
Abstract
Objectives
This study sought to evaluate how Australian veterinarians approach management and monitoring of feline hyperthyroidism and compare these results with a similar survey recently performed in the UK.
Methods
An invitation to complete an online survey was sent to veterinarians in all states and territories of Australia. The survey comprised questions relating to management of hyperthyroidism, use of antithyroid drugs vs radioiodine treatment vs surgical thyroidectomy, in addition to demographic information for respondents.
Results
A total of 546 clinicians completed the survey. The most commonly preferred treatments for long-term management of feline hyperthyroidism were antithyroid medications (305/546; 56%) and radioiodine (210/546; 38%), with substantially more respondents selecting radioiodine when cost was removed as a consideration (425/546; 78%). However, most respondents had treated or referred few cases for radioiodine (median 2). Most veterinarians (500/546; 92%) used antithyroid medications either long term or prior to definitive treatment of hyperthyroidism. For medical management, 45% (244/546) of veterinarians used twice-daily carbimazole. Half of respondents (274/546) aimed to maintain the total thyroxine concentration anywhere within the laboratory reference interval in hyperthyroid cats without chronic kidney disease. Blood pressure monitoring was uncommon. Surgical thyroidectomy was rarely performed.
Conclusions and relevance
Radioiodine was more frequently preferred by Australian veterinarians compared with those in the UK, likely associated with greater availability, reduced cost and shorter hospitalisation times in this jurisdiction, although antithyroid medications were the most frequently used treatment modality. Barriers remain to its utilisation, however, including perceived cost, misconceptions with regard to expected success rate and accessibility. Recent changes to recommendations on the management and monitoring of hyperthyroid cats do not appear to have been widely adopted by veterinarians at this time.
Introduction
Hyperthyroidism, first described in cats in 1979, is the most common feline endocrinopathy in most developed nations.1,2 Recognised options for management of feline hyperthyroidism include administration of radioiodine, chronic daily dosing with antithyroid medication (orally or transdermally) and surgical thyroidectomy. 1 More recently, an iodine-restricted prescription diet has become available in certain countries. 3
Radioiodine is regarded as the gold-standard treatment, with advantages including the following: (i) potential for curative treatment, with approximately 94% of cats cured following a single treatment; 4 (ii) efficacy independent of location and type of hyperfunctional thyroid tissue; (iii) longer median survival than cats treated with antithyroid drugs; (iv) superior cost-effectiveness for cats surviving beyond 1 year following diagnosis compared with antithyroid drugs; and (v) safety, with minimal adverse effects and no requirement for general anaesthesia or even sedation in most instances.4–8 However, restricted accessibility and requirement for hospitalisation can represent potential barriers to radioiodine use.7,9 Curative success of thyroidectomy is dependent on the location of hyperfunctional thyroid tissue, which is important, as ectopic hyperfunctional thyroid has been reported in 4–23% of hyperthyroid cats.10,11 Complications can encompass iatrogenic hypoparathyroidism (6% of patients in one study), recurrent laryngeal nerve damage and incomplete surgical resection. 12 Additional risk exists in anaesthetising older feline patients with comorbidities such as chronic kidney disease (CKD) and thyrotoxic cardiomyopathy. 12 Overall, 2% postoperative mortality has been reported. 12 Reported recurrence rates are 5–11%, using various surgical techniques.12,13 Antithyroid drugs can be an effective option but do not prevent progression of the underlying pathological process in the thyroid.14,15 Therapeutic efficacy is also highly dependent on compliance with daily dosing.14,16 Adverse effects have been reported in 18% of patients receiving methimazole, including anorexia, vomiting, lethargy and, less commonly, self-induced facial excoriation, cytopenias, lymphadenomegaly, hepatopathy and myasthenia gravis.17,18 The prevalence of side effects using carbimazole is reported to be lower.19,20
A recent survey of general practice veterinarians in the UK evaluated their approaches to management and monitoring of feline hyperthyroidism. 21 In the UK, disadvantages of radioiodine have included limited availability and long waiting times, in addition to lengthy hospitalisation after treatment due to radiation safety requirements (up to 4–5 weeks, until recently). In the UK survey, oral antithyroid medication was the most commonly preferred treatment option; however, 59% of respondents agreed that radioiodine was the gold standard for treatment of hyperthyroidism. 21 This highlights a discrepancy between the gold standard and the preferred treatment choice amongst veterinarians in the UK, raising the question of why such a discrepancy exists.
Radioiodine treatment in Australia differs in several ways to that in the UK. In particular, access to radioiodine treatment facilities is greater, with 20 radioiodine treatment facilities (https://madmimi.com/p/525d16 lists treatments facilities in Australia) across 5/6 Australian states (servicing a human population of 25 million people) and generally shorter post-treatment hospitalisation, typically 5–7 days. As a result, we hypothesised that, compared with the UK, radioiodine may be more widely utilised among Australian veterinarians and more widely accepted as the gold standard treatment.
This study aimed to evaluate how Australian veterinarians approach management of feline hyperthyroidism and compare these results with the UK survey.
Materials and methods
A survey of Australian general practitioners was modelled on the previous UK survey. 21 A list of veterinary practices that treat cats in the Australian Capital Territory (ACT), New South Wales (NSW), Northern Territory (NT), Queensland, South Australia (SA), Tasmania, Victoria and Western Australia (WA) was compiled using several directories, including the Australian business telephone directory and any state registers of veterinary practices. An invitation to participate in the survey was sent to each veterinary practice (including branches) by email or post (if an email address was unavailable), including a request to forward survey information to all veterinarians in the practice. A total of 1705 invitations were sent by email (ACT [n = 26], NSW [n = 527], NT [n = 17], Queensland [n = 368], SA [n = 124], Tasmania [n = 46], Victoria [n = 401] and WA [n = 196]) and 392 invitations by post (ACT [n = 5], NSW [n = 99], NT [n = 1], Queensland [n = 144], SA [n = 23], Tasmania [n = 8], Victoria [n = 84] and WA [n = 28]). Reminder emails were sent after 1, 3 and 4–5 weeks. Reminders were not sent to postal recipients owing to cost constraints. An Apple iPad mini and three $100 textbook vouchers were offered as inducements for participation (winners were determined by ballot).
The questionnaire, hosted by the University of Bristol’s online survey program (Bristol Online Surveys), was based on that performed by Higgs et al, 21 with minor amendments to ensure appropriateness for Australian veterinarians. It comprised 32 questions divided into sections, including the following: (i) general information on approach to management of hyperthyroidism; (ii) management of hyperthyroidism with antithyroid drugs; (iii) radioiodine treatment; (iv) surgical treatment of hyperthyroidism; and (v) respondent demographic information. At the time of the survey, the prescription diet (Hill’s y/d) had not been released in Australia and as such was not included in questions. We elected to use the same survey platform to minimise differences due to data acquisition.
Data were entered into a Microsoft Excel (Microsoft Office 15) spreadsheet and analysed using a statistical software package (Minitab version 17). Categorical and quantitative responses were analysed using descriptive statistics. Specific categorical responses were compared using χ2 and odds ratio testing of cross-tabulated data. For all tests, P values <0.05 were considered significant.
Results
Demographics
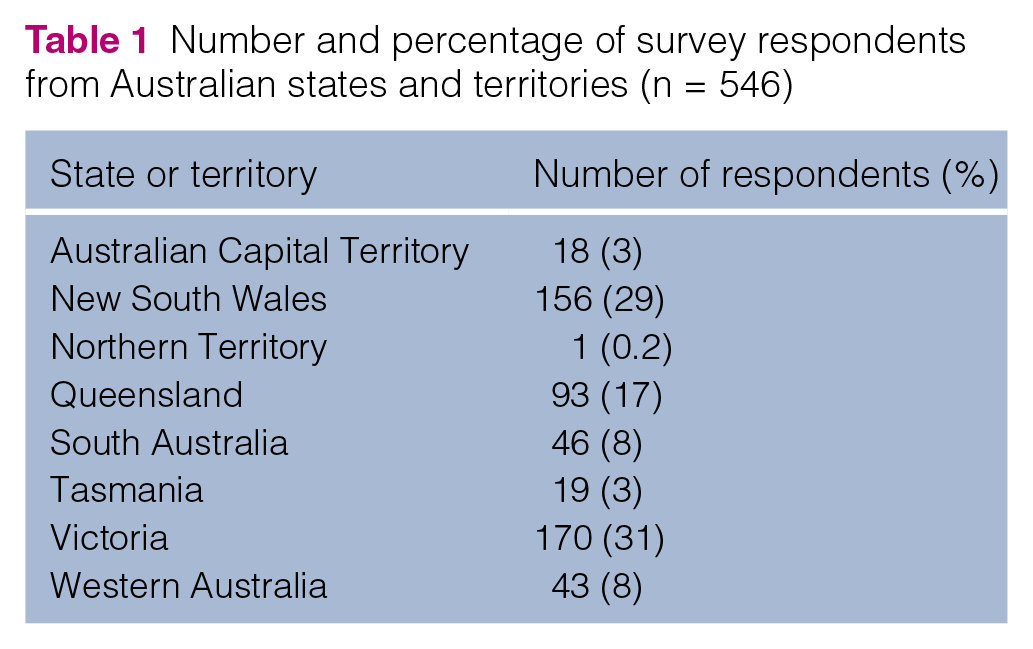
There was a total of 546 respondents (Table 1), representing approximately 6% of registered veterinarians in Australia (9782 veterinarians were registered in Australia in 2012). 22 Of these, 73% were female and 27% were male. Respondents had obtained veterinary training from the University of Sydney (n = 147; 27%), University of Melbourne (n = 135; 25%), University of Queensland (n = 122; 22%), Murdoch University (n = 62; 11%), Charles Sturt University (n = 10; 2%), University of Adelaide (n = 5; 1%) and James Cook University (n = 4; 1%), with the remaining respondents having trained overseas (n = 61; 11%). The median year of graduation was 2000 (range 1958–2014). The median number of veterinarians working in each veterinary practice was 3 (range 1–50). The median estimated percentage of the working day spent with cats was 30% (range 1–100%). In the practice where the respondent was working, 37% (n = 202) had at least one person with postgraduate qualifications in small animal or feline medicine and 23% (n = 123) in surgery.
Number and percentage of survey respondents from Australian states and territories (n = 546)
Management of feline hyperthyroidism
In the previous 6 months, 72% of veterinarians (392/546) had diagnosed 1–5 cats with hyperthyroidism. Ninety-nine (18%) had diagnosed 6–10 cases, 28 (5%) had diagnosed 11 or more, while 27 (5%) had not diagnosed any. Preferred long-term treatment options were oral anti-thyroid medications (n = 223; 41%), radioiodine (n = 210; 38%), transdermal methimazole (n = 82; 15%) and thyroidectomy (n = 20; 4%). Veterinarians in WA were significantly less likely to prefer radioiodine (odds ratio [OR] 0.03, 95% confidence interval [CI] 0.00–0.24; P <0.001) and significantly more likely to choose antithyroid medications (OR 7, 95% CI 3–17; P <0.001). When cost was removed as a consideration, 425 veterinarians (78%) chose radioiodine as their preferred long-term treatment; this was significantly greater than the proportion who preferred radioiodine when cost was a consideration (P <0.001). Of the remaining respondents, preferred treatments were oral antithyroid medication (n = 61; 11%), transdermal methimazole (n = 30; 5%) and thyroidectomy (n = 25; 5%) when cost was not a factor.
Most veterinarians (406/546; 74%) indicated they did not have a practice policy for managing hyperthyroidism. Of those that did, 61 (44%) indicated their practice policy was long-term antithyroid medications, 45 (32%) was referral for radioiodine, 17 (12%) in-house radio-iodine and five (4%) thyroidectomy. The importance of various factors to veterinarians when formulating a long-term management plan is provided in Table 2. Data from eight respondents were excluded from analysis because of an initial computer error that affected data collection for this question alone.
Degree of importance of various factors when formulating a long-term plan for management of feline hyperthyroidism

Counts are provided, with percentage of total respondents in brackets (n = 546)
Antithyroid medication
The majority of respondents (500/546; 92%) used antithyroid drugs as initial treatment for hyperthyroidism, either prior to curative treatment or for long-term medical management, with oral carbimazole (Neomercazole) used most commonly (244/546; 45%), followed by methimazole (Felimazole; Dechra Veterinary Products) (109/546; 20%), transdermal methimazole (17/546; 3%), compounded oral methimazole or carbimazole (16/546; 3%), and carbimazole sustained-release tablets (Vidalta; MSD Animal Health) (10/546; 2%). Remaining respondents (50/546; 9%) had no specific preference.
With regard to monitoring cats receiving antithyroid medications, 328/546 (60%) respondents designed their own monitoring protocol based on their perception of patient needs, 130 (24%) followed a practice policy and were comfortable that this was the best approach, 33 (6%) designed their own monitoring protocol based on owner preference and 31 (6%) designed their monitoring protocol based on manufacturer datasheet guidelines. Some respondents (n = 19; 3.5%) indicated they follow a practice protocol but would prefer more frequent monitoring, while five (1%) indicated they did not believe any monitoring apart from physical examination was necessary. A summary of the frequency of monitoring various parameters in a hypothetical hyperthyroid patient is provided in Table 3. Data from eight respondents were excluded from analysis because of an initial computer error that affected data collection for this question alone. Of respondents selecting ‘other’ in relation to this question, most indicated their frequency of assessment was made on a case-by-case basis.
Frequency of assessment of physical examination and laboratory parameters when respondents were asked the following question: ‘You have recently diagnosed hyperthyroidism in a 12-year-old cat and prescribed antithyroid tablets. Which of the following parameters would you routinely use to monitor the patient and how often?’

Counts are provided, with percentage of total respondents in brackets (n = 538)
TT4 = total thyroxine; ALP = alkaline phosphatase; ALT = alanine aminotransferase; PCV = packed cell volume; CBC = complete blood count; UA = urinalysis; UPCR = urine protein:creatinine ratio
During therapy, 274/546 (50%) respondents aimed for total thyroxine (TT4) concentration to be anywhere in the laboratory reference interval (RI), 186 (34%) aimed for TT4 in the bottom half of the RI and 68 (12%) aimed for the upper half of the RI. One respondent (0.2%) aimed for TT4 to be just above the RI. In contrast, when there was pre-existing CKD, 244 (45%) respondents aimed for TT4 in the upper half of the RI and 84 (15%) respondents for TT4 to be just above the RI. These proportions were significantly different to the proportion of respondents aiming for TT4 in the upper half of the RI or just above the RI when pre-existing CKD was absent (OR 3; 95% CI 2–5; P <0.001). Of the remaining respondents, 98 (18%) indicated that the presence of CKD did not affect their target TT4 concentration, 65 (12%) aimed for TT4 concentration to be in the lower half of the RI and 46 (8%) aimed to ensure the cat was not hypothyroid. Nine respondents (2%) did not monitor renal analytes in hyperthyroid cats.
Adverse reactions had been observed by 40% of veterinarians (217/546) in the previous 12 months (Table 4). Of veterinarians who had seen adverse reactions, 182/217 (84%) had not reported them to the Australian Pesticides and Veterinary Medicines Authority or drug manufacturer. The most common ‘other’ adverse reactions identified were skin reactions to transdermal formulations and diarrhoea.
Frequency and percentage of adverse reactions to antithyroid medications observed by respondents (n = 217)

Surgical thyroidectomy
Only 119/546 veterinarians (22%) had performed one or more thyroidectomies on cat(s) with hyperthyroidism. Of these, 51 (43%) did not routinely submit resected thyroid tissue for histopathological assessment, with 28/119 (24%) submitting 100% of samples, 26/119 (22%) submitting 1–20% of samples and 14/119 (12%) submitting 21–99% of samples. Of samples submitted for histology, thyroid adenocarcinoma was diagnosed in no instances by 27 (43%) respondents, 1–10% of cases by 20 (32%) respondents and 11–50% of cases by 10 (16%) respondents. In cases undergoing bilateral thyroidectomy, recurrence of hyperthyroidism was noted in no cases by 39% of respondents (46/119), in 1–10% of cases by 23% of respondents (27/119) and in more than 11% of cases by 7% of respondents (8/119). Thirty-eight respondents (32%) had never been involved in bilateral thyroidectomy.
Most respondents believed that <10% (n = 305; 56%) or 10–20% (n = 173; 32%) of cats had ectopic thyroid tissue. Nuclear scintigraphy was uncommonly offered, with 51% (72/141) of veterinarians never offering it before surgery.
Radioiodine treatment
Eighty-two percent (447/546) of respondents either agreed or strongly agreed that radioiodine is the ‘gold standard treatment’ for hyperthyroidism, while 4% (n = 24) either disagreed or strongly disagreed with this statement. The remainder (n = 75; 14%) were unsure. With regard to the percentage of cases in which radioiodine was offered to clients, 214/546 (39%) respondents offered it in 100% of cases, 118 (22%) in 81–99% of cases, 66 (12%) in 51–80% of cases and 148 (27%) in <50% of cases. The median number of cases respondents had either personally treated with or referred for radioiodine treatment was two (range 0–800). The closest radioiodine treatment centre was <50 km from 285 respondents (52%), 51–100 km away for 68 respondents (12%), 100–300 km for 90 respondents (16%) and >301 km away for 82 respondents (15%). The remainder (21/546; 4%) did not know the location of their closest radioiodine treatment centre.
A summary of factors impacting respondents’ likelihood of offering radioiodine are provided in Table 5, while the degree of concern caused to clients by various factors as assessed by the veterinarian are explained in Table 6. In relation to the likelihood of referring a hyperthyroid cat for radioiodine treatment, 399/546 respondents (73%) indicated they were either highly or quite likely to do this, while 88/546 respondents (16%) were either highly or quite unlikely to do this. The remainder were unsure (n = 59; 11%).
Effects of various factors on the likelihood of veterinarians offering radioiodine treatment to clients

Counts are provided, with percentage of total respondents in brackets (n = 546)
Degree of concern caused to clients by various factors relating to radioiodine treatment, as assessed by the veterinarian

Counts are provided, with percentage of total respondents in brackets (n = 546)
Most veterinarians (323/546; 59%) considered that >80% of cats were cured by standard doses of radioiodine, with 76 respondents (14%) selecting 61–80% of cats as being cured. The percentage of cats cured by standard doses of radioactive iodine was unknown by 119/546 respondents (22%).
Laboratory testing of serum TT4 concentrations
Most veterinarians (352/546; 64%) were aware of the different laboratory methods available for monitoring TT4. An external laboratory was used for measuring TT4 concentration by 449/546 respondents (82%), with remaining respondents using in-house testing. Half of respondents (225/449; 50%) used an external laboratory where TT4 is measured by enzyme immunoassay.
Discussion
Feline hyperthyroidism is commonly diagnosed by Australian veterinarians. Radioiodine was a preferred long-term treatment option by more than a third (38%) of respondents, which increased to 78% when cost was removed as a consideration. However, antithyroid medications were the most frequently used treatment modality and twice-daily carbimazole was preferred by 49% of surveyed veterinarians. Surgical thyroidectomy was rarely performed.
Greater preference for radioiodine among Australian veterinarians contrasts with the UK survey. In that survey, only 6% of respondents preferred radioiodine treatment for long-term management, rising to 41% when cost was not considered. 21 Factors including reduced hospitalisation times compared with those historically in the UK and more widespread availability of treatment facilities in Australia may have led to a more positive attitude to radioiodine. In our survey, the impact of accessibility was highlighted by significantly reduced preference for this treatment modality among WA veterinarians, where no such facilities currently exist.
In spite of widespread preference for radioiodine treatment, Australian veterinarians treated or referred very few cases for radioiodine treatment (median 2). This suggests that barriers to radioiodine utilisation persist in Australia. Indeed, 22% of veterinarians were unaware of the success rates of radioiodine treatment and an additional 19% underestimated the percentage of cats cured by standard doses of radioiodine. As a result, veterinarians may offer referral for radioiodine, but may not do so in a sufficiently compelling manner for clients to opt for this treatment. Similarly to the survey by Higgs et al, 21 compliance with treatment, ease of drug administration, comorbidities, treatment expense and monitoring emerged as important factors when developing long-term plans for hyperthyroid cats. Importantly, 82% of veterinarians reported they perceived radioiodine treatment cost was of great concern to clients. This contrasts with a survey of UK owners where cost had low impacts on the selected treatment,9 although that may be due to greater adoption of pet insurance in this jurisdiction. Veterinarians may also overemphasise the role of cost in owner decision-making. While there is some variation in treatment expenses for hyperthyroidism, typically the cost of curative treatment approximates 1 year of daily antithyroid medication and monitoring. Therefore, on a cost basis, curative treatment should be strongly considered where a cat is expected to live >12 months after diagnosis.14,23
Despite the advantages of radioiodine, antithyroid therapy was used by >90% of veterinarians in our survey, either for long-term management or prior to curative treatment. Problematically, antithyroid drugs fail to treat the underlying pathological process. As a result, there is a propensity for the primary process to progress, with eventual refractoriness to medical management and sometimes malignant transformation. Indeed, the prevalence of thyroid carcinoma is reported to increase from less than 5% to 19% in cats managed with antithyroid medication for >4 years.14,15 Cats treated with methimazole have shorter survival times than those treated with radioiodine; client compliance with drug administration, poor titration of therapy and drug toxicoses have been hypothesised to account for this observation. 8 While the reversibility of antithyroid medication allows assessment of the effects of restoring euthyroidism on renal function, 14 the importance of trialling this before definitive treatment is now being challenged, particularly when pre-existing azotaemia is absent. A recent study showed that hypothyroid cats that become azotaemic following treatment have shorter survival times. 24 Emphasis should therefore be placed on carefully monitoring thyroid status after definitive therapy to avoid hypothyroidism by pre-emptive replacement therapy with thyroxine, where necessary.
The most commonly used antithyroid medication was twice daily carbimazole, rather than licensed methimazole (Felimazole) or sustained-release once-daily carbimazole (Vidalta). This likely reflects familiarity as the latter two medications have only recently become available in Australia. However, it serves to emphasise the need for veterinarians to remain abreast of new drugs, particularly those that have potential to improve compliance by reducing administration frequency. Transdermal methimazole was often used by respondents to our survey. It is thought to improve client compliance,14,25 but a study evaluating long-term transdermal methimazole use found 17% of owners admitted not treating their cat regularly, suggesting compliance may still be suboptimal. 26 Adverse reactions to antithyroid medications were consistent with previous reports. 14 Interestingly, few veterinarians had reported adverse reactions to the manufacturer or relevant authority, suggesting significant under-reporting exists, similar to the UK study. 21
Surgical thyroidectomy had been performed by approximately one-fifth of respondents in our survey, but only 4% of veterinarians selected thyroidectomy as their preferred treatment, compared with 28% in the UK. 21 Barriers to performing thyroidectomy in general practice, including in Australia, may include concern regarding anaesthetic risks associated with comorbid conditions such as CKD or cardiomyopathy, limited access to nuclear scintigraphy to assess the location of hyperfunctional thyroid tissue, limited experience performing the surgery and absence of adequate postoperative monitoring to manage complications such as hypocalcaemia. The majority of veterinarians were aware that ectopic hyperfunctional thyroid tissue could be present in 4–23% of hyperthyroid cats.10,11
Evaluation of serum TT4 is essential for diagnosis and monitoring of hyperthyroidism. Methods for measuring TT4 include radioimmunoassay (RIA), chemiluminescent enzyme immunoassays (CEIA) and enzyme immunoassays (EIA; also available as in-house assays), with all but RIA being relatively inexpensive and widely available. 27 While CEIA provides similar results to the gold standard RIA, EIA has higher rates of false-positive and false-negative results and tends to underestimate TT4, leading to discordant results in 24% of cases. 27 In Australia, the major veterinary laboratories use different techniques and therefore results cannot be compared between laboratories. Veterinarians must be aware of test methodologies and their varying precision at diagnosing and monitoring hyperthyroid cats using TT4. The in-house EIA has been evaluated with conflicting reports on its usefulness for TT4 measurement, but one study suggested its accuracy to be lower than other methodologies.27–29 With in-house EIAs used by 18% of veterinarians in our survey, and widespread use of a commercial laboratory that uses EIA, many veterinarians may be unaware of the potential for spurious and misleading results. We advise utilising laboratories that use the CEIA methodology, as has been recommended by Peterson. 28 Although generally accepted that the treatment goal when using antithyroid medications is for TT4 concentration to be within the lower half of the RI, 14 50% of respondents aimed for TT4 to be anywhere within the RI and 12% aimed for it to be in the upper half of the RI (in the absence of CKD). This suggests that many cats may be inadequately treated and consequently may continue to experience the adverse pathophysiological effects of hyperthyroidism. While there was a statistically significant increase in the number of respondents aiming for TT4 to be in the upper half or above the RI when CKD was present, many veterinarians do not appear to be aware of current advice regarding management of hyperthyroid cats with concurrent renal azotaemia, which is to avoid hypothyroidism; only 8% aimed to ensure that the patient did not become hypothyroid.
A recent review of best practice for monitoring cats managed with antithyroid medication emphasised regular history taking, serial examinations, body weight and body condition score estimations, TT4 concentrations measured by the same laboratory, renal analytes and systolic blood pressure. 14 In our survey, monitoring in the initial few weeks of therapy was generally adequate. However, during maintenance therapy, blood pressure monitoring was significantly underutilised, with less than half of clinicians complying with monitoring recommendations. 14 Similar observations were made in the survey by Higgs et al. 21 Regular assessment of hyperthyroid cats after treatment is important to prevent devastating hypertensive sequelae such as retinal or intracranial haemorrhage, as well as detrimental effects on renal function. Hypertension is present in 14–23% of hyperthyroid cats at diagnosis, although it has been reported in up to 87% of cats in one study, and importantly, 23% of initially normotensive cats develop hypertension following restoration of euthyroidism.30–32 Hypertension has been correlated with reduced survival times in a retrospective study of cats treated primarily with antithyroid medications and/or thyroidectomy. 33
Practice policies for management of feline hyperthyroidism were reported by approximately one-quarter of veterinarians in our survey. The most common practice protocol was for long-term management with antithyroid medications. Although there may be valid reasons for this, it underscores the importance of continuing to raise awareness of best practice for managing hyperthyroidism and consideration of tailoring long-term treatment plans to the individual patient and owner. For non-azotaemic cats expected to live more than 12 months after diagnosis, practice policies for long-term antithyroid medications may be promoting suboptimal treatment associated with shorter survival times, likely reduced quality of life and increased risk of development of thyroid carcinomas.8,15
The current study suffers from some limitations, similar to those reported by Higgs et al. 21 Inherent limitations of surveys include difficulty with recall, leading to inaccurate responses and bias in responding to the questions by predicting the desired response rather than reflecting the usual practices of the respondent. 34 The distribution of veterinarians in the Australian states and territories was largely similar to the percentages of respondents from these locations in our survey, suggesting the survey may be representative of veterinarians across Australia. 35 In addition to this, the survey was conducted prior to the release of the iodine-restricted prescription diet in Australia and as a result, it is not possible at this time to determine how it will influence treatment decisions for hyperthyroid cats.
Conclusions
Despite radioiodine treatment being more commonly preferred among Australian veterinarians compared with those in the UK, practical barriers persist that limit its utilisation, particularly high initial cost, misconceptions regarding efficacy and availability of referral centres in some regions of Australia. When discussing treatment options with owners, veterinarians should emphasise the significant advantages of radioiodine treatment and its overall cost-effectiveness in cats expected to live >12 months after diagnosis. Long-term antithyroid medication was the most frequently preferred treatment modality for hyperthyroid cats in our survey. Antithyroid medications were also commonly used on a trial basis before definitive management. Current evidence suggests that this may be unnecessary in cats that are non-azotaemic prior to radioiodine treatment, although should still be considered prior to thyroidectomy so anaesthesia is performed in a stable patient. Monitoring practices of veterinarians in our survey were similar to those in the UK survey and may be improved by enhanced emphasis on regular blood pressure determination and appropriately targeting TT4 concentrations while using carbimazole or methimazole in both non-azotaemic and azotaemic hyperthyroid cats. Practice policies for management of feline hyperthyroidism, particularly where they advocate long-term medical management, should be discouraged in favour of tailoring management of hyperthyroidism based on patient and client factors with reference to current literature.
Footnotes
Acknowledgements
We would like to thank the veterinarians who participated in this survey. We would also like to thank the Centre for Veterinary Education, Australian Veterinary Association (including state and territory divisions) and the Australasian Society of Feline Medicine for promoting the survey to their members.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Prizes for the survey were generously donated by the Small Animal Specialist Hospital.