
Abstract
Objectives
The objective was to investigate the effect of one dose of an inactivated feline herpesvirus-1 (FHV-1), feline calicivirus (FCV) and panleukopenia virus (FPV) vaccine (FVRCP) or one dose of a modified live (ML) FVRCP vaccine on clinical signs and shedding of FHV-1 in specific pathogen-free kittens after challenge with FHV-1 7 days after vaccination.
Methods
Twenty-four FHV-1 seronegative 5-month-old kittens were randomized into three groups of eight kittens. Group 1 kittens were maintained as unvaccinated controls, group 2 kittens were administered one dose of the inactivated FVRCP vaccine subcutaneously (SC) and group 3 kittens were administered one dose of the ML FVRCP vaccine SC. All 24 cats were administered FHV-1 by nasal and oropharyngeal inoculation 7 days later and were observed daily for clinical signs of illness for 21 days.
Results
In the 21 days after FHV-1 challenge, both groups of vaccinated cats were less likely to be clinically ill (indicated by lower cumulative clinical scores) than control cats (P <0.001). There was no statistical difference in total clinical score between the two vaccinated groups (P = 0.97). Although the total clinical score was similar between both vaccines, signs of respiratory disease were significantly fewer in the kittens vaccinated with the inactivated FVRCP vaccine compared with the ML FVRCP vaccine (P = 0.005) during the period after inoculation when the majority of clinical disease was observed.
Conclusions and relevance
Parenteral administration of either the inactivated FVRCP vaccine or the ML FVRCP vaccine can decrease clinical signs of illness due to FHV-1 on a day 7 challenge when compared with controls. Use of either vaccine product is indicated in cats at risk of acute exposure to FHV-1.
Introduction
Feline herpesvirus-1 (FHV-1) infection in cats is a common cause of ocular and upper respiratory tract disease in crowded environments, in particular animal shelters.1–3 FHV-1 infection can induce significant morbidity, resulting in conjunctivitis, rhinitis, sneezing and pyrexia, and some affected cats are euthanized owing to severe signs or to prevent spread of disease. Cats housed in shelters are likely to be infected with FHV-1 within 7 days of entering the shelter. 4 In addition, cats with active FHV-1 infection readily shed large amounts of virus, which can infect other cats housed in close proximity.5,6 Thus, use of vaccines to induce rapid protection against FHV-1 in crowded environments like animal shelters is indicated.
In the USA, there are three types of commercially available vaccines containing FHV-1, including modified live (ML) vaccines for subcutaneous (SC) administration (several manufacturers), ML vaccine for intranasal (IN) administration (Feline UltraNasal FVRCP; Elanco Animal Health) and an inactivated vaccine for SC administration (Ultra Fel-O-Vax; Boehringer-Ingelheim Vetmedica). These FHV-1 vaccines are combined with feline calicivirus (FCV) or both FCV and feline panleukopenia virus (FPV). 7 Although vaccination does not induce a sterilizing immunity for FHV-1, vaccination prior to FHV-1 exposure can result in less severe clinical signs and reduced viral shedding. However, there are few studies evaluating response to FHV-1 challenge within 7 days of the first vaccine, a common shelter occurrence.8,9
Adjuvanted inactivated vaccines have previously been thought to elicit a poor immune response compared with the ML vaccines. However, a study showed that cats administered one SC dose of an inactivated FHV-1, FCV and FPV vaccine (FVRCP [Felocell FVR C; Pfizer Animal Health]) developed protective antibody titers against FHV-1 significantly faster than cats administered a ML FVRCP vaccine (Fel-O-Guard Plus 3; Boehringer-Ingelheim Vetmedica). 10 However, the clinical significance of this difference in seroconversion has not been evaluated after FHV-1 challenge. Thus, the purpose of the present study was to investigate the effect of one dose of an inactivated FVRCP vaccine or one dose of a ML FVRCP vaccine on clinical signs and shedding of FHV-1 in specific pathogen-free kittens after challenge with FHV-1 7 days after vaccination.
Materials and methods
Study design and animals
Three-month-old, mixed sex kittens (12 males, 12 females) were purchased from a FHV-1-, FCV- and FPV-free barrier facility (Liberty Research Laboratories). Prior to entering the study at 5 months of age, the kittens were group housed in a barrier facility and the males were neutered. The kittens were randomized utilizing a random number generator into three groups of eight (four males, four females), group housed in different areas of the facility, and acclimated for 7 days. Before vaccination and then twice weekly throughout the study, pharyngeal samples were obtained by gently rubbing a sterile cotton swab against the oropharynx at the level of the molar teeth. Total DNA was extracted from the swabs and the extracts evaluated for DNA of FHV-1 and DNA of the glyceraldehyde 3-phosphate dehydrogenase (GAPDH) gene (housekeeping gene) by PCR as previously described.2,5 Before vaccination and on day 28 of the study, serum was collected and assayed for FHV-1 antibodies by serum neutralization (Veterinary Diagnostic Laboratory, Colorado State University).
Kittens in group 1 were an unvaccinated control group. On study day 0, kittens in group 2 were administered a single dose of a SC vaccine containing inactivated FHV-1, FCV and FPV (Ultra Fel-O-Vax), and kittens in group 3 were administered a single dose of a SC vaccine containing ML FHV-1, FCV and FPV (Purevax FVRCP; Merial). After vaccination, facility staff members continued to use barrier precautions to avoid cross-infection of the kittens with the ML vaccine strains of FHV-1, FCV and FPV. The total protein concentration of both vaccines was determined. The kittens were housed and cared for in accordance with a protocol that was approved by the Institutional Animal Care and Use Committee at the contract research facility that was used for the study (HQR protocol 170.012).
Challenge inoculation
On day 7, all 24 kittens were challenged with the strain of FHV-1 previously used by the US Department of Agriculture (USDA) in challenge studies (Feline Rhinotracheitis Challenge, Lot 96-13, APHIS, USDA). The stock virus was diluted 1:100 in Dulbecco’s modified eagle medium to a concentration of 105.6 50% tissue culture infective dose (TCID50/ml). On the day of challenge, each kitten was administered 0.1 ml per nostril and 0.3 ml into the oropharynx, receiving a final dose of 105.3 TCID50. Inoculations were completed within 30 mins of thawing the stock FHV-1. The protocol included a rescue clause that allowed for removal from the study and SC fluid therapy, buprenorphine for discomfort and famciclovir (40 mg/kg PO up to three times daily) if kittens developed moderate-to-severe signs of FHV-1 infection leading to inappetence or dyspnea.
Clinical monitoring
Clinical scores (Table 1) were obtained by trained observers who were masked to the vaccine groups starting on day −7 and ending 21 days after FHV-1 challenge (day 28). Two observers were instructed to spend 30 mins per group each morning recording signs, starting with group 1 and ending with group 3, for consistency. Observers were not informed that the order was selected to reduce the potential for transmission of the ML vaccine strain of FHV-1 among kittens. Daily body temperatures were obtained via microchip transponder thermometry as described previously and a body temperature >39.4 °C was considered abnormal. 11
Clinical scoring system used to monitor for clinical evidence of upper respiratory disease

Statistical analysis
Respiratory, ocular and total clinical scores were calculated for the prevaccination (days −7 to 0), prechallenge (days 1–7) and weekly through the postchallenge (days 8–28) study periods. Group clinical scores were compared among study periods using Kruskal–Wallis with pair-wise comparison and significance defined as P <0.05. Viral replication was also totaled for the same study periods. ANOVA was used to evaluate viral replication (FHV/GAPDH DNA ratios) over time. P values <0.05 were considered statistically significant to be included in the model. To evaluate for differences among groups on a given test day for FHV/GAPDH DNA ratios and FHV-1 antibody absorbance values, the Student’s t-test was used.
Results
Prevaccination testing
All cats were negative for antibodies against FHV-1 at the beginning of the study. While all pharyngeal samples contained GAPDH DNA, all prevaccination samples were negative for FHV-1 DNA. The total protein concentrations of the inactivated FVRCP vaccine and the ML FVRCP vaccine was 0.16 g/dl and 0.32 g/dl, respectively.
Clinical observations
During the 7 days after vaccination but before challenge with FHV-1 (days 1–7), 1 cat in group 2 had an elevated body temperature (39.8°C) with lethargy that resolved within 24 h without treatment. Other clinical signs recorded during days 1–7 included sneezing in three cats (one in group 1 and two in group 2) and elevated body temperature in five cats (one cat in each of groups 1 and 3, three cats in group 2). The cats with elevated body temperatures had no other manifestations of disease at the time the abnormality was noted.
After FHV-1 challenge, the most common clinical signs were sneezing, nasal congestion and clear ocular discharge. One kitten from group 1 was removed from the study on day 10 postchallenge owing to severe clinical disease leading to inappetence and weight loss. Thus, daily clinical scores from this kitten were not included in this analysis after it was removed from the study. Other than sneezing, major clinical signs in this kitten resolved after administration of famciclovir (40 mg/kg PO q24h) for 7 days and isotonic SC fluids (60 ml) for 6 days.
The total clinical score, total respiratory score (sneezing, nasal congestion, nasal discharge, coughing) and total ocular score (conjunctivitis, blepharospasm, ocular discharge) were stratified and compared among groups on days 8–14, days 15–21, days 22–28 and days 8–28 after FHV-1 challenge on day 7. The mean and range for the clinical score in the different periods and groups are listed (Table 2).
Mean and range for the total clinical score, total respiratory score (sneezing, nasal congestion, nasal discharge, coughing) and total ocular score (conjunctivitis, blepharospasm, ocular discharge) among groups on days 8–14, days 15–21, days 22–28 and days 8–28 after feline herpesvirus-1 challenge on day 7

Over the 21 day postchallenge inoculation period (days 8–28), both groups of vaccinated cats were less likely (P <0.001) to be clinically ill (indicated by lower cumulative clinical scores) than control cats. The highest total clinical scores during the postinoculation period (days 8–28) were observed on days 15–21 with 267/589 clinical score points observed. During this period when cats were most clinically ill, both groups of vaccinated cats (group 2 and group 3) were less likely to be clinically ill than control cats (P <0.001 and P = 0.01, respectively) (Figure 1). There were no statistical differences in total clinical score during the 3 week study period (days 8–28) and days 15–21 between the two vaccinated groups (P = 0.97 and P = 0.32, respectively).
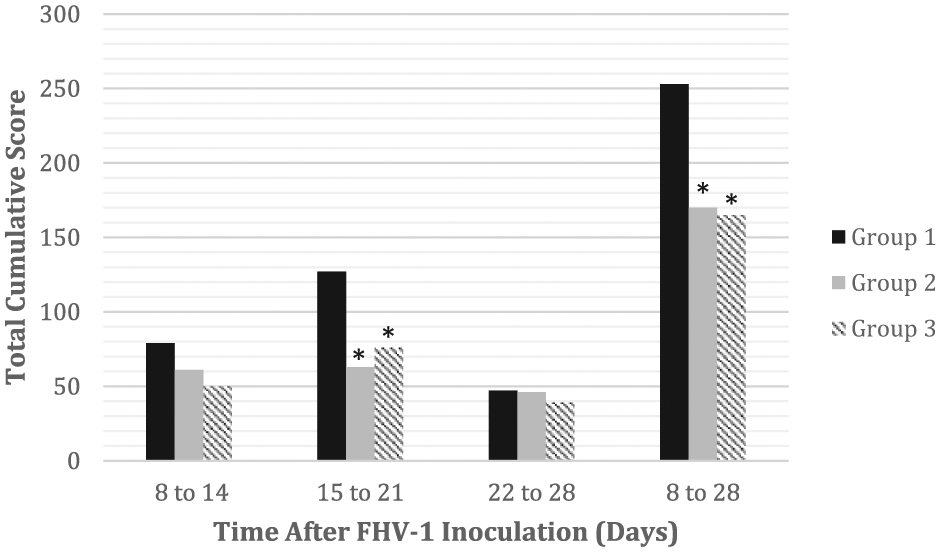
Total cumulative score for each group on days 8–14, days 15–21, days 22–28 and days 8–28 after feline herpesvirus-1 (FHV-1) challenge on day 7. During the 3 week period (days 8–28) after FHV-1 inoculation and the period when cats were most clinically ill (days 15–21), both groups of vaccinated cats (groups 2 and 3) were less likely to be clinically ill than control cats (P <0.001 and P =0.01, respectively). During these periods (days 8–28 and 15–21), there was no statistical difference between the vaccinated groups (P = 0.97 and P = 0.32, respectively)
On days 15–21, group 2 had significantly lower respiratory scores than group 3 (P = 0.005) and group 1 (control cats) (P <0.0001) (Figure 1). On days 22–28, group 2 had significantly lower total respiratory scores than group 1 (P = 0.003) (Figure 2). There was no significant difference in the total respiratory scores between group 3 and group 1 on days 15–21 (P = 0.14) and days 22–28 (P = 0.74). During the postchallenge inoculation period (days 8–28), both groups 2 and 3 had a significantly lower total respiratory score compared with group 1 (P <0.01) (Figure 2). Both group 2 and group 3 had significantly lower ocular scores on days 15–21 compared with group 1 (P < 0.01). Although difference in the total ocular score between groups 2 and 3 (P = 0.15) on days 15–21 was not observed, ocular scores were lower in group 3 when compared with group 2 on days 22–28 (P = 0.03).

Total respiratory score for each group on days 8–14, days 15–21, days 22–28 and days 8–28 after feline herpesvirus-1 (FHV-1) challenge on day 7. Kittens that received a single parenteral inactivated FVRCP vaccine (group 2) during the postinoculation observation period (days 15–21) had significantly lower respiratory scores than kittens that received a single parenteral modified live FVRCP vaccine (group 3) (P = 0.005) and control cats (group 1) (P <0.0001). On days 22–28, cats in group 2 had significantly lower total respiratory scores than group 1 (P = 0.003). During the 3 week period (days 8–28) after FHV-1 inoculation, cats in both vaccinated groups (group 2 and 3) had significantly lower total respiratory scores compared with the unvaccinated group (group 1) (P <0.01)
Assay results after FHV-1 challenge
FHV-1 DNA quantitative PCR results are presented as a ratio of FHV-1 to the housekeeping gene GAPDH DNA to standardize specimens and to ensure that viable feline cells (GAPDH-positive) were present in the pharyngeal swab sample. Of the 242 samples collected after vaccination, 233 had GAPDH amplified from the pharyngeal samples and 122 were positive for FHV-1 DNA. Those samples positive for GAPDH were used in the calculation of the FHV-1/GAPDH ratios for comparison among groups over time. Statistical differences were not detected over time by ANOVA or daily by Student’s t-test (Figure 3). In addition, on day 28, all kittens were positive for FHV-1 antibodies in serum. No differences among group mean FHV-1 antibody absorbance values were noted on day 28.

Quantitative PCR analysis on pharyngeal swab DNA was conducted throughout the study, starting with vaccination date and continuing through the 21 day postinoculation observation period. Statistical differences in feline herpesvirus-1/glyceraldehyde 3-phosphate dehydrogenase (FHV-1/GAPDH) were not detected in the days postinoculation (dpi) between unvaccinated controls (group 2), kittens vaccinated with single parenteral inactivated FVRCP vaccine (group 1) and kittens vaccinated with single parenteral modified live FVRCP vaccine (group 3)
Discussion
In this study, we demonstrated that after FHV-1 challenge, kittens administered a single dose of either a ML FVRCP or inactivated FVRCP vaccine had significantly fewer clinical signs of disease compared with the unvaccinated control group with no statistical difference in the total clinical score between the two vaccinated groups. Although the total clinical score was similar between both vaccines, signs of respiratory disease were significantly less in the kittens vaccinated with the inactivated FVRCP vaccine compared with the ML FVRCP during a period postinoculation when a majority of clinical disease was observed. In addition, although there was a statistically significant lower total ocular score for the kittens vaccinated with the ML FVRCP compared with the inactivated FVRCP on days 22–28, all score points during this period were from a single cat in the inactivated FVRCP group that developed chronic FHV-1 conjunctivitis and clear ocular discharge.
No major side effects were noted with either the ML or inactivated FVRCP vaccines used in the study; however, one cat that was administered the inactivated FVRCP vaccine (group 2) had a fever with lethargy and pain at the site of injection for <24 h after injection. Vaccine components such as adjuvants, nucleic acids, peptides, lipids and carbohydrates induce the innate immune system leading to activation and secretion of cytokines and chemokines. This inflammatory response, while helpful in establishing adaptive immunity, is the cause of local vaccine reactions in some cats, leading to the most commonly reported vaccine reactions, including lethargy, anorexia, fever and local inflammation at the site of injection shortly after vaccination. 12 The inactivated vaccine used in the present study contains a proprietary adjuvant that is not aluminum based. Aluminum-based adjuvants have previously been reported to be associated with vaccine-associated sarcomas in cats. 12 More recent studies have found no relationship between the use of inactivated vs ML vaccines and the risk of subsequent sarcoma formation.7,13–15
It was recently proven that administration of vaccines grown on Crandell Rees feline kidney cells (CRFK) can induce antibodies that react with feline renal tissues, and repeated inoculation of CRFK lysates can induce interstitial nephritis.16–18 The most immunoreactive antigen was shown to be alpha-enolase and these antibodies are markers of inflammation in people.17,18 The inactivated FVRCP used in the prior studies has been additionally purified and re-branded as the 0.5 ml dose vaccine utilized here (Ultra Fel-O-Vax). The total protein concentration of the inactivated vaccine was 50% less than the ML FVRCP vaccine. Further studies will be required to determine whether this results overall in fewer side effects in larger numbers of vaccinated cats.
One kitten from group 1 was withdrawn from the study on day 10 postchallenge owing to severe clinical disease leading to inappetence and weight loss. After removal from the study, the kitten was administered oral famciclovir and SC fluids with resolution of clinical signs, appetite and hydration status within 1 week of treatment, besides occasional sneezing. Clinical scores from this kitten were not included in the statistical analysis after removal from the study, which could have artificially lowered the clinical score of the kittens in group 1. The reason why this kitten was more clinically ill than others in the same group is unknown. However, as all kittens were administered the same FHV-1 challenge dose, these findings likely indicate a less robust immune response to the viral challenge compared with the other kittens.
A previous serological study showed that cats administered one SC dose of either an inactivated or ML FVRCP vaccine did not develop protective antibody titers until 14–28 days postvaccination, with all cats in the inactivated vaccine group having protective antibody titers at day 14. 10 In the current study, both vaccines induced similar decreases in total clinical scores in the 1–3 weeks following FHV-1 challenge, suggesting an effect as early as 7 days postvaccination. This early protection against FHV-1 prior to protective antibody titers is supportive of early induction of cell-mediated immunity by FVRCP vaccines. All kittens in the study were purchased from a specific pathogen-free facility and were tested as seronegative for FHV-1 prior to enrollment, thus these kittens did not have maternal derived FHV-1 antibodies. Additional field studies are needed to evaluate the effect of maternal antibody interference on vaccine immunity for FHV-1 in the general cat population.
Although both vaccines significantly decreased the overall clinical disease of FHV-1 infection compared with the control group, total respiratory scores were lower for the kittens administered the inactivated vaccine. The statistical difference in respiratory score in group 2 compared with group 3 as early as 14 days postvaccination (days 15–21) may be explained by earlier induction of innate or acquired cell-mediated immunity and may relate to the presence of the adjuvant. In future studies, specific and non-specific immune functions induced by the different types of FVRCP vaccines should be studied.
Previous FHV-1 challenge studies have amplified FHV-1 DNA from oropharyngeal swabs after vaccination but before FHV-1 challenge with an IN FVRCP vaccine, suggesting that the FHV-1 PCR-positive results were from the IN FHV-1 vaccine strain.8,19 In the present study, FHV-1 DNA was not amplified from oropharyngeal swabs after vaccination with parenteral FVRCP vaccines. Regardless, as commercially available FHV-1 PCR assays amplify DNA of both vaccine strains and field strains of FHV-1, previous vaccinations for FHV-1 should be considered when interpreting FHV-1 PCR.
Statistical differences in viral shedding were not detected between the groups. In a previous study, kittens that were administered both a ML IN and parenteral FVRCP vaccine had significantly lower FHV-1/GAPDH ratios than unvaccinated kittens or kittens that received the SC FHV-1 vaccine alone. 8 The importance of lower viral shedding with vaccination and whether it equates to reduced infectivity is unknown, but it is unlikely clinically significant as the infective dose of FHV-1 is believed to be low. 20 On day 7 postinoculation, group 2 had an elevated FHV-1/GAPDH ratio compared with the other groups, owing to two cats having a large amount of FHV-1 DNA extracted from the pharyngeal swab. Although the goal is to obtain a representative sample with the pharyngeal swab, if a sample from an active FHV-1 oral lesion was obtained than the amount of FHV-1 DNA extracted could be exceptionally high. Although no statistical difference between groups was found on day 7 postinoculation, the relevance of these two outlier data points in group 2 is difficult to interpret in this small sample size.
The present study supported the use of either inactivated or ML FVRCP vaccine product in cats at risk of acute exposure to FHV-1. Current published vaccine recommendations from the American Association of Feline Practitioners state that cats with a high risk of exposure to FPV should receive the parenteral ML FVRCP vaccine. 7 Therefore, some recommend that the inactivated FVRCP vaccine only be used for the first vaccination in shelters with low risk of panleukopenia or in client-owned cats. The study also supports the theory that both cell-mediated and humoral immune responses are important for protection against FHV-1.
Conclusions
Parenteral administration of either the inactivated vaccine or the ML FVRCP vaccine can decrease clinical signs of illness due to FHV-1 on a day 7 challenge when compared with controls. Use of either vaccine product is indicated in cats at risk of acute exposure to FHV-1.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.