
Abstract
Objectives
The objective was to describe the complications and long-term outcome associated with Kirschner (K)-wire fixation of combined distal radial and ulnar physeal fractures in six cats.
Methods
Medical records (2002–2014) of six referral institutions were searched for cats with combined distal radial and ulnar physeal fractures. Cases with complete clinical files, radiographs and surgical records were retrospectively reviewed. Long-term outcome was assessed via telephone interviews using an owner questionnaire.
Results
Complete files were available for 6/9 identified cases (cases 1–6). All fractures were classified as Salter–Harris type I or II. Five cases underwent open reduction and internal fixation via cross-pinning of the distal radius and intramedullary pinning of the ulna (cases 1–3); fixation of the distal radial and ulnar physes with one K-wire each (case 4); and K-wire fixation of the radial physis in combination with two transulnoradial K-wires (case 5). One case underwent closed reduction and percutaneous cross-pinning of the distal radius under fluoroscopic guidance (case 6). The complications encountered were: reduced radiocarpal range of motion (ROM) (cases 1, 3, 4, 5); implant loosening/migration (cases 1, 2, 5); and radioulnar synostosis (case 4). None of the cats developed angular limb deformity. Long-term outcome (12 months to 7 years after surgery) was graded as ‘excellent’ by the owners in all cases.
Conclusions and relevance
Prognosis is favourable for feline combined distal radial and ulnar physeal fractures following K-wire fixation in cats over 7 months of age. Implant removal after bony union is recommended to minimise reduction in ROM and to prevent implant loosening/migration.
Introduction
Combined radial and ulnar distal physeal fractures in cats are uncommon fractures that occur as a consequence of trauma to the distal antebrachium in skeletally immature animals. 1
These types of fractures heal rapidly, but the prognosis for healing without the development of angular limb deformity depends on the age of the kitten at the time of injury and the remaining growth potential, preservation of blood supply to the epiphysis, the method and time of reduction and the open or closed nature of the fracture.2,3
Various Kirschner (K)-wire fixation configurations have been described in the literature to repair these fractures,1,4,5 but there are no studies that evaluate the outcome following internal fixation.
The aim of this case series is to describe the complications and long-term outcome associated with K-wire fixation of combined distal radial and ulnar physeal fractures in six cats.
Materials and methods
Inclusion criteria
The clinical, radiographic and surgical records from six referral institutions (Queen’s Veterinary School Hospital, University of Cambridge, UK; Queen Mother Animal Hospital, Royal Veterinary College, UK; Dick White Referrals, Six Mile Bottom, UK; Langford Veterinary Services Small Animal Hospital, University of Bristol, UK; Small Animal Hospital, University of Melbourne, Australia; The Veterinary Medical Teaching Hospital, Texas A&M University, USA) were searched for cats with distal radial and ulnar physeal fractures that occurred between 2002 and 2014. Only cases of combined distal radial and ulnar physeal fracture and cases where at least the clinical and radiographic records were available were included in the study.
Retrieved data
The following information was extracted from the clinical records: signalment, traumatic event, concurrent injuries, aftercare recommendations, use of external coaptation, postoperative complications, timing of implant removal (if performed), number of weeks until lameness subsidence (based on repeated orthopaedic examination at follow-up appointments), clinical evidence of angular limb deformity immediately after surgery and at the last recheck appointment. Complications were classified as minor (when either no treatment or medical treatment was necessary), major (when surgical treatment was necessary) and catastrophic (when limb amputation was necessary). Preoperative, postoperative and follow-up radiographs were reviewed by two of the authors (VB and HR). The following information was recorded after reviewing the preoperative and postoperative radiographs: type of fracture according to the Salter–Harris (SH) classification, 2 preoperative displacement, postoperative alignment and apposition achieved, and type and positioning of the implants. The following information was recorded after reviewing the follow-up radiographs: evidence of physeal closure and biological activity of the bone at the fracture site, any change in apposition or alignment, implant loosening or failure or any other signs of complications, and the presence of signs of degenerative joint disease. Physes were considered closed if there was complete cortical continuity and no radiographic evidence of a physis. 6
The following information was extracted from the surgical records: time to fixation, surgical approach, surgical technique, implant sizes, occurrence of intraoperative complications, duration of general anaesthesia and duration of the surgical procedure.
Assessment of long-term outcome (>12 months postoperatively)
The owners were contacted by telephone and the following information was recorded: owner perception of limb function (excellent, good, fair, poor, very poor), presence of any limb deformity in the owner’s opinion, any visit to the first-opinion veterinary practice related to the fracture repair since the last visit at the referral centre, any signs of implant-related problems (eg, soft tissue irritation over the implants) and owner satisfaction with the surgical procedure (very displeased, indifferent, somewhat disappointed, somewhat pleased, very satisfied).
Limb function was classified as ‘excellent’, if the owner reported that there were no detectable gait abnormalities and limb function was the same as before the injury occurred, ‘good’ if there was mild intermittent lameness after prolonged exercise or during cold weather, ‘fair’ if a frequent or continuous mild-to-moderate weightbearing lameness was present, ‘poor’ if continuous moderate-to-severe weightbearing lameness was present and ‘very poor’ if continuous non-weight-bearing lameness requiring amputation was present. 7
Results
Clinical cases
A total of nine cats, seven males and two females, with combined distal radial and ulnar physeal fractures were found (Table 1). Five were domestic shorthair cats; the other four cats were pure breeds. Age at presentation varied between 7 and 26 months. The traumatic event was unknown in all cases. Three of six cats presented with concurrent injuries: soft tissue injuries of the same limb and diaphyseal ulna fracture (case 5); inflammation of the upper airways (case 2); physeal fracture of the right ischiatic tuberosity that was treated conservatively (case 4). Three cases were excluded from the further study as radiographic records were not available.
Case and treatment details of the nine cats with combined distal radial and ulnar physeal fractures
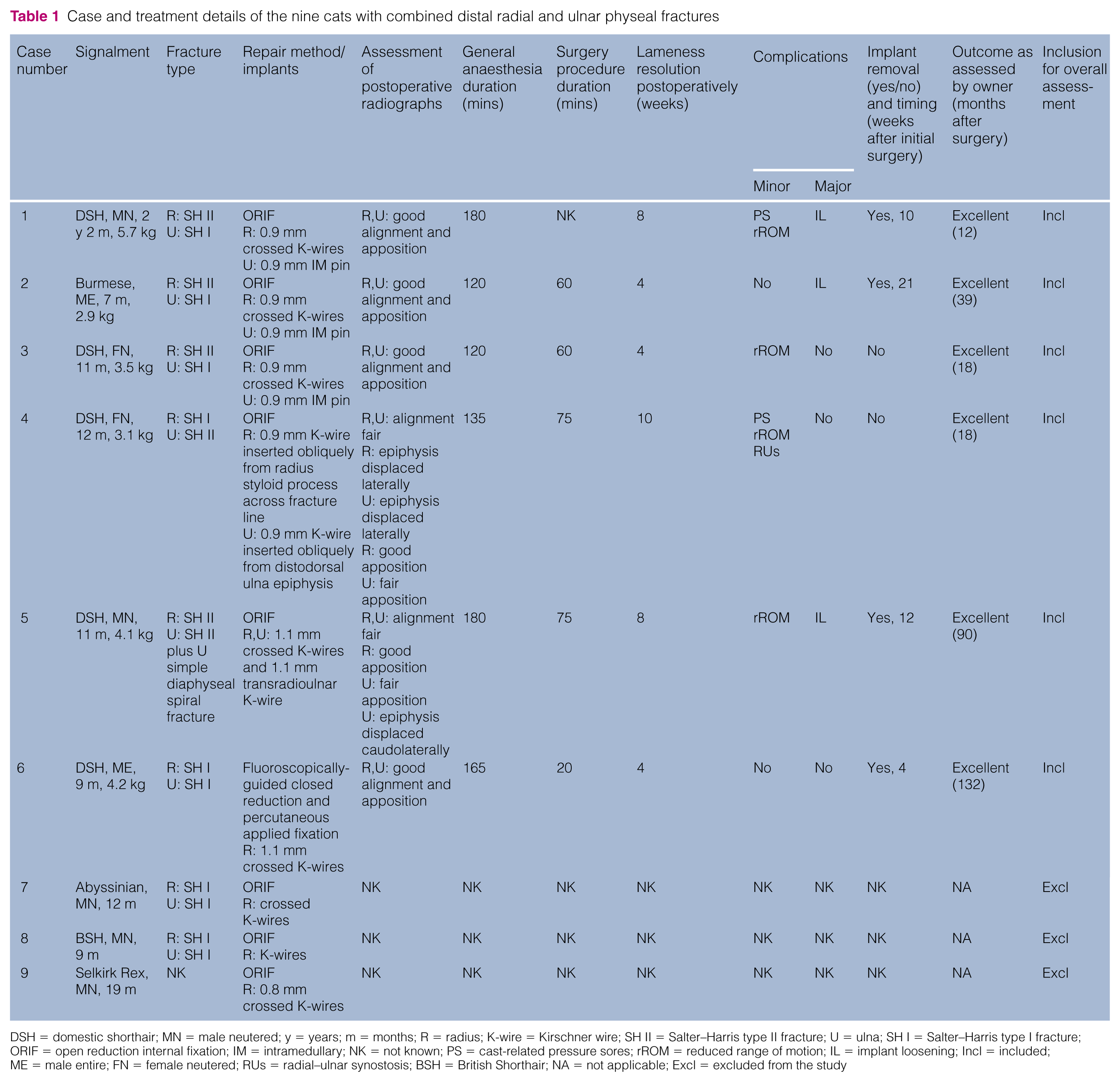
DSH = domestic shorthair; MN = male neutered; y = years; m = months; R = radius; K-wire = Kirschner wire; SH II = Salter–Harris type II fracture; U = ulna; SH I = Salter–Harris type I fracture; ORIF = open reduction internal fixation; IM = intramedullary; NK = not known; PS = cast-related pressure sores; rROM = reduced range of motion; IL = implant loosening; Incl = included; ME = male entire; FN = female neutered; RUs = radial–ulnar synostosis; BSH = British Shorthair; NA = not applicable; Excl = excluded from the study
Review of radiographic records and surgical technique (cats 1–6)
Assessment of the preoperative radiographs revealed that all cats had SH type I or II fractures of the distal radius and ulna (cases 1–6; Figures 1–3). One cat also had a simple spiral fracture of the distal third of the ulnar diaphysis in addition to a SH type II fracture of the ulnar physis (case 5; Figure 3a).

Case 1: (a) Craniocaudal and mediolateral preoperative radiographs of a 26-month-old domestic shorthair cat with a Salter–Harris (SH) type II fracture of the distal radial physis and an SH type I fracture of the distal ulnar physis. (b) Immediate postoperative radiographs showing internal fixation with 0.9 mm crossed K-wires across the radial physis and 0.9 mm intramedullary K-wire in the ulna. Good apposition and good alignment of the radial and ulnar distal physeal fractures were achieved. (c) Radiographs taken 5.5 months postoperatively showing healing of the radial and ulnar physeal fracture, and closure of the distal radial and ulnar physes

Case 4. (a) Craniocaudal and mediolateral preoperative radiographs of a 12-month-old domestic shorthair cat with a Salter–Harris (SH) type I fracture of the distal radial physis and an SH type II fracture of the distal ulnar physis. (b) Immediate postoperative radiographs showing internal fixation with a 0.9 mm K-wire inserted obliquely from the radius styloid process across the distal radial physis and a 0.9 mm K-wire inserted obliquely from the distodorsal aspect of the ulna epiphysis across the distal ular physis. Good apposition of the distal radial physeal fracture and fair apposition of the distal ulnar physeal fracture were achieved. Fair alignment was achieved for both fractures. (c) Radiographs taken 10 weeks postoperatively showing healing of the radial and ulnar distal physeal fractures, closure of the radial and ulnar physes, and synostosis of the distal radial and ulnar metaphyses

(a) Case 5: craniocaudal and mediolateral immediate postoperative radiographs of an 11-month-old domestic shorthair cat (DSH) with a Salter–Harris (SH) type II fracture of the distal radial and ulnar physes repaired with a 1.1 mm K-wire inserted from the radial styloid process across the radial physis into the lateral cortex of the radius, and a second 1.1 mm K-wire from the ulna styloid process across the ulnar physis into the caudomedial cortex of the radius. A third 1.1 mm K-wire was also placed parallel to the fracture line across the radial and ulnar metaphyses. Good apposition of the distal radial physeal fracture and fair apposition of the distal ulnar physeal fracture were achieved. Fair alignment was achieved for both fractures. (b) Case 6: craniocaudal and mediolateral immediate postoperative radiographs of a 9-month-old DSH with an SH type I fracture of the distal radial and ulnar physis. Internal fixation was achieved by percutaneous insertion of two 1.1 mm crossed K-wires across the distal radial physis. Good alignment and apposition were achieved
All cats underwent surgical treatment within 48 h of the occurrence of trauma.
The fractures were reduced in an open (case 1–5) or closed fashion (case 6). Whether the reduction was open or closed, it was achieved in all cases by gently levering the distal radial epiphysis into place. This was achieved by applying manual traction onto the metacarpals while the antebrachium was held in a fixed position.
Fracture repair was performed by one of four different techniques.
Technique 1
Following open reduction the fracture was stabilised by applying two K-wires in a cross-pin fashion. The first K-wire was inserted from the radial styloid process across the fracture line into the lateral cortex of the radius, and the second K-wire was inserted from the craniolateral portion of the radius across the fracture line into the caudomedial cortex of the radius. A small K-wire was also inserted as an intramedullary pin into the ulna in a normograde fashion from the distal aspect of the ulna styloid process. The distal ends of the K-wires and the intramedullary pin were bent through 180°, cut and bent to lie flush on the bone (case 1–3; Figure 1).
Technique 2
Following open reduction, surgical stabilisation was achieved by inserting a K-wire from the radial styloid process across the fracture line into the lateral cortex of the radius, and a second K-wire from the ulna styloid process across the ulna fracture line into the caudomedial cortex of the ulna. The distal end of the K-wires were cut flush with the bone (case 4; Figure 2).
Technique 3
Following open reduction the fracture was repaired by inserting a K-wire from the radial styloid process across the fracture line into the lateral cortex of the radius, and a second K-wire from the ulna styloid process across the fracture line into the caudomedial cortex of the radius. A third K-wire was also placed parallel to the fracture line across the radial and ulnar metaphyses. The distal end of the K-wires were cut flush with the bone (case 5; Figure 3a).
Technique 4
The fracture was reduced in a closed manner under fluoroscopic guidance. Internal fixation was then achieved by percutaneous insertion of two K-wires in a crossed-pin fashion across the radial physeal fracture. The distal end of the K-wires were cut so that they were left protruding through the skin about 1–2 cm (case 6; Figure 3b).
Details regarding the surgical approach, size of the implants and duration of surgical procedure and general anaesthesia are presented in Table 1.
Review of the postoperative radiographs revealed good alignment and apposition immediately postoperatively in four cases (Figures 1b and 3b). Implant positioning was satisfactory in all cases except case 4, where the K-wire placed across the radius failed to purchase bone securely in the distal fragment (Figure 2b).
Follow-up radiographs were taken 4–10 weeks after surgery in all cases but one (case 2 had follow-up radiographs taken 10 months after surgery). Alignment and apposition were unchanged in all cases. Implant loosening or failure were not evident in any of the cases. Assessment of bone activity revealed the presence of bridging callus in all cases where a SH type II fracture of the radius or of the ulna was present (cases 1, 3, 4 and 5). Assessment of follow-up radiographs taken for case 6 (SH type I fracture of radius and ulna) 4 weeks after surgery revealed partial closure of both radial and ulnar distal physes.
The distal radial physis had started to close at the radiographic recheck 4–10 weeks postoperatively also in cases 1, 3, 4 and 5, while the distal ulnar physis had started to close only in case 4. No signs of carpal degenerative joint disease were noted in any of the cases.
Synostosis of the distal radial and ulnar metaphyses was noted in case 4, 10 weeks after surgery.
Postoperative care
All cats had external coaptation applied immediately after surgery. Five cats had a cast applied for 3–6 weeks, and one had a modified Robert Jones bandage for 3 weeks (case 2). Bandage changes were performed weekly for the first 2 weeks and every 2 weeks after that. All patients were prescribed cage rest for 4–6 weeks, followed by a gradual increase in indoor exercise for another 4 weeks. In case 6, implant removal was planned and performed 4 weeks after the initial surgery.
Complications
No intraoperative complications were reported in any of the cases, although a surgical report was not available for case 5. Five of six cats developed minor postoperative complications that did not require further treatment. A reduced range of motion (ROM) of the radiocarpal joint in carpal flexion was noted during the last follow-up appointment in cases 1, 3, 4 and 5. Case 4 developed radioulnar synostosis that was noted radiographically 10 weeks postoperatively. Cases 1 and 3 developed cast-related complications (cast slippage and mild cutaneous pressure sores).
Two cases developed complications that required surgical treatment (classified as major complications): cases 1 and 2 returned to the referral hospital 5 and 9.5 months after surgery, respectively, owing to recurrence of lameness on the operated limb and soft tissue swelling around the implants. Implant loosening was confirmed radiographically and further surgery was performed to remove the implants in both cases. In both cats the distal end of the K-wires had been bent through 180° at the time of surgery. Case 5 also suffered implant-related complications: the owner reported that two of the K-wires migrated through the skin within 3 months of the surgery. In this cat the distal end of the K-wires had been cut flush with the bone at the time of surgery. None of the cats developed a clinically evident angular limb deformity immediately after surgery or at the last re-check appointment. Catastrophic complications were not reported for any of the cases.
Outcome
Resolution of lameness after surgery as assessed by orthopaedic examination occurred in all cases over a period of 4–10 weeks (Table 1). Long-term outcome was graded as excellent with regard to limb function by the owners, and all owners were very satisfied with the overall outcome of the surgical procedure (Table 1).
Discussion
The incidence of combined radial and ulnar physeal injuries has been reported in dogs but never in cats. 3 A computer search performed on the database of six referral institutions over a period of 13 years retrieved only nine cats affected with distal physeal fractures of the radius and ulna, demonstrating the rarity of this injury.
The age at presentation of the cats included in this study varied between 7 and 26 months. Radiographic closure of the distal radial and ulnar physes is generally expected to occur at 13–23 months of age. Delayed closure of distal radial and ulnar physes is not unusual in neutered cats as gonadectomy in cats is generally carried out at 5–6 months of age, before closure of these growth plates (13–23 months), 8 and the low level of gonadal steroids may be one of the factors responsible for initiating physeal closure at the onset of puberty.6,9,10 Radiographic closure of the distal radial and ulnar physes does, however, not correspond with cessation of activity of the growth plates; in fact, activity of the feline physes slows down significantly at about 6 months of age and stops at about 10 months of age. After this point the radius in castrated male cats shows minimal increase in length. 11 All the cats included in our study were older than 7 months at the time of injury and therefore had little growth potential left. As very little physeal activity is present at this age, growth retardation due to rigid internal fixation with K-wires inserted in a cross-pin fashion across the radial and ulnar physes ceases to be a cause of concern.5,12,13 Furthermore, the risk of development of angular limb deformity following premature symmetrical or asymmetrical closure of the distal radial physis is expected to be extremely low, 14 and the data obtained from the present case series support this.
In our study, three cats (cases 1–3) underwent open reduction and internal fixation with cross pins in the radius and an intramedullary pin in the ulna. There are three main considerations to support providing internal fixation for an ulnar fracture that accompanies a radius fracture: if the ulna fracture is stabilised before the radius fracture, it aids in maintaining reduction of the radial fracture while the implants are applied; load-sharing decreases the risk of implant failure, particularly in heavy cats or in cats with concurrent injuries to other limbs; and as cats lack a strong interosseus ligament between the radius and ulna and have a much higher relative mobility of these two bones compared with the dog, fixation of the radius alone is unlikely to result in stable fixation of the ulna.4,7 The main disadvantage in providing additional stabilisation of the ulna could be a slight increase in surgical time, although in our study the duration of general anaesthesia for these three cats was similar to the other cats that received internal fixation with different techniques. Excellent fracture apposition and alignment was achieved in these three cases. Two of these cats (cases 2 and 3) had a short recovery period and were sound at the first recheck 4 weeks after surgery. Case 1 remained lame for about 8 weeks after surgery but this was thought to be a consequence of cast-related complications (mild soft tissue pressure-related injuries) rather than being associated with prolonged fracture healing.
One other cat (case 4) underwent open reduction and internal fixation with one diagonal K-wire inserted through the distal radial physeal fracture and one through the distal ulnar physeal fracture. In this cat, fracture reduction immediately postoperatively was suboptimal. Radiographs taken 10 weeks postoperatively revealed that the cat had developed synostosis of the radius and ulna in the metaphyseal region. On clinical examination, reduced range of motion of the carpus was present, although the cat appeared minimally lame. When contacted by telephone 18 months after the surgery, the owner reported that the residual lameness gradually disappeared and graded limb function as excellent. Radioulnar synostosis is a rare complication (2%) of forearm fractures in people that can develop as a consequence of high-energy trauma, iatrogenic injury to the interosseus ligament, prolonged immobilisation or delayed rehabilitation, and implants protruding in the interosseus space.15,16 In this case, the synostosis developed distally to the point where the K-wires penetrated the transcortex and was unlikely to be a consequence of iatrogenic injury. It is possible that the use of a single diagonal K-wire in each bone and the insufficient bone purchase of the radial K-wire in the distal fragment of the radius caused suboptimal fixation stability that resulted in micromotion and exuberant callus formation, which then could have led to radioulnar synostosis in the region just adjacent to the fracture line. It is also possible that the synostosis could have developed as a consequence of high-energy trauma. Other contributory factors could be the presence of a concurrent injury to a pelvic limb (SH type I fracture of the ischiatic tuberosity that was treated conservatively), which is likely to have caused immediate weightbearing onto the forelimb after fracture repair, suboptimal fracture reduction and prolonged limb immobilisation (a cast was applied onto the forelimb for a period of 6 weeks). Although in this cat the synostosis did not appear to have clinical consequences, the surgical technique should be employed, which aids in avoiding the development of radioulnar synostosis.
One cat (case 6) underwent closed reduction under fluoroscopic guidance and percutaneous insertion of crossed pins across the distal radial physeal fracture. No additional stabilisation was provided for the ulna. The cat did not develop any complications, the fracture healed rapidly and the implants were removed 4 weeks after surgery. This treatment model has several advantages: short surgical time (surgery duration was reported to be 20 mins), minimally invasive, short recovery period and early return of limb function. 17 The main disadvantage is that closed reduction under fluoroscopic guidance can be challenging: duration of general anaesthesia in this case was 2 h and 45 mins, indicating that closed reduction can, indeed, take a relatively long time. The distal end of the K-wires in this cat were cut 1–2 cm from the surface of the skin: the advantage of this approach is that it facilitates pin retrieval; the disadvantage is that it could lead to soft tissue irritation and pin tract infections, although none of these complications occurred in this case.
Reduced ROM of the carpus was noted in 4/6 cats at the last recheck appointment, although it did not appear to be causing lameness in any of them. It is possible that it may have developed as a consequence of prolonged immobilisation due to cast application, although in case 5 it could also have been a consequence of scarring secondary to soft tissue injuries, and in cases 1 and 3, where the distal end of the K-wires had been bent, it could have been a consequence of the presence of relatively bulky implants near the joint. Considering that 2/6 cats (cases 1 and 4) also developed pressure sores as a consequence of cast immobilisation, clinicians should consider carefully the use of external coaptation. Although additional stability may be advantageous immediately after surgery to protect the repair against the force generated by the long lever arm acting on the distal physes, it may be preferable to provide external coaptation for less than the 3–6 weeks described in these cases. All four cases that had follow-up radiographs taken 4 weeks after surgery (cases 1, 3, 5 and 6) showed advanced bone healing at this stage, indicating that external coaptation for a reduced period of 1–2 weeks after surgery may have been sufficient.
Implant-related complications developed in 3/5 cats where the implants had been left in situ after fracture healing, indicating that implant removal might be indicated following distal radial–ulnar physeal fracture repair.
Conclusions
The prognosis is favourable for distal radial–ulnar physeal fractures following prompt surgical fixation and accurate anatomical reduction. The risk of angular deformity is low for cats older than 7 months of age at the time of injury. A limitation of this study lies in the small number of cases that we could include. Further studies with higher case numbers would be necessary to establish the incidence of complications associated with each treatment model and the incidence of growth deformities in cats younger than 7 months at the time of injury.
Footnotes
Acknowledgements
We would like to thank Martin Owen and Adrian Wallace for searching their own local database for cases.
Presented as a clinical research abstract at the British Veterinary Orthopaedic Association’s spring meeting in April 2014.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.