
Abstract
Objectives
Diagnosis of feline infectious peritonitis (FIP) remains challenging, especially in cats without effusions. The objective of this study was to evaluate the sensitivity and specificity of a real-time reverse transcriptase polymerase chain reaction (RT-PCR) detecting feline coronavirus (FCoV) RNA in peripheral blood mononuclear cells (PBMCs) and serum in comparison with the same real-time RT-PCR in cell-free body cavity effusion.
Methods
This prospective case-control study included 92 cats. Forty-three cats had a definitive diagnosis of FIP, established either by histopathological examination (n = 28) or by positive immunofluorescence staining of FCoV antigen in macrophages of effusions (n = 11), or by both methods (n = 4). Forty-nine control cats had other diseases but similar clinical signs. Real-time RT-PCR was performed on PBMCs of 37 cats (21 cats with FIP, 16 controls), on serum of 51 cats (26 cats with FIP, 25 controls) and on cell-free body cavity effusion of 69 cats (36 cats with FIP, 33 controls). Sensitivity, specificity, positive and negative predictive value, including 95% confidence intervals (CI), were calculated.
Results
Real-time RT-PCR of PBMCs, serum and cell-free body cavity effusion showed a specificity of 100% (95% CI 79.4–100% in PBMCs, 86.3–100% in serum, 89.4–100% in cell-free body cavity effusion) and a sensitivity of 28.6% (95% CI 11.3–52.2%) in PBMCs, 15.4% (95% CI 4.4–34.9%) in serum and 88.9% (95% CI 73.9–96.9%) in cell-free body cavity effusion to diagnose FIP.
Conclusions and relevance
Although it is known that RT-PCR can often provide false-positive results in healthy cats, this real-time RT-PCR was shown to be a specific tool for the diagnosis of FIP when applied in a clinical setting. Sensitivity in cell-free body cavity effusion was high but low in PBMCs and serum. PBMC samples showed a higher sensitivity than serum samples, and are therefore a better choice if no effusion is present.
Introduction
Feline infectious peritonitis (FIP) is a common disease and a major cause of death in young cats.1,2 Feline coronavirus (FCoV) infections occur frequently in the cat population worldwide.3–6 Despite the high prevalence of FCoV infection, only some infected cats develop FIP. 7 The change from the harmless enteric biotype (feline enteric coronavirus) into the pathogenic variant (feline infectious peritonitis virus) is due to mutations of the virus.8–11 The mutations cause a change in enterocyte to macrophage tropism with the ability to infect and effectively replicate within cells of the macrophage lineage.2,12 The latter is regarded as the key event in the pathogenesis of FIP.13,14 Various genes, including 7b, 3c and S, are thought to be associated with virulent mutations and the change of tissue tropism.8,10,11,15–18
A definitive diagnosis of FIP ante-mortem remains challenging. If no effusion is present, organ biopsy is necessary for a definitive diagnosis. 19 As the median survival time of cats with FIP is only a few days,20,21 and the diagnosis of FIP commonly leads to euthanasia, a highly specific diagnostic tool is necessary to confirm the diagnosis. Different reverse transcriptase polymerase chain reaction (RT-PCR) protocols are used to diagnose FIP, but for most of them sensitivity and specificity are rather low.19,22–25 Most studies have used serum or plasma and found a very low sensitivity. Using whole blood was associated with a slightly better sensitivity but a lower specificity.26,27 However, the sensitivity of RT-PCR in body cavity effusion seems to be higher, but this has not been investigated in controlled studies involving large numbers of cats.10,19
The aim of the present study was to investigate and compare the sensitivity and specificity of a real-time RT-PCR in peripheral blood mononuclear cells (PBMCs), serum and cell-free body cavity effusion in cats with confirmed FIP and cats with confirmed diseases other than FIP but with similar clinical signs.
Materials and methods
Animals
This study was designed as a case-control study and included 92 cats. The cats were presented to the Clinic of Small Animal Internal Medicine, LMU University of Munich, Germany (n = 80) or to private veterinarians (n = 12). The case group (n = 43) included cats with a definitive diagnosis of FIP (Table 1). FIP diagnosis was confirmed by typical morphology in histopathological examination (surface-bound multi-systemic pyogranulomatous and fibrinonecrotic disease with venulitis with or without high-protein exudate) in 28/43 cats. In 11/43 cats, FIP diagnosis was established ante-mortem by positive immunofluorescent staining of FCoV antigen in macrophages of thoracic or abdominal effusions;19,28 in 4/43 cats, FIP was confirmed by both methods.
Clinical presentation of cats with feline infectious peritonitis, number of positive samples in peripheral blood mononuclear cells (PBMCs), serum and cell-free body cavity effusion, and mean threshold cycle (Ct) values of positive samples
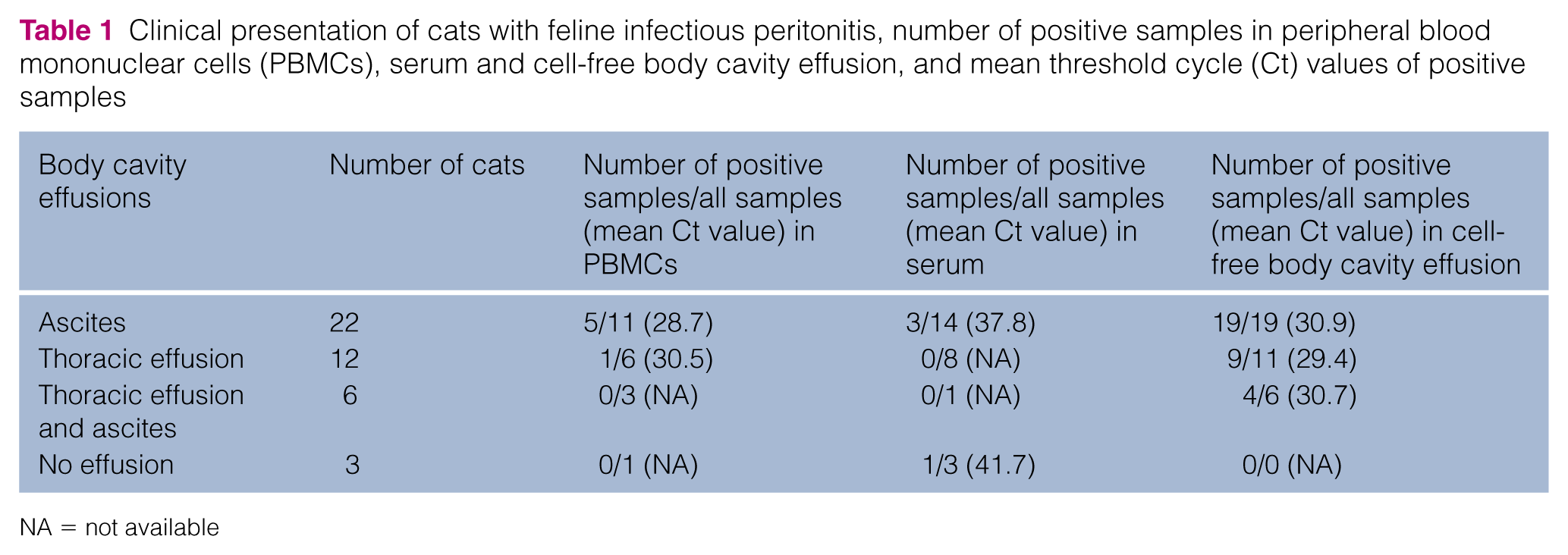
NA = not available
The control group (n = 49) was defined as a population of cats in which a veterinarian would consider FIP as a differential diagnosis. Only cats with one or more of the following signs were included: body cavity effusion, rectal temperature ⩾40 °C (with ⩽20,000 white blood cells/µl and ⩽1000 banded neutrophils/µl), icterus, ocular signs and neurological signs. Cats were included in the control group if they were definitively diagnosed with diseases other than FIP that explained the clinical signs. Most of the cats of the control group suffered from neoplasia (n = 20), followed by decompensated cardiac diseases (n = 13) and inflammatory diseases (n = 6), such as pancreatitis and cholangiohepatitis or bacterial peritonitis and pleuritis (Table 2). Two cats had hepatolipidosis, one with hepatoencephalic syndrome. The remaining eight cats suffered from various diseases. One cat had an aneurysm of the portal vein with thrombus formation leading to portal hypertension and ascites. One cat had fever of unknown origin, which was self-limiting after 3 days. One cat had a pulmonary fibrosis with thoracic effusion. One cat had chronic thoracic chylous effusion of unknown origin and secondary fibroplastic pleuritis. In one cat, an end-stage kidney disease caused effusion, likely due to hypervolaemia. In one cat, an acute kidney injury caused effusion, likely due to vasculitis. Urine leakage was associated with an obstructive feline lower urinary tract disease (FLUTD) in one cat. In a cat with eosinophilic enteritis with protein-losing enteropathy, the ascites was likely due to a low oncotic pressure.
Diseases of the cats of the control group, clinical presentation and the number of tested samples

Fever with ⩽20,000 white blood cells/µl and ⩽1000 banded neutrophils/µl
The diseases of the cats of the control group (n = 49) were definitively confirmed ante-mortem (n = 23), or at necropsy with histopathological examination (n = 18), or by a survival time of at least 1 year after sampling (n = 8). Ante-mortem diagnosis was established by echocardiography for cardiac diseases (n = 13), cytology or histology for neoplasia (n = 8), cytology and bacterial culture of effusion for bacterial pleuritis (n = 1), and history and physical examination for urine leakage in association with obstructive FLUTD (n = 1). The cats with a survival time of at least 1 year after sampling were included because the average survival time of cats with FIP after the onset of clinical signs is between days and weeks.12,20,21 Consequently, cats with FIP are not expected to be alive after 1 year.
Sampling and RNA extraction of PBMCs
Whole blood samples (n = 37) were collected ante-mortem for diagnostic purposes. PBMCs were obtained from non-coagulated EDTA blood samples (21 cats with FIP, 16 cats with other diseases) within 24 h of sampling by applying the following process: 1 ml non-coagulated blood mixed with one volume of phosphate-buffered saline (PBS; Sigma-Aldrich) was used for density gradient centrifugation. The mixture was carefully added on top of 5 ml of a density gradient medium (NycoPrep 1.068; Progen Biotechnik) and centrifuged at 300 × g for 30 mins. PBMCs were collected and, after two washing steps with 10 ml PBS, centrifuged at 800 × g for 10 mins to get a fluid-free cell pellet.
Total RNA of the cell pellet was extracted using an RNeasy Mini Kit (Qiagen) following the manufacturer’s instructions. Briefly, cells were treated with a lysing buffer (buffer RLT) and homogenised using QIAshredder spin columns (Qiagen). The lysate was applied to RNeasy Mini spin columns. After two washing steps, RNA was eluted with 30 µl RNase-free water and stored at −80°C in a 1.5 ml Safe-Lock microcentrifuge tube (Eppendorf).
Sampling and RNA extraction of serum and body cavity effusion
Serum samples (26 cats with FIP and 25 cats with other diseases) and body cavity effusion samples (36 cats with FIP and 33 cats with other diseases) were obtained ante-mortem for diagnostic purposes. Ascitic and thoracic fluids were obtained with ultrasound guidance using a 19 or 21 G butterfly needle. Serum and the cell-free supernatant of centrifuged body cavity effusions were stored at −80°C in a 1.5 ml Safe-Lock microcentrifuge tube (Eppendorf).
Viral RNA was isolated from serum and cell-free body cavity effusion using a QIAamp Viral RNA Kit (Qiagen). Briefly, 140 µl aliquots of samples were lysed under highly denaturing conditions to inactivate RNases and isolate the intact viral RNA. Adjusted buffering conditions yielded an optimal binding of the viral RNA on the silica membrane of the QIAamp Mini spin column. After being washed with two wash buffers, the RNA was eluted with 60 µl RNase-free buffer and stored at −80°C in a 1.5 ml Safe-Lock microcentrifuge tube (Eppendorf).
Real-time RT-PCR
Detection of FCoV was performed using a real-time RT-PCR as described previously. 29 A real-time RT-PCR detecting β-actin messenger RNA (mRNA) 30 was used as an internal and extraction control. The QuantiTect Probe RT-PCR Kit (Qiagen) was used for the one-step real-time RT-PCR. RNA template (5 µl) was added to 12.5 µl Master Mix, 0.25 µl RT Mix, 5.25 µl RNase-free water and 2 µl primer probe mix. All primers were used in a concentration of 0.8 µM, and 5’FAM/3’BHQ-1-labelled TaqMan probes were used in a concentration of 0.3 µM. For β-actin mRNA, the PCR primer and probe concentrations were 0.2 µM and 0.1 µM, respectively. The following temperature profile was chosen: reverse transcription at 50°C for 30 mins, reverse transcriptase inactivation and polymerase activation at 95°C for 15 mins, 42 cycles of denaturation for 30 s at 95°C, and annealing and elongation for 60 s at 60°C. A Stratagene MX3005P was used for the fluorescence measurement.
Data analyses
Sensitivity and specificity as well as the positive (PPV) and negative predictive values (NPV) were calculated. Ninety-five percent confidence intervals (CI) were determined. Data analyses were performed using a two-sided Fisher’s exact test with Graph Pad Prism Version 5.0 and a significance threshold of 0.05.
Results
Overall, 157 samples were evaluated, including 83 samples from cats with FIP and 74 samples from control cats (Table 3). The sensitivity and specificity, as well as the PPV and NPV, are shown in Table 4. None of the samples that tested positive for FCoV RNA was false positive. Hence, the specificity was 100%. PBMCs had a sensitivity of 31.6%. The sensitivity of serum was 23.1%, and the sensitivity of cell-free body cavity effusion was 88.9%. Threshold cycle (Ct) values ranged between 25.8 and 41.7. Mean Ct values are given in Table 1.
Results of the real-time reverse transcriptase polymerase chain reaction in peripheral blood mononuclear cells (PBMCs), serum and cell-free body cavity effusion

Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the real-time reverse transcriptase polymerase chain reaction (real-time RT-PCR) in peripheral blood mononuclear cells (PBMCs), serum and cell-free body cavity effusion to diagnose feline infectious peritonitis (FIP) and the prevalence of FIP
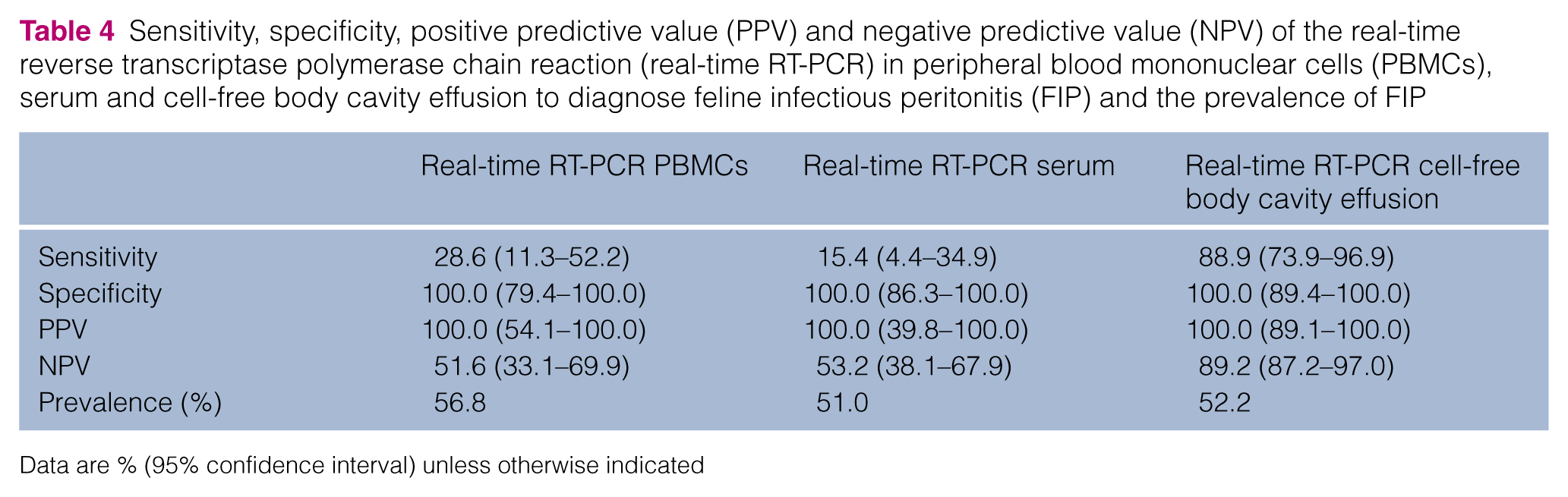
Data are % (95% confidence interval) unless otherwise indicated
Discussion
The aim of the study was to compare the diagnostic utility of a real-time RT-PCR in PBMCs, serum and cell-free body cavity effusion as diagnostic tool for FIP. The sensitivity of the present assay was relatively low in PBMCs (31.6%) and in serum (23.1%). This is in contrast to previous studies in which RT-PCR of blood had sensitivities ranging from 50% to 93%.19,22,24,26 It could be argued that these results were caused by a low analytical sensitivity of the PCR assay. However, sensitivity of the same real-time RT-PCR was much higher when testing cell-free body cavity effusion (88.9%) in the present study. RNA was isolated from the serum and cell-free body cavity effusion using the same method under identical conditions. Nevertheless, sensitivity of cell-free body cavity effusion was quite high and that of serum rather low. This indicates that the RNA extraction was adequate. Thus, the low sensitivity is likely due to a low virus concentration in blood samples. Sensitivity of PBMCs was higher than that of serum, which can be explained by the fact that the virus replicates intracellularly. This is in accordance to other studies, which had higher sensitivities when using PBMCs. 26 Therefore, PBMCs rather than serum should be recommended in the future. The higher sensitivity in cell-free body cavity effusion, in contrast to blood, could be explained by the close contact of body cavity effusion with the pyogranulomas and serosal surface of the abdominal viscera, which contain high virus concentrations. 12
Although an absolute quantification was not performed, the high Ct values, especially in serum, indicate a low viral load in the specimen. The mean Ct value of serum was 38.8. Ct values in PBMCs were lower than in serum, with a mean Ct value of PBMCs of 29.0, which supports the theory of intracellular replication causing higher viral loads in samples containing white blood cells in contrast to cell-free serum. The Ct values of cell-free effusion were in the same range as the Ct values of PBMCs, as the mean Ct value of cell-free body cavity effusion was 30.4. This indicates a high viral load in the cell-free supernatant of body cavity effusion, likely caused by the close contact of the ascites to pyogranulomas in the body cavities.
The specificity of the real-time RT-PCR used in this study was 100%, regardless of the material used; thus, this value was much higher than comparable values of previous studies investigating RT-PCR for the diagnosis of FIP.19,22,24,25 These previous studies have described RT-PCR specificities ranging between 20% and 90% for serum and plasma. Only one former study had a specificity of 100%, which however, used an mRNA RT-PCR. 26 The idea behind detecting for mRNA was to identify only the replicating virus. However, this impressively high specificity was not confirmed 2 years later, when Can-Sahna et al used an identical mRNA RT-PCR and found FCoV in 52% of healthy cats that came from multi-cat households or were stray cats from the same location. 27 Most of the former studies used healthy cats from catteries or shelters, in which the prevalence of FCoV infection is generally much higher than in single-cat households.4,31 One study used cats in the control group that were experimentally infected with non-pathogenic FCoV. 25 These cats, from catteries or that were experimentally infected, are often transiently viraemic, and FCoV can also be found in various organs in these cats, even without development of FIP.32,33 In the present study, only 5/35 cats (of which information was available) of the control group were derived from households with more than two cats. Therefore, the high specificity in the present study is probably due to the absence of circulating FCoV infection. Moreover, in the present study, the control group consisted of cats that were presented to veterinary institutions for various diseases leading to similar clinical signs to those of FIP. The chosen type of population mimics the real situation in which a clinician considers FIP as differential diagnosis. Such a control group is better suited to evaluate the clinical utility of a diagnostic test for FIP than a control group that includes the entire clinic population, healthy cats or cats infected experimentally with FCoV.
Furthermore, using a one-tube real-time RT-PCR system minimises the risk of carry-over contamination, which adds to the high specificity of the assay used in this study. 34
It has to be considered that the high specificity of the present study could potentially also be caused by the inclusion of cats in the FIP group that had false-positive immunofluorescence staining of FCoV antigen in macrophages. Based on a positive immunofluorescence staining, 10 cats without histopathological examination were assigned to the FIP group.19,28,35 Whereas this test was reported to have a specificity of 100% in earlier studies, a more recent study by Litster et al found a specificity of only 71.4%. 36 However, 8/10 cats (from the present study) that were included based only on a positive immunofluorescence staining were positive in the real-time RT-PCR performed in this study. It would be very unlikely that two tests would be false positive at the same time. However, even if the 10 cats were excluded, the sensitivity of the real-time RT-PCR would not differ much (29.4% in PBMCs of cats with histopathological examination vs 28.6% of all cats; 22.2% in serum of cats with histopathological examination vs 15.4% of all cats; and 88.9% in cell-free body cavity effusions of cats with histopathological examination vs 88.9% of all cats). Furthermore, the specificity would not differ, as it was 100% in all samples.
Another reason for the high specificity in the present study could be the use of cell-free effusion. It could be hypothesised that there might have been false-positive results if the cell pellet of body cavity effusion had been used, as a higher viral load is expected in the cell-containing fraction of a specimen. However, PBMCs did not lead to false-positive results in the present study. The sensitivity of cell-free body cavity effusion was quite high, and the Ct values were as low as the Ct values of PBMCs. Therefore, it can be assumed that cell-containing body cavity effusion would also not have lead to false-positive results.
The real-time RT-PCR of the present study used a well-conserved nucleotide region spanning the membrane–nucleocapsid gene junction for amplification and did not detect any of the mutations in various genes (7a, 7b, 3c, S) that have recently been discussed for biotype conversion of FCoV.9,10,14,15,17,29 Even if the real-time RT-PCR of the present study did not detect any of the published mutations, it still proved to be highly specific. Therefore, the real-time RT-PCR of the present study with a specificity of 100% can be considered a reliable tool for diagnosing FIP as long as there is no further information available about the different mutations that are supposed to be associated with the acquisition of FIP virulence. 2
One limitation of this study was that not all sample types were available from each cat. Consequently, the comparability of different sample types from the same cat was limited. Another limitation was the assignment of cats to the control group. Cats were assigned to the control group if a disease other than FIP was confirmed that explained the observed signs. The possibility that a cat in the control group suffered from both FIP and another disease cannot be excluded completely. However, the occurrence of such a coincidence is very unlikely as no false-positive PCR results were observed in the present study.
Conclusions
This study evaluated the sensitivity and specificity of a real-time RT-PCR in PBMCs, serum, and cell-free body cavity effusion. The study found an excellent specificity, indicating that this PCR is a valuable tool for the diagnosis of FIP. The sensitivity of PBMCs and serum was low, with that of PMBCs being higher than that of serum, indicating the use of PBMCs instead of serum or plasma for the diagnosis of FIP if no effusion samples are available. Real-time RT-PCR of cell-free body cavity effusion had a high sensitivity. Thus, body cavity effusion, if available, is the sample type of choice when diagnosing FIP.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Parts of the results of this study were presented at the 21st German Internal Medicine and Clinical Pathology Conference 2013 in Munich, Germany.