinued owing to suspected toxicity. Highest VCOG grade AEs for these four cats were grade 2 lethargy, vomiting, diarrhea and inappetence; grade 2 lethargy and inappetence; grade 2 anemia; and grade 4 increased ALP activity.
Severe AEs (grade 4 or 5) were reported in five cats. Three grade 4 AEs were reported, all involving increases in either ALT or ALP activity. ALT and ALP values were normal in these cats at toceranib initiation; however, no cat was symptomatic or required treatment for increased enzyme activity. In two cats with visceral MCTs, grade 5 AEs were reported. One cat, age 14 years at toceranib therapy initiation, experienced grade 5 increased creatinine (5.2mg/dl, reference interval [RI] 0.8–2.1). This cat received toceranib for 149 weeks. Another cat experienced grade 5 anemia (packed cell volume 8%; RI 30–45). Neither of these events were suspected to be related to toceranib administration.
At the time of data submission, 21 cats were still alive while 23 cats had died. Of these 23 cats, 19 died or were humanely euthanized as a result of their MCTs. For the remaining four cats, documented unrelated causes were chronic kidney disease (n = 2), aortic thromboembolism (n = 1) and hypertrophic cardiomyopathy (n = 1). Cats whose cause of death was not described were assumed to have died of their MCTs. Six cats were reported lost to follow-up by their attending clinician.
Discussion
The aim of this retrospective study was to assess MCTs-bearing cats receiving toceranib phosphate for possible clinical benefit and toxicity. While the retrospective nature of this study precludes direct comparison of response rates to other treatments reported elsewhere, perhaps more limiting is the paucity of literature pertaining to medical therapy for feline MCTs. A single retrospective report in which CCNU (lomustine) was utilized as either primary or adjunctive therapy for cutaneous and extracutaneous MCTs revealed an overall response rate of 50% with a median response duration of 168 days (24 weeks). 7 The results reported in this study are similar in median response duration (224 days; 32 weeks) with overall CB of 80%. A previously discussed case report describing treatment of a single cat with feline MCTs with imatinib revealed a response after 5 weeks of treatment with complete regression of cutaneous masses and significant reduction in mastocytemia. 14 In another small cohort of cats with feline MCTs treated with imatinib, 7/8 cats achieved an objective response (six partial remissions and one complete remission). 12 In a report of 36 cats undergoing splenectomy for MCTs, no survival benefit was noted in 22 cats receiving various postoperative chemotherapy protocols over cats not receiving chemotherapy; however, no cat in that study received a TKI. 28
In this study population, toceranib administration was well tolerated. While 60% of cats experienced AEs, the majority were mild (grade 1 or 2) hematologic or gastrointestinal events and did not necessitate toceranib discontinuation. This AE profile is similar to that described in dogs treated with toceranib at commonly prescribed dosages. 29 Vomiting and inappetence were two of the most frequently observed AEs in studied cats, and may have contributed to concurrent weight loss in these animals. Increased gastric acid secretion secondary to MCTs may also play a role, as observed in dogs, although its true significance is unknown in cats. 30 In addition, many cats in this study were treated with gastroprotective medications and histamine antagonists, which may confound these results. Five severe (grade 4 or 5) AEs were noted. Three grade 4 AEs were noted, including two grade 4 increases in ALT activity and one grade 4 increase in ALP activity. No cat had an abnormal ALT or ALP value before beginning toceranib; however, no cat was symptomatic for its increase in enzymatic activity, and no cat required treatment. Two grade 5 AEs were also noted. The cat who experienced a grade 5 increase in creatinine had no evidence of kidney dysfunction before starting toceranib. However, while toceranib administration cannot be eliminated as a cause of the reported grade 5 increase in creatinine, based upon the natural progression of kidney values, it was suspected this increase was due to chronic kidney disease, unrelated to tocernib administration. The cat experiencing grade 5 anemia was reported by the attending clinician to have suffered suspected hemorrhage caused by progressive MCTs. Toceranib use was not suspected as a cause of this AE but cannot be ruled out.
There have been several recent publications regarding the use of toceranib in cats, and a summary of selected findings is presented in Table 8. Of note in these publications are increases in ALT and ALP activities in a small but consistent number of cats within these study groups. Grade 4 increased ALT activity has also been noted in a single cat receiving imatinib at the lowest dose administered to the cats in that study. 33 In dogs, increases in ALT activity have been reported in approximately 21% of those receiving toceranib; however, few suffer increases of grade 3 or 4. 22 It has been demonstrated that toceranib excretion is hepatic in dogs, and it is possible that cats share a similar elimination mechanism. 34 Whether these uncommon liver enzyme activity changes are due to cumulative exposure or idiosyncratic reaction is unknown. Here, five cats experienced increases in either ALT (n = 4) or ALP (n = 1) activity (see Table 7). Glucocorticoid use was noted in three of the affected cats; however, it has not been associated with inducible increases in ALT or ALP activities in cats, as is common in dogs. Given the wide range of treatment durations, it would appear that an idiosyncratic reaction may be a more likely explanation, but all studied groups were small and routine restaging was not performed; therefore, increased enzyme activities related to metastatic disease cannot be eliminated. The majority of affected cats were also treated with methimazole, and either drug effects or poorly controlled hyperthyroidism cannot be excluded as causes of these increases. Furthermore, one affected cat was treated with glipizide, which has been associated with rare increases in liver enzyme activity. 35 As recommended in recent literature, periodic liver enzyme assessment should be pursued in further studies in which cats are administered toceranib. 32
Recent data regarding the use of toceranib in cats and specific adverse events (AEs)

NA = not applicable; MCT = mast cell tumor; SCC = squamous cell carcinoma; GI = gastrointestinal; ALT = alanine aminotransferase; VCOG = Veterinary Cooperative Oncology Group; ALP = alkaline phosphatase
As with all retrospective studies, this analysis was subject to several limitations. Given the way data were solicited, recall bias could result in preferential recall of cats who experienced a response to toceranib, resulting in a falsely increased rate of CB. While toceranib was almost always administered at or below the maximum tolerated dose described for dogs of 3.25 mg/kg (one cat received 3.5 mg/kg every other day), no standard dose or administration schedule was utilized. Based upon case data, cats were administered whole tablets only, using one, or in a few cases, two 10 mg or 15 mg tablet(s). These limited tablet sizes make precise dosing of cats difficult, and likely is the cause of the wide dosing range. While the rise of compounding pharmacies makes compounded toceranib readily available, the stability and efficacy of these products is unknown, and splitting of tablets is not recommended. 36 Concurrent use of glucocorticoid and supportive medication was also allowed. This study did not specifically evaluate single-agent glucocorticoid efficacy, and published literature regarding glucocortoid use in feline MCTs is extremely scarce.3,7–9,28,37 Additional controlled studies are needed to resolve the specific role of glucocorticoids in the treatment of feline MCTs. While attempts to standardize AE reporting and response by utilizing objective parameters (VCOG and RECIST criteria, respectively) were made, retrospective analysis of medical records makes either misinterpretation or simple lack of data possible. Finally, the relatively small sample size of this study could have contributed to lack of statistical significance. However, despite these limitations, the response rate and demonstrated tolerability in this study in cutaneous, visceral and gastrointestinal feline MCTs merits consideration of toceranib in the treatment of this disease.
Conclusions
Toceranib was well tolerated in this study population, with preliminary indication of biologic activity in feline mast cell neoplasia. Additional evaluation in prospective studies is needed to describe fully its role in the treatment of this condition.
Footnotes
Acknowledgements
The authors wish to acknowledge Dr Chong Wang and Ju Ji (Iowa State University) for their assistance in statistical analysis, and Dr Austin Viall for his assistance in manuscript editing. They also wish to acknowledge Dr Chelsea Tripp, Dr Theresa Arteaga, Dr Martin Crawford-Jakubiak, Dr Ana Rita Serras, Dr Sarah Gillings, Dr Christine Swanson, Dr Shawna Greene, Dr Michelle Pressel and Dr Kelly O’Neill for their case contributions to this study.
Conflict of interest
CMJ is a former employee of Pfizer Animal Health and serves as a member of the Zoetis (formerly Pfizer Animal Health) Oncology Advisory Board and occasionally receives honoraria for these activities. The remaining authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded by Iowa State University College of Veterinary Medicine – Oncology Section.