
Abstract
Practical relevance:
Chronic kidney disease (CKD) is one of the most commonly diagnosed diseases in older cats. In most cats, CKD is also a progressive disease and can be accompanied by a wide range of clinical and clinicopathological changes. These ISFM Consensus Guidelines have been developed by an independent panel of clinicians and academics to provide practical advice on the diagnosis and management of this complex disease.
Clinical challenges:
Although CKD is a common clinical problem in cats, the manifestations of disease vary between individuals. Thus there is a need for careful and repeat evaluation of cats with CKD and adjustment of therapy according to individual needs. In addition to addressing problems arising from CKD and improving quality of life (QoL) for the patient, therapy may also target slowing the underlying progression of disease and hence prolonging life. While maintaining QoL is of paramount importance in our patients, this can be challenging when multiple therapies are indicated. In some cases it is necessary to prioritise therapy, given an understanding of what is likely to most benefit the individual patient.
Evidence base:
In preparing these Guidelines, the Panel has carefully reviewed the existing published literature, and has also graded the quality of evidence for different interventions to help to provide practical recommendations on the therapeutic options for feline CKD. This is a field of veterinary medicine that has benefited from some excellent published clinical research and further research findings will undoubtedly modify the recommendations contained in these Guidelines in the future.

Introduction
Chronic kidney disease (CKD) is a common feline disease. Its prevalence will vary between populations, but a large UK study estimated that the prevalence of feline renal disease in first opinion practices was ~4% (CKD was the seventh most common specific diagnosis made). 1 CKD is more common in older cats,2 –4 and may affect ⩾30–40% of cats over 10 years of age. 4 Renal disease was the most common cause of mortality in cats ⩾5 years of age in a UK study, being the cause of death of >13% of cats at a median age of 15 years. 5
The underlying aetiology of CKD often remains obscure. Most cats investigated have chronic tubulointerstitial nephritis and renal fibrosis on histology (Figure 1)6,7 – lesions thought to be the end phase of a variety of potential underlying aetiologies that may include toxic insults, hypoxia, chronic glomerulonephritis, chronic pyelonephritis, upper urinary tract obstructions, and potentially viral infections involving retroviruses as well as a recently recognised morbillivirus.8 –12 Other specific causes of CKD sometimes recognised include amyloidosis, polycystic kidney disease, renal lymphoma, hypercalcaemic nephropathy and congenital disorders – some of these have breed associations.4,8,13

Typical histopathology of a kidney from a cat with chronic kidney disease (CKD), characterised by inflammatory infiltrate, tubular loss, increase in extracellular matrix and fibrosis x 20. Courtesy of Shannon McLeland
Other than age, clear risk factors for development of CKD have not been identified in cats,14 –17 but weight loss or poor body condition, polyuria/polydipsia (PU/PD), higher creatinine concentrations, dehydration and potentially lower urine specific gravity (USG) may indicate the presence, or predict development, of CKD.14 –17
The purpose of these Guidelines is to give practitioners an up-to-date, critically assessed overview of the current diagnostic and treatment options to guide in the practical management of CKD.

Diagnosis and assessment of CKD in cats
Routine diagnosis of CKD in cats
CKD in humans is defined as a sustained (⩾3 months) reduction in glomerular filtration rate (GFR, <60 ml/min/1.73 m2) or evidence of sustained (⩾3 months) kidney damage (eg, structural damage, proteinuria). 18 Although CKD has not been clearly defined in cats, similar principles should apply; notably there should be evidence of sustained functional or structural kidney damage (eg, ⩾3 months’ duration).
As CKD is more common in older cats, these patients should be targeted for more detailed and frequent health assessments. Recommendations from International Cat Care/International Society of Feline Medicine, the American Association of Feline Practitioners and the American Animal Hospital Association suggest health checks every 6 months for cats >7 years of age (including evaluation of body weight, body condition score and blood pressure), together with selected diagnostic testing (including haematology, serum biochemistry screening and routine urinalysis) at least annually.19,20
Historical and clinical findings suggestive of CKD, such as weight loss, altered kidney size, unexplained dehydration, PU/PD, systemic hypertension or an unexplained low USG (<1.035–1.040), also justify further investigation.
A simple, accurate biomarker to assess renal function does not currently exist. Thus in clinical practice the combination of azotaemia (increased serum creatinine and/or urea) and an inappropriately low USG are routinely used to diagnose CKD. However, their interpretation is not always straightforward:21,22
Although often measured together, creatinine is preferred over urea as a marker of GFR as its concentration is inversely related to GFR, and is affected by fewer non-renal factors.
Creatinine is an imprecise marker of GFR though; it lacks specificity if reference intervals are set low enough to detect early stage disease, but lacks sensitivity if reference intervals are set higher.
Creatinine concentration is affected by lean tissue mass and hydration.
Creatinine concentrations (and reference intervals) vary between different assays, analysers and laboratories.
The exponential relationship between GFR and creatinine means that substantial early declines in GFR may be accompanied by only small changes in creatinine,while in the latter stages of disease large changes in creatinine may reflect only small changes in GFR.
Bearing in mind these limitations, in clinical practice feline CKD is often diagnosed on the basis of:
An increased serum creatinine concentration >140 µmol/l (>1.6 mg/dl); together with
An inappropriately low USG (<1.035); and
Evidence that these changes are sustained (over several weeks or months) or with a history suggesting sustained clinical signs consistent with CKD.
However, not all cats with CKD will meet these criteria:
Chronic kidney damage evidenced by structural changes to the kidney recognised on diagnostic imaging or persistent renal-origin elevated proteinuria may be present in the absence of azotaemia or an inappropriate USG.
While relatively few healthy cats will produce a USG <1.035, this can be affected by diet, 23 and occasionally some cats with azotaemic CKD will produce a USG ⩾1.035.24,25
Some cats have reduced urine concentrating ability before they develop overt azotaemia.
A persistent and substantial (>15%) increase in serum creatinine from previously determined baseline values in a cat is also likely to indicate reduced renal function.
For these reasons, serial (eg, annual or bi-annual) assessment of serum creatinine or symmetric dimethylarginine (SDMA – see later) and USG may be helpful in older cats (>7 years of age) to determine changes over time, as this may facilitate earlier or more certain diagnosis of CKD.22,26 Additionally, if there is doubt over the diagnosis, additional testing (see page 222) may be desirable.

Routine investigation and staging of CKD in cats
Where CKD is suspected, a minimum routine database should ideally include:
Full history and physical examination;
Routine urinalysis (to include USG, ‘dipstick’ analysis, urine sediment analysis, urine protein:creatinine ratio [UPCR], and culture where indicated);
Routine serum biochemistry, to include a minimum of proteins, urea, creatinine, electrolytes (Na+, K+, Ca2+, Cl_, PO4_), and other analytes (eg, thyroxine in an older cat) as relevant;
Routine haematology;
Systolic blood pressure (SBP);
Diagnostic imaging (renal ultrasonography is generally more valuable than radiography);
In some situations (eg, unexplained renomegaly) a kidney biopsy or fine-needle aspiration may be desirable.
These investigations are aimed at:
Identifying potential underlying aetiologies of the CKD (which may require specific therapy);
Identifying complications that are arising from the CKD;
Identifying concomitant disease that may affect management (eg, hyperthyroidism).
The International Renal Interest Society (IRIS) has established a CKD staging system 27 based on the cat’s fasting creatinine concentration (see box on page 221). This is valuable as the stage (severity) of disease is related to the prognosis for the patient (see later) and can help to focus attention on appropriate treatments. Staging is applicable in cats with confirmed, stable CKD that are well hydrated, and IRIS substaging is based on UPCR and SBP, two important prognostic and therapeutic parameters.
Advanced and emerging tests for feline CKD
Estimation of GFR
The gold standard in renal function testing is direct determination of GFR. Limited- and single-sample plasma clearance methods (eg, using iohexol, inulin, exogenous creatinine or radiolabelled markers) have made GFR assessment easier to undertake in clinical practice, but the reduced numbers of blood samples may yield greater inaccuracy.21,28 Clinical measurement of GFR is mainly used to confirm suspected CKD in non-azotaemic cats.
Symmetric dimethylarginine (SDMA)
SDMA has become available in the veterinary marketplace as a surrogate marker of GFR and, like creatinine, its reciprocal has a linear relationship with GFR. 29 It appears to offer greater sensitivity than creatinine for detection of early CKD 30 and does not appear to be affected by muscle mass. However, further studies are required to fully evaluate its accuracy in clinical patients as SDMA may also be affected by non-renal factors. 31 Although it cannot currently be recommended as a single screening test for CKD, its measurement may be helpful in supporting a diagnosis of CKD or in staging CKD, especially in cats with marked loss of muscle mass. 27
Serum cystatin C
Serum cystatin C is a useful surrogate marker of GFR in human patients. However, in cats its diagnostic value appears compromised by overlap in values between healthy cats and cats with CKD, and the interference of non-renal factors.32,33
Microalbuminuria
Detection of microalbuminuria is important in the diagnosis of CKD in human patients where there is a high prevalence of glomerular disease, but its clinical significance in cats remains unclear. It is measured using a species-specific assay but a benefit of measuring urine albumin:creatinine ratio (UACR) over UPCR in predicting which cats will develop azotaemia has not been demonstrated. 17
Other assays
Studies have demonstrated that development of renal secondary hyperparathyroidism 34 and increased fibroblast growth factor-23 (FGF-23) 35 may precede azotaemia in feline CKD. However, whether there is any diagnostic utility in these assays remains to be determined.

Routine evaluation of feline CKD patients
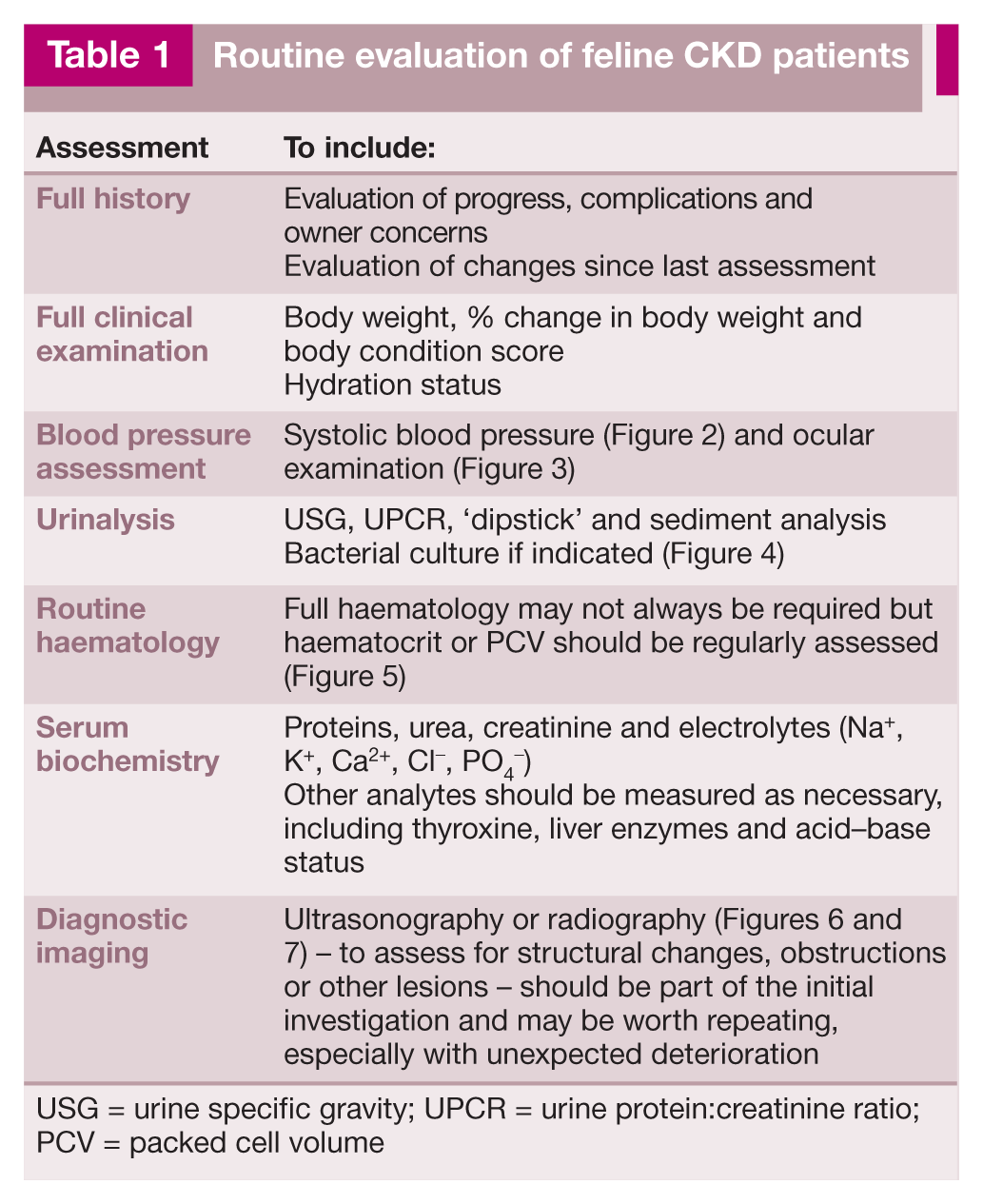
USG = urine specific gravity; UPCR = urine protein:creatinine ratio; PCV = packed cell volume

Blood pressure measurement should be part of the routine evaluation of all cats with proven or suspected CKD. Courtesy of Sarah Caney

Ocular examination (in this case distant indirect ophthalmoscopy) performed in a dark room is valuable, given the strong association between CKD and hypertension. Courtesy of Sarah Caney

Collection of a urine sample by lateral cystocentesis for routine monitoring of CKD. Courtesy of Sarah Caney

Collection of blood for routine monitoring of CKD (note the no restraint technique). Courtesy of Jessica Quimby

A small kidney and loss of corticomedullary distinction are ultrasound findings consistent with feline CKD. Courtesy of Jessica Quimby

Radiographs are helpful for identifying abnormalities such as stones within the urinary tract. Courtesy of Jessica Quimby

Studies evaluating IRIS stage and prognosis

Approach to management
Management of CKD is largely focused on supportive and symptomatic therapy with the aim of improving the quality of life (QoL) of affected cats (especially those in CKD stages 3 and 4) and, where possible, slowing the progression of disease (especially in CKD stages 2 and 3). Although beyond the scope of these Guidelines, careful evaluation of cats (as outlined earlier) should also allow identification of certain underlying aetiologies that permit specific intervention such as renal lymphoma, UTIs, nephroliths and ureteroliths.
Because of the chronic nature of the disease, the need for regular monitoring and the potential for various interventions, establishing a good relationship and good communication between the clinic and the cat’s owner is vital. This will facilitate individualised management plans to be created that take into consideration the wishes and ability of the owner, as well as the needs of the cat.
Issues that should be considered are outlined in the box below.

Management of CKD patients
Managing hydration in CKD46,47

CKD is associated with variable obligatory diuresis, and affected cats may be predisposed to dehydration, especially in CKD stages 3 and 4.

Correcting dehydration46,47
Cats with unstable or decompensated CKD may require hospitalisation and intravenous fluid therapy, typically with lactated Ringer’s solution or Hartmann’s. Consideration should also be given to concomitant electrolyte and acid–base disturbances that may need addressing.
The fluid required to correct dehydration (in ml) is calculated from: body weight (kg) × estimated dehydration (%) × 1000, and this (along with maintenance fluids, eg, 50 ml/kg/24 h) is typically provided over 24–48 h, although some cats may tolerate more rapid rehydration.
After rehydration, maintenance fluids can be administered but cats should be monitored carefully to avoid fluid overload. When azotaemia is stable, fluids should be tapered over 2–3 days before the patient is discharged.
Long-term maintenance of hydration

Multiple sources of fresh water are important for maintaining hydration. Courtesy of Jessica Quimby

Subcutaneous fluid therapy can be used on an outpatient basis or by owners at home. Courtesy of Sarah Caney
Although a balanced electrolyte solution such as lactated Ringer’s solution is often used, a hypotonic solution (half-strength lactated Ringer’s or 0.45% saline, with added potassium as needed) may be preferable to reduce the sodium load. Fluids can be administered via a needle and giving set, or through an indwelling subcutaneous catheter, although there is the risk of the latter becoming blocked or infected.
Managing diet and mineral/bone disease in CKD
Dietary manipulation is a mainstay of CKD therapy in human 50 and veterinary patients. Renal formulated diets are restricted in both protein and phosphorus, but other features include an increased calorie density, sodium restriction, potassium supplementation, alkalinisation, and supplementation with B vitamins, antioxidants and omega-3 fatty acids.
Protein and phosphate restriction

Protein restriction and phosphate restriction are considered together as they are the main features of commercial renal diets, and are thought to confer the major benefits seen. Feline renal diets typically contain 6–7 g of protein per 100 kcal (above the 5 g/100 kcal recommended allowance for adult cats, 51 but below the 9–10 g/100 kcal commonly seen in maintenance diets). Energy requirements of older (>13 years) cats may increase and severe protein restriction may lead to loss of lean tissue; 52 thus moderate protein restriction is recommended in CKD, together with monitoring of lean body mass, weight and caloric intake (Figure 10). In addition to protein restriction, renal diets contain much less phosphate compared with typical maintenance diets.53,54

Muscle wasting and dehydration in a cat with CKD. Careful attention to body condition, muscle mass and caloric intake is important. Courtesy of Jessica Quimby
In cats with CKD, renal diets have been shown to reduce clinical signs of uraemia,55 –57 and to significantly prolong longevity (see Table 3), providing a strong rationale for their use.
Studies evaluating effect of renal diets on longevity

Differentiating the effects of protein and phosphate restriction is complex and not always possible, but while moderate protein restriction is thought to help reduce signs of uraemia, there is little evidence that this alone has a major effect on progression of CKD.58 –60 Conversely, hyperphosphataemia is known to be associated with progression of CKD,42,44,45 and phosphate restriction may reduce the severity of renal pathology in CKD;53,61 thus phosphate restriction is thought to be mainly responsible for the improved longevity seen. Furthermore, renal secondary hyperparathyroidism (which may contribute to uraemia and disease progression) can be seen prior to the development of overt hyperphosphataemia or azotaemia, 34 and phosphorus-restricted diets reduce hyperphosphataemia, hyperparathyroidism and FGF-23 (which may indirectly promote hyperparathyroidism).55 –57,62,63

Changing and transitioning diets
Renal diets are generally less palatable than maintenance diets (probably at least partially due to their lower protein content). This can lead to poor acceptance of these diets,24,65 a problem that may be exacerbated by inappetence in cats with more advanced CKD.
Use of phosphate binders

As CKD progresses, serum phosphate tends to increase and may become more refractory to control with dietary phosphate restriction. Where diet alone is insufficient, the use of intestinal phosphate binders is important. Several agents can be used for this purpose (see Table 4).53,67 –69 There are no studies comparing different phosphate binders in cats with CKD, but all are likely to be efficacious. 53 Offering alternative binders when needed may be appropriate, as palatability of the phosphate binders varies.69,70 If calcium-containing phosphate binders are used, monitoring of serum calcium (ideally ionised) is recommended, as hypercalcaemia is occasionally seen as an adverse event. 53
Some common oral phosphate binders used in cats

For all phosphate binders, it is important to split the daily dose and give it mixed with food or at the same time that the cat eats. Doses may have to be increased to achieve the desired effect

Where cats cannot be transitioned to a commercial or home-prepared renal diet with restricted phosphate, phosphate binders can be used with a maintenance diet, but their efficacy is likely to be compromised by the quantity of phosphate in the diet.

Managing serum calcium
Hypercalcaemia is a recognised cause of renal injury, but CKD can also cause changes in serum calcium, although these are generally mild. Ionised hypocalcaemia appears to be most common, and tends to be seen in advanced CKD. 72 An increased calcium–phosphorus product has been linked with disease severity in cats. 73

Calcitriol therapy

Calcitriol (active vitamin D) deficiency may occur with CKD due to various mechanisms including hyperphosphataemia-mediated inhibition of hydroxylation and loss of renal tissue. Calcitriol supplementation can potentially help suppress renal secondary hyperparathyroidism and has been shown to be beneficial in dogs and humans; 74 but despite anecdotal reports of improved QoL, low dose calcitriol has not been shown to have the same benefits in feline CKD. 75 Additionally, formulations of calcitriol can make accurate dosing difficult in cats. Hyperphosphataemia should also be carefully controlled when using this therapy to avoid increasing the serum calcium–phosphate product.

Managing potassium

Feline CKD can lead to excessive kaliuresis, which may be compounded by reduced potassium intake, vomiting and transcellular shifts.55,76 Hypokalaemia may cause or contribute to clinical signs such as lethargy, inappetence, constipation and muscle weakness, and may contribute to development of acidosis, but has not been identified as a risk factor for disease progression or outcome.42,44,45
Although renal diets are typically supplemented with potassium, hypokalaemia may still be seen in some cats. Conversely, hyperkalaemia may occasionally be seen in advanced CKD.

Managing acid–base balance

Metabolic acidosis is multifactorial in CKD 77 and bicarbonate therapy has been shown to improve nutrition (calorie and protein intake, lean body mass) and slow progression in humans with CKD. 78 Metabolic acidosis has been reported to occur in over half of cats with advanced (stage 4) CKD.79,80 However, cats fed commercial renal diets may have higher serum bicarbonate concentrations. 56

Other nutrients

One retrospective study suggested that renal diets with the highest omega-3 fatty acid content were associated with the longest survival times. 54 However, a causal relationship could not be established, and feeding a renal diet may not alter fatty acid profiles. 81
Dietary sodium restriction is recommended for people with CKD to mitigate hypertension and other effects, 82 but evidence for a beneficial effect in older cats, with and without CKD, is generally lacking, and very restricted sodium intake may be deleterious.83 –86
Cats with CKD have evidence of increased oxidative stress compared with healthy cats,87,88 and dietary antioxidant therapy (with vitamins E, C and beta-carotene) may reduce this. 89 Whether this results in any renoprotective effect remains to be determined.
Other dietary supplements, including Chinese rhubarb (Rheum officinale) and a prebiotic/probiotic combination, have not shown any beneficial effects.90,91

Managing hypertension in CKD

Systemic hypertension associated with CKD has a reported prevalence of 19–40% in primary care practices,36,92 and as high as 65% in referral populations. 93 The pathogenesis is not entirely clear, with some cats demonstrating activation of the renin–angiotensin–aldosterone system (RAAS),94 –96 and some having apparent autonomous hyperaldosteronism.96,97
Doppler and high-definition oscillometry are the most reliable non-invasive blood pressure measurement techniques in conscious cats.98 –105 However, even when cats are calm, and a standardised protocol is followed, 105 measurements will vary with the equipment, the operator, the cat and the circumstances.36,106 –111 Current non-invasive techniques are inaccurate for assessing diastolic blood pressure in cats.101,104
Within these limitations, hypertension is usually defined as an SBP persistently >160–180 mmHg,36,112 but has also been defined according to the perceived risk of target organ damage (TOD) (see box on page 221 and Table 5).27,105 Target organs are those particularly susceptible to hypertensive damage – the eyes,93,107,113 heart,114 –116 cerebrovascular tissue113,117 and kidneys. While hypertension is an independent risk factor for progressive CKD in dogs and people,118,119 this has not been proven in cats.37,116,117,120 However, hypertension is associated with the severity of proteinuria (as in people and dogs),37,120 –122 which can be reduced with successful antihypertensive therapy.37,120,123

SBP = systolic blood pressure
Management of hypertension is aimed at preventing TOD, although the current perceived risk categories (Table 5) are imprecise as data are lacking, risks may vary between individuals and may, for example, depend on how rapidly blood pressure rises. In general, treatment aims to reduce SBP to <150–160 mmHg.27,105
Monotherapy with angiotensin-converting enzyme inhibitors (ACEIs) or atenolol is not effective in most hypertensive cats.95,105,112,124,125 There is some experimental data to suggest the ARB telmisartan at 3 mg/kg q24h may be more effective than benazepril as an anti-hypertensive agent, 126 but further clinical studies are needed. Conversely, the calcium channel blocker amlodipine is an effective monotherapy for most (but not all) cats,97,112,113,115,120,127,128 and may be combined with other drugs if adjuvant therapy is needed (Table 6).

Suggested oral therapy for systemic hypertension

ARB = angiotensin receptor blocker; ACEI = angiotensin-converting enzyme inhibitor
Managing anaemia in CKD

Anaemia of varying severity is seen in 30–65% of cats with CKD 38 (Figure 11). A relative lack of erythropoietin (EPO) in CKD produces a non- or poorly-regenerative anaemia, which may be exacerbated by blood loss and/or shortened red blood cell (RBC) survival. 129 Anaemia has been identified as a dependent or independent risk factor for progression of CKD,42 –45 and there is evidence that treatment with erythrocyte-stimulating agents (ESAs) may improve QoL and potentially survival in some cats with CKD. 129

Anaemia is a recognised risk factor for progression of CKD. Courtesy of Cathy Langston

Enteral (oesophagostomy) tube in place to support food and fluid intake. Courtesy of Isuru Gajanayake
Blood transfusions and haemoglobin-based oxygen carrying solutions (eg, Oxyglobin; Dechra Veterinary Products) have limited value for the chronic anaemia associated with CKD,130,131 and the use of anabolic steroids is not recommended due to lack of evidence of efficacy and potential adverse events.132,133 In contrast, the use of ESAs (EPO or EPO analogues) has become the standard of care in human medicine.
ESA therapy is designed to elevate the packed cell volume (PCV) to around the lower limit of the reference interval – sufficient to meet tissue oxygen demand. Iron supplementation alone is not effective in managing CKD-associated anaemia, but it enhances the efficacy of ESA therapy in humans, 134 and anecdotal evidence suggests the same is true in cats.
The two ESAs most widely used in cats are recombinant human epoetin alfa (EA, ~80% homology to feline EPO) and darbepoetin alfa (DA, a hyperglycosylated recombinant human EPO analogue). Although often successful, in one study, >40% of cats with CKD-associated anaemia failed to respond or failed to develop a sustained response to ESA therapy. 135 Potential reasons for this include:129,135
Concurrent illnesses (present in most cats that fail to respond to ESA);
Infections or inflammation;
Gastrointestinal bleeding;
Iron deficiency;
Pure red cell aplasia (PRCA) from production of anti-EPO antibodies (Table 7).
Clinical use of human epoetin alfa or darbepoetin alfa in cats with CKD

Anti-erythropoeitin antibodies are produced and PRCA manifests as worsening anaemia, lack of erythrocytosis, and no response to ESA therapy. Diagnosis is supported by a bone marrow aspirate/core and cats become transfusion-dependent for months. 137 SC = subcutaneously; PCV = packed cell volume; PRCA = pure red cell aplasia
Hypertension is also recognised as an adverse effect of ESA therapy, affecting up to 50% of treated cats.129,135

Managing proteinuria in CKD

In human medicine, regardless of the cause of CKD, the severity of proteinuria at the time of diagnosis is an important prognostic indicator, and controlling proteinuria results in slower progression of CKD, largely irrespective of the underlying cause of the CKD. 138 CKD is generally associated with increased intraglomerular capillary pressure and other changes that impair glomerular permselectivity, leading to increased loss of albumin (and other proteins) into tubular fluid; this appears to directly contribute to disease progression by promoting tubular inflammation and fibrosis. 138
Although there may be species differences in pathophysiology, increased proteinuria in cats with CKD (assessed with UPCR and not routine dipsticks, which are inappropriate for assessment of feline proteinuria139,140) is also known to carry a poorer prognosis.37,42,44,120,123 In one study, 37 cats with a UPCR <0.2 were reported to have a median survival time of ~1000 days compared with ~500 days for those with a UPCR of 0.2–0.4, and ~400 days for those with a UPCR >0.4. Very similar findings have also been reported elsewhere. 120 Currently, there is no evidence that measurement of UACR rather than UPCR offers any benefits in cats,37,141 but the urinary proteome in healthy cats and cats with CKD is complex and more studies are needed.142 –146
In humans, treatment with angiotensin receptor blockers (ARBs) or ACEIs is effective in blocking RAAS activation, decreasing glomerular capillary pressure, restoring glomerular permselectivity, reducing proteinuria and slowing the progression of CKD.138,147 –149 These effects are partly as a result of haemodynamic changes and partly through modifying non-haemodynamic remodelling in the kidney. 150
The existing IRIS 27 CKD (see box on page 221) and American College of Veterinary Internal Medicine (ACVIM) proteinuria 151 guidelines suggest cats should be classified as:
Overtly proteinuric: UPCR >0.4
Borderline proteinuric: UPCR 0.2–0.4
Non-proteinuric: UPCR <0.2
Using these criteria, around 50–66% of cats with CKD are likely to be non-proteinuric and around 20% overtly proteinuric.37,42
In cats with CKD, RAAS inhibition with the ACEI benazepril has been shown to significantly reduce the severity of proteinuria.152 –154 More recently, the ARB telmisartan has been licensed in some countries for the management of proteinuric feline CKD. In a large multicentre European study of telmisartan in cats with naturally occurring CKD it was shown to significantly decrease proteinuria at all time points during the 6 months of the study. 155 However, a survival benefit from RAAS blockade in cats has not been demonstrated.152,153 The reasons for the lack of effect on survival are uncertain but may include:
Underpowered clinical trials;
Inadequate duration of clinical trials;
Differences in the pathophysiology between humans and cats with CKD (eg, proteinuria could be a marker of tubular dysfunction in cats rather than a cause of progressive disease);
Differences in the prevalence or severity of proteinuria between humans and cats with CKD;
Inadequate control of proteinuria and/or inappropriate targets for antiproteinuric therapy (while benazepril therapy significantly reduced UPCR in CKD cats compared with placebo in clinical trials, these studies also showed little overall reduction in the UPCR from baseline values within the treatment group152,153).
Further investigations are needed to assess the role of RAAS inhibition in feline CKD and to determine optimal therapy, but currently both ARBs and ACEIs are available and used in cats, and are licensed in some countries (Table 8). There is some (weak) evidence that RAAS blockade may have more beneficial effects (possibly on survival, QoL and appetite) in CKD cats with more severe proteinuria (eg, UPCR ⩾1.0), 152 and currently IRIS and ACVIM guidelines71,151 suggest antiproteinuric therapy should be instituted in CKD cats with a UPCR >0.4.
Suggested oral therapy for managing proteinuria

ARB = angiotensin receptor blocker;
ACEI = angiotensin-converting enzyme inhibitor

Managing inappetence, nausea and vomiting in CKD

Cats with CKD can suffer from nausea, vomiting and inappetence as a result of uraemic toxins affecting the central chemoreceptor trigger zone. Inappetence is a significant QoL concern for owners, 156 and in the CKD patient could result in protein and calorie malnutrition with its many adverse consequences. 157 A reduced appetite should therefore be actively managed, along with complications of CKD that can contribute to inappetence, such as dehydration, hypokalaemia, acidosis and anaemia. Centrally acting antiemetics such as maropitant, mirtazapine, ondansetron and dolasetron158 –160 should be considered for management (Table 9). In placebo-controlled trials of cats with stage 2 or 3 CKD, maropitant (given orally for 2 weeks) was shown to reduce vomiting, 160 and mirtazapine (given orally for 3 weeks) reduced vomiting and also increased appetite and weight. 158 Mirtazapine may therefore be a useful adjunct to the nutritional management of cats with CKD.
Suggested therapy for managing inappetence, nausea and vomiting

SC = subcutaneously; IV = intravenously; PO = orally
There are anecdotal reports of H2 blockers or proton pump inhibitors alleviating inappetence in some feline CKD patients, but the presence and degree of gastric hyperacidity and efficacy of these medications remain unproven. Additionally, although hypergastrinaemia has been reported in feline CKD, 161 gastric ulceration has generally not been observed or reported.73,162 If therapy for hyperacidity in cats is considered, omeprazole appears to be superior to famotidine. 163

Managing UTIs in CKD

Bacterial UTIs in cats with CKD occur at a reported frequency of around 15–30%,39,164 –166 with older female cats having an increased risk. 39
Most (>70%) of these UTIs appear to be subclinical (ie, without lower urinary tract signs [LUTS]), although >85% show changes on urine sediment analysis (>5 white blood cells [WBCs]/hpf, and/or >5 RBCs/hpf, and/or microscopic bacteriuria). 39 Escherichia coli represents 60–75% of isolates, while other organisms include Enterococcus, Streptococcus, Staphylococcus, Enterobacter, Pseudomonas and Klebsiella species.
The presence of LUTS or detection of pyuria (⩾5 WBCs/hpf) in routine urinalysis of CKD patients are indications for bacterial culture of a cystocentesis sample, but whether routine culture of all urine samples should be recommended is controversial, as the significance of subclinical bacteriuria is uncertain. While some clinicians advocate routine treatment of all CKD-associated UTIs (as cats may be at risk for pyelonephritis and deterioration of CKD), recurrent or recrudescent UTIs are common after treatment, 39 the presence of subclinical UTIs has not been associated with disease severity or apparent survival, 39 and unnecessary treatment may risk development of bacterial resistance.
When treated, UTIs should be managed according to international guidelines, 167 selecting antibacterials based on sensitivity testing (note that boric acid tubes should be avoided for urine cultures 168 ) that are excreted unchanged in urine and have a wide therapeutic index (Table 10). If initial empirical therapy is needed, amoxicillin (11–15 mg/kg PO q8h) 167 or potentiated amoxicillin 169 are appropriate choices; 2–4 weeks’ therapy has been recommended, 167 although optimum duration of therapy for CKD-associated UTIs is uncertain. 170 Response to treatment should be monitored with repeat culture 7 days after cessation of treatment.
Considerations when selecting an antibacterial to treat urinary tract infections in cats with CKD

Some cephalosporins accumulate in renal tubular cells and can cause damage
Avoid enrofloxacin in cats with CKD due to increased risk of retinopathy at standard therapeutic doses
Water soluble tetracyclines (eg, oxytetracycline) depend partly on renal excretion. Tetracyclines also increase protein catabolism, and breakdown products of oxytetracycline have been shown to be nephrotoxic
IRIS = International Renal Interest Society

Other treatments
Anabolic steroids
Information regarding the efficacy of anabolic steroids for cats with CKD is lacking and, as hepatotoxicity has been reported, 133 their use is not currently recommended.
Stem cell therapy
Pilot studies investigating stem cell therapy for feline CKD have not to date demonstrated beneficial effects; and with some techniques adverse effects occur.171,172 Consequently, this treatment is not currently recommended.
Renal transplantation
Kidney transplants from living donors may be available to treat cats with CKD at specialist centres in some regions. This procedure has numerous implications including ethical, financial, welfare and monitoring considerations.173 –176 While it may be viable in some patients, kidney transplantation is beyond the scope of these Guidelines.
Dialysis therapy
Haemodialysis or peritoneal dialysis are techniques that can be successfully applied to cats, although complications may arise. Their main indications are for management of acute kidney injury or acute on chronic kidney disease.177,178


Footnotes
Funding
These Guidelines were supported by an educational grant from Boehringer Ingelheim to the ISFM.
Conflict of interest
Jonathan Elliott has acted as a paid consultant for CEVA Animal Health, Boehringer Ingelheim, Pfizer (now Zoetis), Bayer, Idexx, Novartis Animal Health, Waltham Centre for Pet Nutrition and Royal Canin; he has research grant funding and contracts to work on kidney disease in cats from CEVA Animal Health, Orion, Zoetis, Royal Canin and Novartis Animal Health (now Elanco Animal Health). Natalie Finch has received research funding from Boehringer Ingelheim. Catherine Langston is a paid consultant for Bayer and for Abaxis. Hervé Lefebvre has received grants/research contracts and/or performs consulting for Royal Canin, Novartis Animal Health, CEVA Animal Health and Bayer.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.