
Abstract
Objectives
There is a distinct subset of lesions arising on the digits of cats, located at or close to the nail-bed epithelium, which are typically composed of proliferative fibroblast-like cells, multinucleate giant cells and areas of osseous metaplasia, but currently there is no published literature detailing the clinical or histological features of these lesions.
Methods
This study identified 41 such cases from two large commercial diagnostic laboratories and assessed various histological and clinical features; 22 cases had additional follow-up data available.
Results
All masses in this study were exophytic, variably inflamed, contained large numbers of spindle cells and had areas of capillary formation. The majority also had areas of ulceration, multinucleate giant cells and osseous metaplasia. The mitotic count was variable, but mitoses were confined to the fibroblast-like cells. Male cats appeared predisposed and the second digit was the most commonly affected.
Conclusions and relevance
These distinctive lesions arising on the digits of cats had potential for local recurrence but metastasis was not reported. Based on these clinical and histological features, the masses in this study appear most similar to giant cell reparative granulomas, and trauma, injury to the nail or nail-bed and nail-bed infections may potentially contribute to their development.
Introduction
Masses arising on the digits of cats can be either reactive or neoplastic and because these typically have similar clinical presentations but different outcomes, biopsy of the mass or amputation of the affected digit followed by histopathological assessment is often required to reach a diagnosis and prognosis. Depending on the gross features present, potential differential diagnoses might include a primary inflammatory process (including various infectious diseases), a traumatic injury, a primary neoplasm such as soft tissue sarcomas or squamous cell carcinoma, or digital metastasis of a pulmonary adenocarcinoma.
Experience in feline clinical practice and diagnostic pathology laboratories suggests that there is a distinct subset of lesions arising on the digits of cats, typically located at or close to the nail-bed epithelium, which present as exophytic and often ulcerated masses. On histological assessment these lesions typically show proliferative fibroblast-like or spindle cells, multinucleate giant cells (MNGCs) and areas of osseous metaplasia. Despite this unique presentation and histomorphology, there is currently no published literature detailing the clinical or histological features of these lesions. This study identified such cases from two large commercial diagnostic laboratories, one in the UK and the other in New Zealand, obtained additional clinical information and follow-up where available, and reviewed the histological features of each mass. This enabled the behaviour of these distinctive digital lesions and their clinical outcome to be determined and the pathognomonic histological features to be identified.
Materials and methods
Records from two commercial diagnostic laboratories (Finn Pathologists, Diss, UK, and New Zealand Veterinary Pathology Ltd, Palmerston North, New Zealand) were searched for potential cases diagnosed from fixed tissue samples, based on combinations of key words such as ‘feline’, ‘toe’, ‘digit’, ‘dewclaw’, ‘nail’, ‘nail-bed’, ‘osteosarcoma’, ‘sarcoma’, ‘osseous metaplasia’, ‘peripheral giant cell granuloma’, ‘granulation tissue’, ‘decalcification’, ‘inconclusive’ and ‘giant cell tumour’.
Clinical details including age, sex and neuter status, breed and presenting signs were recorded for all 41 cases where available. Further information was then sought and acquired for 22 of these 41 cases using a questionnaire to the submitting veterinary practices, approved by the Royal Veterinary College Clinical Research Ethical Review Board. The requested data comprised further information about the cat (confirmation of signalment, vaccination status, indoor/outdoor access, concurrent conditions and treatments, current age or date and cause of death if no longer alive), about the mass (whether the mass was the reason for presentation to the veterinary surgeon, the foot and digit affected, duration, colour and size of the mass, presence of pain, lameness, inflammation, concurrent nail-bed infection, nail-bed involvement, local recurrence, and details of any previous or concurrent treatments), whether there was any history of trauma and whether the mass was radiographically assessed.
Haematoxylin and eosin-stained 5 μm sections of each mass were blindly reviewed by pathologists (MJD, AF, AMP). Each individual mass was assessed for the presence of MNGCs (defined as three or more nuclei per cell), osseous metaplasia and spindle cells. The mitotic count per 10 high-power fields (HPFs, 400×) was also recorded, together with which cell types included mitotic figures. Other features recorded were exophytic or invasive growth, presence of ulceration, capillary formation, reactive bone changes, vascular invasion, haemorrhage, fibrin, oedema, necrosis and involvement of the nail-bed epithelium. The presence of any inflammation was scored on a subjective basis and allocated a numerical value (none = 0; mild = 1; mild-to-moderate = 2; moderate = 3; moderate-to-severe = 4; severe = 5) and the cell types involved were recorded.
Statistical analysis of the data was conducted using Graphpad Prism 6 (GraphPad Software). Two categorical variables were analysed using χ² (sex, limb or digit prevalence) or Fisher’s exact test if there were two binary variables (pedigree vs non-pedigree). A P value of <0.05 was considered significant. The breed of cats in the study population was compared with the breed prevalence of the control population (n = 3771); the control population was based on cats from which fixed tissue samples were received by the Finn Pathologists laboratory throughout the study period and with any diagnosis.
Results
Signalment, clinical presentation and outcome
Signalment data were obtained for all 41 cats in this study (Table 1). The age of 36 of the affected cats was known (range 1–18 years; median 11 years). Sex was recorded for all 41 cats in the study, with 29 males (70.7%) and 12 females (29.3%); this difference was statistically significant (P = 0.008). All but two cats (one male, one female) were recorded as neutered. Thirty cats were recorded as domestic shorthair (DSH; 73.2%), two cats as Siamese (4.9%) and one each (2.4%) as domestic longhair (DLH), ‘domestic cat’, Maine Coon–DSH cross, European Shorthair, Persian, British Blue and British Shorthair. The breeds of two cats were not recorded. There was no statistical difference (P = 0.205) between the prevalence of non-pedigree cats (DSH, DLH and ‘domestic cat’; 32/39 cats with the breed recorded) vs pedigree cats in the study population when compared with the control population.
Signalment, affected foot and digit, and outcome for 41 cats with this novel nail-bed lesion
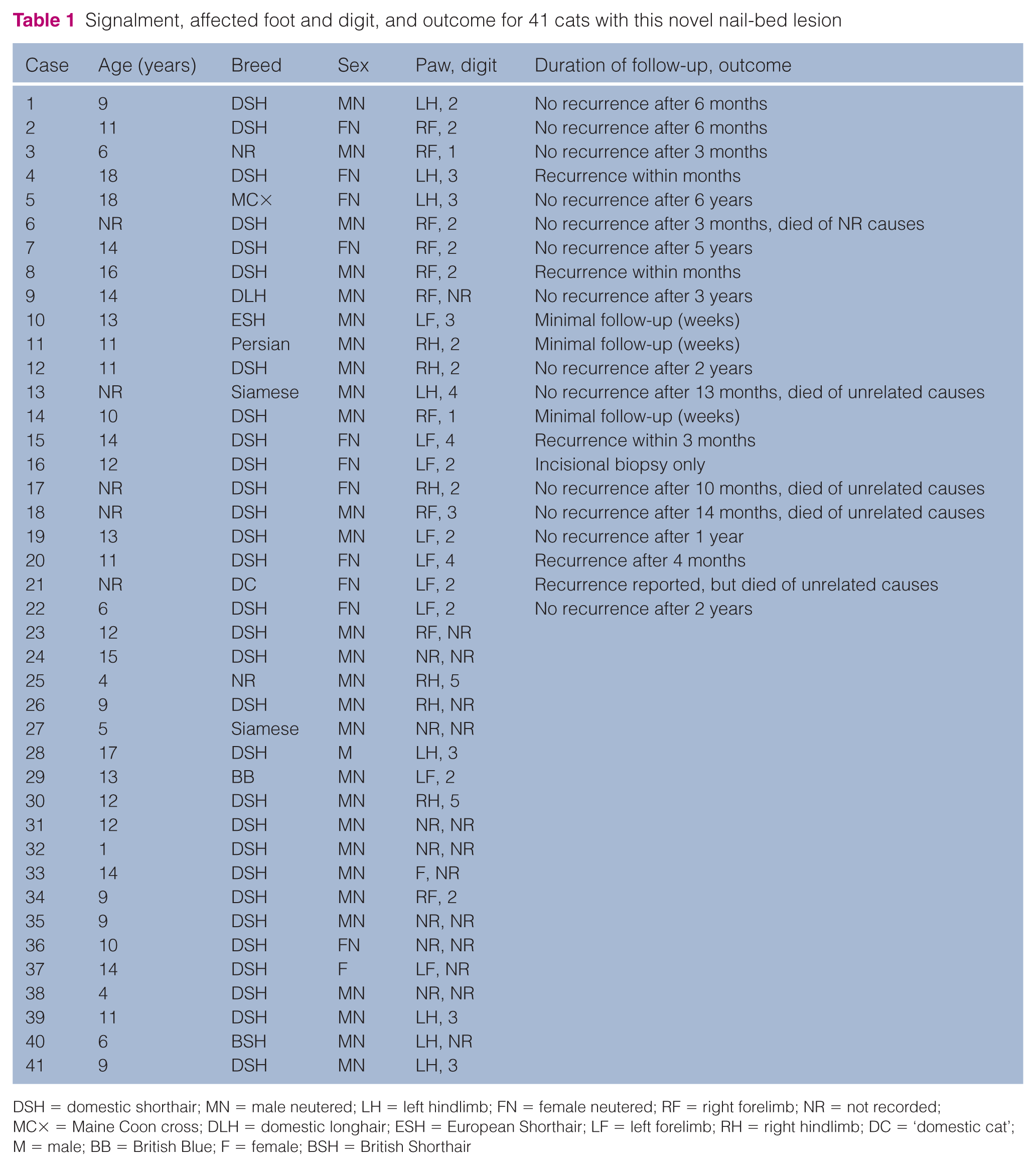
DSH = domestic shorthair; MN = male neutered; LH = left hindlimb; FN = female neutered; RF = right forelimb; NR = not recorded; MC× = Maine Coon cross; DLH = domestic longhair; ESH = European Shorthair; LF = left forelimb; RH = right hindlimb; DC = ‘domestic cat’; M = male; BB = British Blue; F = female; BSH = British Shorthair
Of 22 cats with further clinical information available, 19 had indoor/outdoor access and two were indoor-only (one was not recorded), while 16 were fully vaccinated, five were not and the vaccination status of one cat was not recorded.
The affected limb was recorded for 34 cases (Table 1), with eight lesions (24.2%) affecting the left hindlimb, nine (27.3%) the left forelimb, six (18.2%) the right hindlimb and 10 (30.3%) the right forelimb; there was no statistically significant difference (P = 0.787). One case was described as affecting a forelimb (left or right not specified) and in seven cases the limb was not noted. Overall, 20 (58.8%) cases were affecting a forelimb and 14 a hindlimb (41.2%); again this difference was not statistically significant (P = 0.304). The affected digit was recorded for 28 cases (Table 1), with two lesions (7.1%) affecting digit 1, 14 involving digit 2 (50%), seven arising from digit 3 (25%), three involving digit 4 (10.7%) and two affecting digit 5 (7.1%); this difference was statistically significant (P = 0.0009; Figure 1).
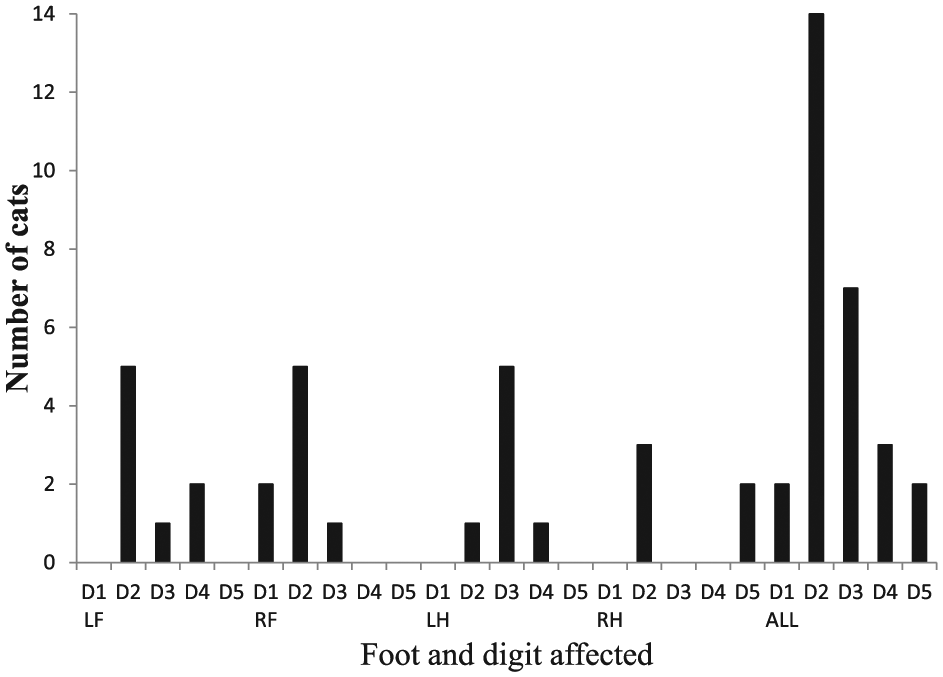
Distribution of lesions on different feet and digits of affected cats. D1 = digit 1; D2 = digit 2; D3 = digit 3; D4 = digit 4; D5 = digit 5; LF = left forelimb; RF = right forelimb; LH = left hindlimb; RH = right hindlimb; ALL = all limbs
Asked if the mass appeared painful on palpation, 8/22 responding primary clinicians replied ‘yes’, 10 responded ‘no’ and four did not answer the question. Five cats were described as lame on the affected limb, while 13 cats were not and there was no response to this question from four cases. The clinicians indicated there was evidence of local inflammation in 18 of the cases, but only one described evidence of more widespread inflammation, in this case a palpably enlarged regional lymph node. The most common terms used to describe the mass were ‘pink’, ‘red’, ‘fleshy’ or ‘flesh-coloured’, and ‘small’. Others terms less frequently used included ‘inflamed’, ‘dark’, ‘raw’, ‘irregular’, ‘raised’, ‘polyp-like’ and ‘shiny’ (Figure 2a,b).
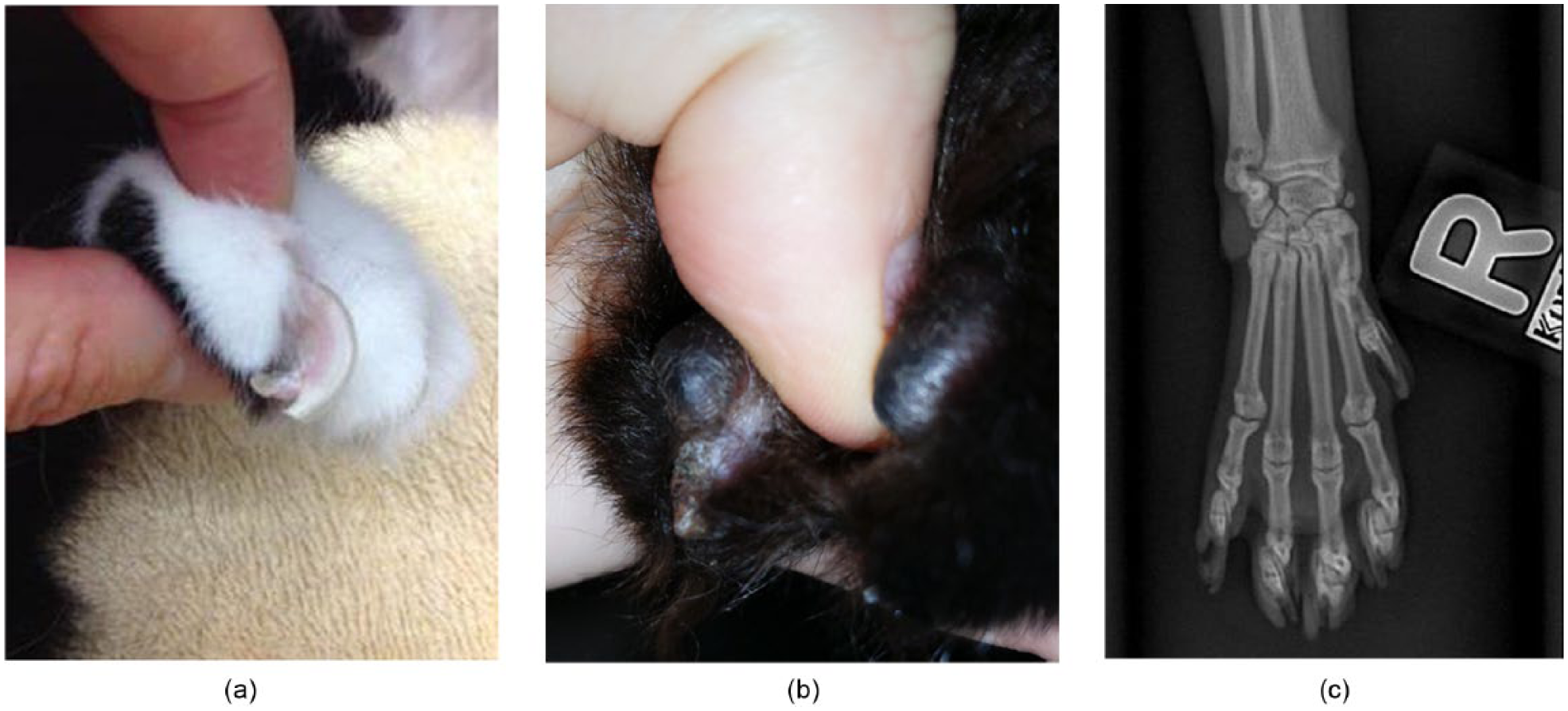
Two photographs and one radiograph of typical lesions arising from the nail-bed. (a) Right forelimb, digit 5: the mass can be seen protruding from the ventral aspect of the nail. (b) Right hindlimb, digit 2: in this case the mass is associated with trauma and injury to the claw. (c) Radiograph of a lesion arising on the right forelimb, digit 5. No radiographic changes can be seen, which correlates with the absence of bone destruction or lysis on histological examination
There was a history of associated trauma to the affected limb in 6/22 cases, and a suspicion of trauma in a further two. One cat presented with the lesion and forelimb lameness after repeatedly jumping out of a top-floor window. Many cases were described as having a concurrent nail-bed infection and/or an injury to the nail itself. In two cases, radiographic assessment of the digit was performed, with no changes evident in one case (Figure 2c), and only soft tissue swelling visible in the second.
In 5/22 cases there was evidence of local recurrence (22.7%) at the original site, occurring within 1–4 months of either excisional biopsy (with histologically incomplete margins) or cauterisation. In three cases the recurring mass was described as similar in appearance to the original lesion. The remaining cases had no evidence of local recurrence, and were either excisional biopsies (often with histologically incomplete margins) or digit amputations, with the length of clinical follow-up available ranging from 1 week to 6 years (Table 1). None of the cats developed any evidence of metastasis or multicentric growths.
Histological features
Forty-one cases were histologically assessed. All of the masses examined were exophytic, variably inflamed, contained large numbers of spindle cells and had areas of capillary formation. All except two cases had obvious areas of ulceration in the sections examined (95.1%; Figure 3a). In one case the presence of ulceration was uncertain and in another case ulceration was apparent in one sample but not in a second sample from a recurrent lesion in the same cat.

Histological appearance of a typical nail-bed lesion. (a) Section through an exophytic and ulcerated (arrows) mass composed of a spindle cell population, areas of osseous metaplasia (asterisk) and multinucleate giant cells (haematoxylin and eosin, × 40); (b) multinucleate giant cells (arrows) surrounded by spindle cells (haematoxylin and eosin, × 400); (c) areas of osseous metaplasia (asterisk), surrounded by spindle cells (haematoxylin and eosin, × 400)
All except one case had MNGCs present in varying numbers (97.6%; Figure 3b); numbers of nuclei per MNGC also varied, with one MNGC containing >100 nuclei. Osseous metaplasia was present in 36 cases (87.8%; Figure 3c) and extensive in one case. The mitotic count ranged from 0 to 25 per 10 HPFs (median 3); all mitotic figures were present within spindle cells as opposed to MNGCs.
Inflammation ranged from mild to severe. Neutrophils were seen in all cases and were the predominant inflammatory cell type, with other inflammatory cell types (macrophages, plasma cells and lymphocytes) also seen in 12 (29.3%) cases. Thirty-four (82.9%) of the masses contained fibrin and 29 (70.7%) had evidence of oedema, with 29 (70.7%) containing some haemorrhage. Haemosiderin was noted in six (14.6%) cases.
Reactive bone changes were present in 13 (31.7%) cases, uncertain in 13 (31.7%) cases and absent in 15 (36.6%) cases.
None of the cases showed any evidence of vascular or lymphatic invasion, nor any evidence of intralesional necrosis.
Involvement of the nail-bed epithelium was histologically apparent in 13 (31.7%) of the cases, but was uncertain or impossible to assess in the remaining cases, often owing to the size of the biopsy. Based on the questionnaire results, 19 (90.5%) cases were described as involving or arising from the nail-bed, one case as probably involving the nail-bed and one as arising from the pad (one participant did not respond to the question).
All masses were measured as part of the histological assessment and the size ranged from 1 × 2 mm up to 10 × 11 mm, based on formalin-fixed, paraffin-embedded tissue samples, with a median size of 6 × 4 mm. Based on the questionnaire results, the masses ranged in size from 2–3 mm up to 20 mm (prior to fixation).
Discussion
The masses described in this study are located on the digit and are generally closely associated with the nail-bed. They are typically described by clinicians as protuberant, pale pink to red, fleshy and small – ranging from 1 to 20 mm in size, ulcerated and inflamed. On histology, the masses are exophytic, ulcerated, inflamed, (typically neutrophilic), with MNGCs, evidence of capillary formation, often with osseous metaplasia, with or without fibrin deposition, oedema and/or haemorrhage, but without necrosis. They may be associated with reactive bone changes but are not destructive. They can have a variable mitotic rate (from 0 up to 25 per 10 HPFs in the masses in this present study), but mitoses are confined to the spindle cell population and are not seen within the MNGCs.
Any deviation from these gross or histological findings should prompt consideration of other diagnoses. In such circumstances, depending on the features present, the gross differential diagnosis would most likely include granulomatous inflammation, other traumatic injuries, digital metastasis of pulmonary adenocarcinoma and primary neoplasms such as soft tissue sarcomas or squamous cell carcinoma. Histological differential diagnoses would include reactive granulation tissue and various forms of sarcoma with the potential to contain MNGCs with or without associated osteoid production, including osteosarcoma, giant cell tumour of bone (GCTB), giant cell tumour of tendons/soft tissues, fibrosarcoma or other poorly differentiated sarcomas.
Male cats were over-represented in the study population; this possibly reflects an increased likelihood of male cats experiencing digital trauma due to roaming, fighting and hunting. Although all digits can potentially be involved, half of the lesions in this study arose on the second digit of the affected limb, implying this is a predisposed site. Trauma, injury to the nail or nail-bed and nail-bed infections may contribute to their development. These masses have some potential for local recurrence if incompletely excised, but metastasis or multicentric growths are not recorded.
In a recently published review of benign bone lesions that may be confused diagnostically with true osseous neoplasms in humans, 1 a proliferative and lytic lesion which contains numerous osteoclast-like giant cells is described, termed a giant cell reparative granuloma; however, this is an intraosseous (ie, central) lesion. It most typically occurs in the mandible or maxilla, but it has also been described in distal appendicular skeletal sites, most notably the phalanges or metatarsal and metacarpal bones. Microscopically, there is a proliferation of fusiform and ovoid stromal cells with no nuclear atypia, punctuated by an irregular distribution of osteoclast-like giant cells. Other authors argue that the lesions affecting the appendicular sites are different from those affecting the jaws. 2
A histologically similar lesion to these masses is the giant cell epulis (recently renamed giant cell granuloma), described in both dogs and cats.3–5 De Bruijn et al 4 described a series of 52 feline epulides, of which 15 were giant cell epulides. In that study the MNGCs and some of the mononuclear cells stained positive for vimentin and for tartrate-resistant acid phosphatase, a marker for osteoclasts. Osteoid and woven bone formation was present in 11/15 cases. The authors speculated the osteoclast-like giant cells in the epulides are most likely formed from a monocyte/macrophage-like precursor that differentiates into osteoclasts under the influence of the mononuclear osteoblast-like stromal cells.
The renaming of such lesions as giant cell granulomas rather than epulides reflects the fact that these lesions are generally considered reactive and non-neoplastic in nature, although in humans the cause of such lesions is still poorly understood; interestingly, an association with trauma, haemorrhage and/or periodontal disease has been suggested in humans. In dogs, these lesions are reported rarely to recur, 3 while in cats they have a higher recurrence rate following marginal excision alone when compared with other feline epulides. De Bruijn et al 4 speculated this recurrence may be related to the rapid growth and poor demarcation of such lesions, associated with a persistent inflammatory component.
In an article reviewing the diagnoses made from 85 surgically amputated feline digits, 6 neoplastic disease was diagnosed in 63 of the submissions, of which 60 were considered malignant. The remaining 22 were purely inflammatory and not described further. Interestingly, two of the tumours were denoted as GCTB, not previously reported in the digits of cats. The authors of that study believed that the fibroblast-like stromal cells in the tumours were the proliferating component and that the giant cells were non-neoplastic, reactive cells with immunohistochemical staining properties consistent with osteoclasts. 6 In that study, the GCTB were from the toes of young cats (3 and 5 years), while the reported age range in the literature for cats with GCTBs from any site is from 1 to 12 years.6–8
Conclusions
This study describes the clinical and histological features of these distinctive feline lesions based on 41 cases, identifying the pathognomonic histological features, as well as potential variations that may be noted by clinicians and pathologists. Histological features include an exophytic growth pattern, with ulceration, neutrophilic inflammation, MNGCs, capillary formation and often foci of osseous metaplasia. Fibrin deposition, oedema and haemorrhage may or may not be evident, but necrosis is absent. Male cats were over-represented in this study and the second digit appears to be a predisposed site. These masses have some potential for local recurrence if incompletely excised; however, there is no evidence that they are malignant (ie, there was no evidence of metastatic potential or multicentric growths identified). Based on these clinical and histological features, the masses in this study appear most similar to giant cell reparative granulomas, which have been described affecting the phalanges in humans, and trauma, injury to the nail or nail-bed, and nail-bed infections may potentially contribute to their development in cats.
Footnotes
Acknowledgements
We would like to thank all of the veterinary practices and cat owners who kindly responded to the questionnaires, supplying the necessary follow-up information for their cases, as well as all the veterinarians who responded to the authors’ request for cases on the International Society for Feline Medicine discussion forum. We would also like to thank the technicians at Finn Pathologists and New Zealand Veterinary Pathology for preparing the haematoxylin and eosin-stained sections of the masses. This research was performed as part of a final-year research project (RAF) supported by the Royal Veterinary College.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.