
Abstract
Clinical summary:
A 13-year-old, spayed Devon Rex with unilateral digital flexor musculotendinous contracture of the forelimb was treated by surgical tenotomy. The condition improved transiently, but recurred rapidly and became bilateral. Histopathologic analysis of necropsy tissues resulted in a morphologic diagnosis of fibromyositis of the antebrachial muscles causing contracture and flexural deformity of the carpi and phalanges of both thoracic limbs. A search for similar cases yielded the clinical notes of a second cat, a 10-year-old, spayed Devon Rex, also with bilateral disease. This second case responded well to surgical tenotomy but tissue biopsies were not obtained to permit microscopic assessment of the underlying pathologic process.
Relevance and novel information:
Acquired and permanent contracture of the digital flexor muscles and/or tendons of the forelimbs is a rare and poorly described condition of cats. The very limited number of documented cases describing disease affecting one or more digits (but not the carpus) infers a causal link with onychectomy, but reported histopathologic changes have been limited to the tendons. The two cases described in this report suffered contracture of the carpus and all digits bilaterally, one without previous onychectomy and the other 9 years after onychectomy. There were novel histopathologic findings in the muscles of the one case for which biopsy material was available. Information gained from these two cases provides a new perspective for the investigation and treatment of future cases. Specifically, consideration should be given to an underlying immune-mediated myopathic process and a possible genetic predisposition in the Devon Rex breed. Currently, the poorly understood etiopathogenesis hinders our ability to definitively recommend treatment options, which might include corticosteroids and other forms of immunosuppressive therapy.
Introduction
Acquired permanent flexural deformity of the distal forelimbs of cats as a result of muscle and/or tendon contracture has been rarely reported in the feline literature. To the authors’ knowledge there are only two reports (encompassing a total of five cases) describing similar clinical presentations,1,2 and theories concerning etiopathogenesis are tenuous. The two previous reports describe digital flexor tendon contracture due to a presumptive traumatic etiology, most often onychectomy, although all potential associations are circumstantial.1,2 There is one well documented report of superficial digital flexor contracture in a dog. 3 The treatment approach for this broad group of cases has been surgical tenotomy1,2 which, based on experiences to date, has potential to be successful.
The purpose of this report is to describe two cases of digital flexor musculotendinous contracture in Devon Rex cats, one with novel histopathologic findings. These cases provide a unique foundation from which future case investigation and treatment trials may be instigated.
Case descriptions
Case 1
A 13-year-old, 3.4 kg, female spayed Devon Rex was presented to Wilston Vet, Brisbane, Australia with a 1 week history of progressive flexural deformity of the phalanges of the right thoracic limb, resulting in lameness and weightbearing on the dorsal aspect of the phalanges. There was no antecedent history of trauma. Physical examination revealed taut flexor muscle tendons between the carpus and distal phalanges. The claws of the affected limb could not be retracted into their sheaths. There was no evidence of pain, thickening or swelling of any structures of the forelimb, or of spontaneous muscle contraction, such as fasciculations. The remaining three limbs appeared normal and a full clinical examination revealed a systolic heart murmur (grade 1/6) as the only other abnormality. Clinical pathology was not performed.
Radiologic assessment of the affected limb revealed mild subluxation of the carpal bones, presumed to be secondary to increased tension in the soft tissues traversing the joint. The carpus, metacarpophalangeal and proximal interphalangeal joints of digits II–V, and the metacarpophalangeal joint of digit I were fixed in flexion. Radiographic interpretation may have been affected by positioning limitations. No additional abnormalities could be appreciated.
The case was referred to Queensland Veterinary Specialists, Brisbane. The severity of contracture had increased and a diagnosis of contracture of the deep digital flexor muscle and/or tendon was made. Involvement of other muscles and/or tendons of flexion was suspected also. Deep general anesthesia did not result in any relief of the tension over the affected joints. Tenotomy of the five branches of the deep digital flexor tendon proximal to the metacarpal pad was performed. Postoperatively, the phalanges were maintained in a weightbearing position with an L-shaped splint for 13 days. Within 2 days of splint removal, the cat was using the limb normally on soft surfaces.
The condition recurred 2 months later, and the muscles attached to the accessory carpal bone (flexor carpi ulnaris and ulnaris lateralis) also appeared to have undergone contracture, resulting in carpal abduction and further flexion. A second tenotomy with more intensive aftercare using physiotherapy was recommended but declined by the owners.
Eight months after initial presentation, the left forelimb became similarly affected. The flexion had become so severe bilaterally that the cat’s nails had become embedded in the digital pads. The cat progressively became less able and willing to walk, being forced to bear weight on the dorsal aspects of the carpi bilaterally. Meloxicam (0.1 mg/kg q24h PO) provided pain relief but no improvement in the patient’s morphologic presentation. Eleven months after initial presentation the cat was euthanased on humane grounds and a necropsy was performed.
No gross abnormalities could be appreciated in the thoracic or abdominal cavities. Euthanasia did not result in relaxation of the contracture (Figure 1). Radiographs of the forelimbs were repeated, with similar results to 11 months prior, although the degree of flexion was more severe (Figure 2). The flexor carpi ulnaris, flexor carpi radialis, deep digital flexor and superficial digital flexor muscles and tendons were isolated from the left forelimb and removed at their points of insertion. These tissues were fixed in neutral buffered formalin, paraffin embedded, cut at 5 µm and stained using haematoxylin and eosin (H&E), trichrome, periodic acid Schiff and oil red O. H&E-stained slides (from a total of 15 blocks from skeletal muscles with attached tendons) were examined by one of the authors (RP).
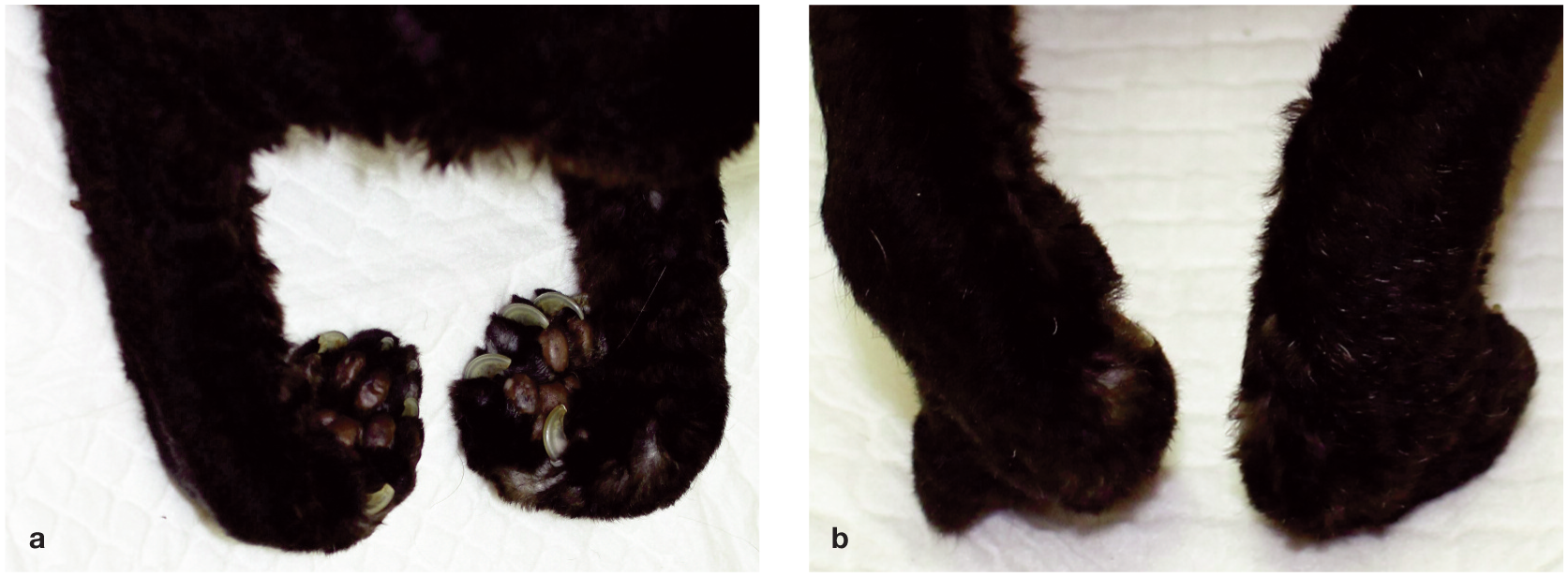
Bilateral digital and carpal flexion (a) and abduction (b) in case 1 (images taken at necropsy after euthanasia)
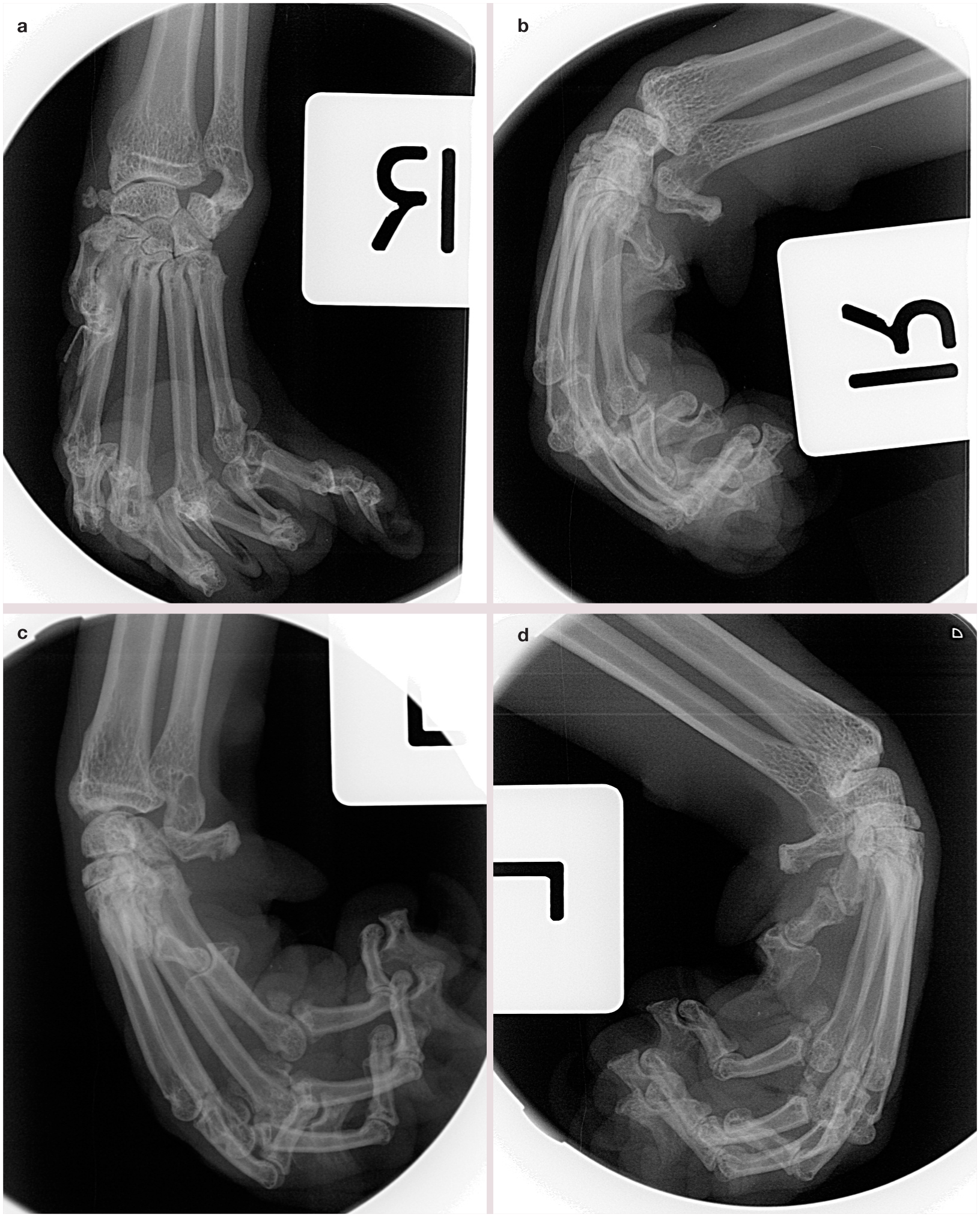
Radiographs of the forelimbs of case 1 at necropsy: (a) right dorsopalmar view; (b) right lateral view; (c) left dorsolateral–palmaromedial view; (d) left lateral view
Histologically, focal lymphoplasmacytic infiltrates were visualized in the endomysium (Figure 3a) and beneath the perimysium (Figure 3b) of all muscles. There was evidence of excessive proliferation of spindle cells in these zones, presumably originating from primitive endomyseal fibroblasts and myosatellite cells. Both of these infiltrates appeared to invade and dissect degenerative skeletal muscle fibers, resulting in their atrophy and replacement (Figure 3c). There were also relatively lower numbers of lymphoid cells in the face of abortive attempts by skeletal muscle fibers to repair the damage (Figure 3d). Lastly, there were focal areas of fibrous tissue replacement of fusiform areas of muscle tissue immediately beneath the perimysium, indicating possible scar tissue. The tendons were normal, as were the nerves. The final morphologic diagnosis was fibromyositis of the antebrachial muscles of flexion, causing contracture and flexural deformity of the carpi and phalanges of both thoracic limbs.
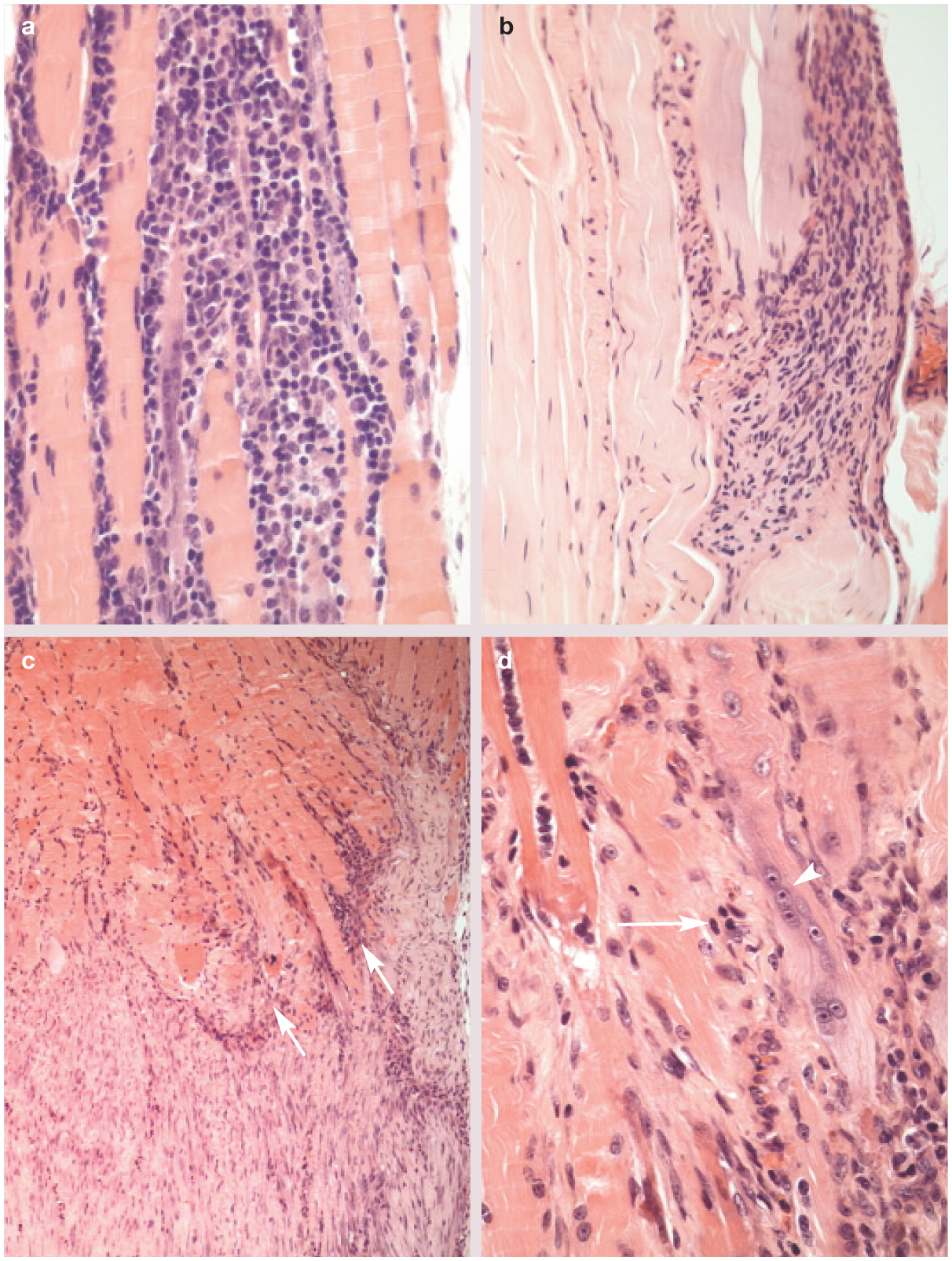
Photomicrographs of muscle biopsy specimens of case 1. (a) Lymphoplasmacytic infiltrate dissects between atrophic skeletal muscle fibers. (b) Lymphoplasmacytic infiltrate present beneath the perimysium. (c) Skeletal muscle fibers (above) separated from fibrous tissue replacement (below) by a lymphoplasmacytic infiltrate (arrows). (d) Junction of inflammatory cell infiltrate with border of skeletal muscle fibers, demonstrating muscle fiber degeneration, abortive attempt at muscle fiber repair (arrow) and fibrosis (arrowhead)
Case 2
A 10-year-old, 3.0 kg, female spayed Devon Rex was presented to the All Cats Hospital in Largo, Florida, USA with a left thoracic limb lameness and permanent flexion of the fifth digit. Bilateral thoracic limb onychectomy had been performed 9 years previously. A diagnosis of osteoarthritis of the fifth metacarpophalangeal joint was made based on radiographic findings and the cat was prescribed oral meloxicam (0.1 mg/kg q24h PO for 3 days, then tapering to 0.025 mg/kg q48h PO [Metacam; Boehringer Ingelheim] intermittently over a 5 month period).
The cat re-presented 5 months later with bilateral carpal and digital flexion, and was experiencing great difficulty in walking. Attempts at extending the digits caused the patient discomfort. Systolic blood pressure determinations, hematology and a six enzyme biochemistry analysis were unremarkable. Neither intra-articular (site not specified) methylprednisolone acetate (6 mg, once) nor acupuncture proved beneficial.
The cat was referred to The Veterinary Medical Center at the University of Florida 18 months after initial presentation. Bilateral carpal flexion with abduction of both paws was noted (Figure 4). Physical examination (including a detailed neurologic examination) and routine bloodwork were unremarkable apart from the aforementioned findings. Cytologic examination of joint fluid was unremarkable. Radiographs of the thoracic limbs revealed marked degenerative changes and subluxation affecting both carpi. Lytic lesions were noted within the bone, and peri-articular proliferative changes were consistent with an enthesopathy. A diagnosis was made of flexural deformity of the right carpus and manus, with displacement of the proximal row of carpal bones.

Bilateral carpal and digital flexion in case 2
A bilateral flexor tenotomy was performed 20 months after initial presentation. A fiberglass splint was applied postoperatively and replaced weekly for a month. At follow- up examination the cat walked well, but hyperextension of the carpal and metacarpophalangeal joints was evident bilaterally (Figure 5), and pain was exhibited during manual extension of the joints. Twelve weeks postsurgery, pain on manipulation had resolved but bilateral lameness was noted, presumably as a result of weightbearing on the distal metacarpal bones proximal to the metacarpal pads. Arthrodesis was offered to normalise the posture, but declined by the owners. The patient survived another 4 years and was noted to have bilateral carpal hyperextension at each visit. It was euthanased for an unrelated illness.

(a,b) Postoperative hyperextension in case 2
Discussion
The two cases described in this report exhibit a similar morphologic presentation of digital flexor muscle and/or tendon contracture. A literature search revealed only two reports describing a total of five cases with some similarities to the present two cases.1,2 Without exception, the seven cases demonstrated an acquired rather than a congenital disease and all affected extremities were those of the thoracic limbs. To make a claim that all seven affected cats were suffering from the same ‘syndrome’ is not possible due to the small sample size, limited data available and many uncontrolled variables. Nevertheless, it is interesting to compare and contrast them despite the fact that we cannot prove they are linked in a consistent fashion (Table 1).

Digits of the thoracic limb in each case. MN = castrated male; FN = spayed female; DSH = domestic shorthair
A search of the Veterinary Information Network database revealed 21 additional cases, which were variably well documented. Information concerning these cases is summarised as supplementary material.
Muscles and tendons affected
It was apparent from the physical, radiographic and histopathologic findings of case 1 that multiple muscles of carpal and digital flexion (see box) were affected, including the flexor carpi radialis, flexor carpi ulnaris and the superficial and deep digital flexor muscles. Histology demonstrated that the tendons were not involved. Case 2 was possibly similarly affected, based on the physical and radiographic findings, but muscle and tendon biopsy and histology was not performed.


Distal aspect of flexor tendon anatomy on a third thoracic digit (distal digital annular ligament has been removed). * = Deep digital flexor tendon; P1 = proximal phalanx; P2 = middle phalanx; P3 = distal phalanx; + = superficial digital flexor tendon. Reproduced, with permission, from Cabon et al 2
In two of three cases previously described by Cabon and colleagues, one digit only was affected, leading to the proposition that the abnormal pathologic process was limited to a point distal to the division of the common deep and superficial digital flexor tendons. 2 The remaining case displayed bilateral digital involvement, although digit I was not described as being affected, implying that only the superficial digital flexor tendon was affected. In the two patients described by Cooper and colleagues, involvement was bilateral and encompassed all digits but not the carpi, suggesting that the predominantly affected site was the deep and/or superficial digital flexor tendons or the muscles giving rise to them. 1 Therefore, the present case 1 is unique compared with all previously reported cases, at least anatomically, and case 2 may likewise be unique.
Possible pathomechanism and etiology
The relationship between previous onychectomy and this disease entity is an interesting point of comparison. Case 1 is distinct in that bilateral disease in a cat that has not undergone onychectomy has not been described previously. Case 2 had undergone onychectomy 9 years previously, suggesting that the relationship between the surgery and disease might not be cogent. Cooper and collaborators infer a direct link between onychectomy and the onset of signs in both of their cases, supported by a temporal relationship of only 6–12 weeks and the histologic findings of granulation tissue surrounding the distal tendons in one patient. Cabon and colleagues also considered a similar pathomechanism for two of their three cases, which was supported by tendon histology in one case. However, the temporal delay between surgery and the onset of clinical signs (3.5 and 6.5 years) and the lack of onychectomy in the remaining case is not consistent. Indeed, it would be fair to question whether the associated histologic findings were coincidental (ie, onychectomy may not have anything to do with causation of the syndrome). Muscle biopsy was not performed in any of the cases and therefore an underlying myopathic process cannot be excluded, especially in those cats with all digits affected.
Given the inflammation of skeletal muscle evident in case 1, both traumatic and non-traumatic causation should be considered. Traumatic injury to a muscle can result in compartment syndrome, whereby the increased pressure within the confines of the muscle sheath results in ischaemic damage. Necrosis leads to reparative fibrosis and contracture, placing tension on the associated tendons, sometimes sufficiently severe to cause physical deformity. Similarly, tearing of the muscle belly or tendon due to sudden high impact forces heals by replacement with fibrous scar tissue, which may give rise to contracture. Neither of the cases in this report were known to have experienced non-surgical trauma, although acute or chronic repetitive strains of these tendons should be considered, possibly attributable to regular jumping down from a height onto hard surfaces.
The pathologic feature of lymphoplasmacytic myopathic inflammation in case 1 is actually more consistent with an immune-mediated process. Although most autoimmune diseases are ‘idiopathic’, they may be triggered by infectious agents. Toxoplasma gondii myositis is a well known clinical entity, although usually seen as part of a disseminated disease process. Bacterial myositis is very common given the high prevalence of cat fight wounds. However, the characteristic histologic features of polymicrobial anaerobic infection are neutrophilic inflammation, necrosis and subsequent healing with fibrosis; to the authors’ knowledge, none have been reported to cause contracture of muscles or permanent deformity. No microbial pathogens were observed in case 1, but they can be missed – especially if the culprit is a ‘stealth pathogen’ like Bartonella species and was present transiently. 5 There are no reports to date of a feline viral myositis, although one prospective study of feline immunodeficiency virus (FIV) infection noted inflammatory changes in skeletal muscles. 6 The FIV status of the cats in this report was unknown. Degenerative joint disease or other forms of arthritis can affect the conformation of the joint and was considered a component of the clinical symptomatology in case 2. Denervation atrophy may also result in deformity, but histological evidence of this was likewise lacking in case 1.
Consideration of the group of disorders broadly described as fibrotic myopathies may be relevant, as some are associated with inflammation and replacement of myofibers with dense fibrous connective tissue. All are characterized by a relative shortening of a muscle belly resulting in permanent contracture.7,8 In cats, one case of brachialis muscle contracture 7 and another involving the semitendinosus muscle 8 have been reported. It is possible that similarities exist between these entities and the cases reported here.
The three cases described by Cabon and collaborators were in Siamese and Siamese-cross cats, prompting those authors to propose a possible genetic predisposition in this breed. 2 The fact that both of the present cases, as well as one described by Cooper and colleagues, 1 were Devon Rex cats may be purely coincidental, but again raises the spectre of a genetic predisposition.
Management of future cases
Until now, cases of digital flexor musculotendinous contracture in the forelimbs of cats have been diagnosed by physical findings, a relative lack of other significant radiographic changes, occasionally a temporal association with onychectomy, and tendon biopsy at the time of surgical treatment. This report provides a valid case for additional diagnostic studies, of which muscle and tendon biopsy are of paramount importance. Prior to surgery, needle electromyography may be useful; so too serum creatine kinase activity determinations and antinuclear antibody testing. Magnetic resonance imaging would provide exquisite definition of the changes present in the muscles and tendons, and high-resolution ultrasound studies would likely also provide useful extra information. If future cases present in specific breeds, such as Siamese, Devon Rex or their crosses, investigation into a genetic link may be worthwhile.
While non-steroidal anti-inflammatory therapy failed to improve the morphologic presentation of previously documented cases,1,2 or those in this report, we can anticipate the condition is painful (despite difficulties measuring pain in the patients). Therefore, some form of analgesia is warranted. The presence of lymphoplasmacytic myositis in case 1 suggests treatment trials with immunosuppressive doses of corticosteroids and/or ciclosporin may be worth considering prior to surgical interventions. However, assuming that immune-mediated myositis precedes contracture and fibrosis by a variable (and possibly lengthy) period of time, the best opportunity for treatment could be during the subclinical phase of disease, which is likely to be prior to presentation.
The current treatment modality for deep and/or superficial flexor contracture is tenotomy or tenectomy of the affected branches of the tendons, with case 2 in this report and all previously documented cases having responded well.1,2 Case 1, however, suffered a rapid recurrence postoperatively, the reason for which is unknown. Despite this, the evidence to date suggests that surgery remains the most reliable treatment option (with biopsy performed intraoperatively) until more is known about this unique disease in cats.
Conclusions
Digital flexor musculotendinous contracture in the forelimbs of cats remains a rare and perplexing condition, perhaps reflecting a spectrum of disease processes. The novel histopathologic observation of fibromyositis in case 1 opens the door for scrutiny of future cases for an immune-mediated myopathic process. However, previous theories implicating trauma such as onychectomy should still be considered, while a genetic component is also worthy of further investigation using the power of genomics. Archiving of DNA from affected cats, particularly in Devon Rex and Siamese lineages, is to be encouraged. Further investigation is also required to determine if this is a single disease entity or a collection of cases more broadly described as a syndrome with various potential etiologies.
Surgical treatment by tenotomy or tenectomy will probably remain the mainstay of therapy but all future cases should undergo biopsy of all affected muscles and tendons at the time of surgery. Trial immunosuppressive therapy might be appropriate in selected cases, particularly when owners decline surgical intervention.
Supplemental Material
Supplemental Material
Summary of data acquired from the Veterinary information Network concerning 23 cases of feline digital flexor musculotendinous contracture
Footnotes
Acknowledgements
The authors thank Jeanine Sandy of Queensland Medical Laboratory Pathology, Australia and Professor Beth Valentine of the College of Veterinary Medicine, Oregon State University, USA for their opinions regarding the histopathology of case 1. Jason Beck of Queensland Veterinary Specialists, Brisbane, Queensland, Australia performed the surgical treatment of case 1, and Deborah Edwards of All Cats Hospital, Largo, Florida, USA was the consulting clinician who provided the records for case 2. The clinicians at Wilston Vet, Brisbane, Queensland, Australia are thanked for their insights and provision of time and resources in enabling LT to investigate this syndrome. RM is supported by the Valentine Charlton Bequest of the Centre for Veterinary Education of the University of Sydney, Australia.
Supplementary material
Summary of data acquired from the Veterinary Information Network concerning 23 cases of feline digital flexor musculotendinous contracture.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article. Laboratory costs for case 1 were generously covered by the management of Wilston Vet.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Date accepted: 6 October 2016
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.