
Abstract
Objectives
Feline infectious peritonitis (FIP) is an important cause of death in the cat population worldwide. The ante-mortem diagnosis of FIP in clinical cases is still challenging. In cats without effusion, a definitive diagnosis can only be achieved post mortem or with invasive methods. The aim of this study was to evaluate the use of a combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach in the diagnosis of FIP, detecting mutations at two different nucleotide positions within the spike (S) gene.
Methods
The study population consisted of 64 cats with confirmed FIP and 63 cats in which FIP was initially suspected due to similar clinical or laboratory signs, but that were definitively diagnosed with another disease. Serum/plasma and/or effusion samples of these cats were examined for feline coronavirus (FCoV) RNA by RT-nPCR and, if positive, PCR products were sequenced for nucleotide transitions within the S gene.
Results
Specificity of RT-nPCR was 100% in all materials (95% confidence interval [CI] in serum/plasma 83.9–100.0; 95% CI in effusion 93.0–100.0). The specificity of the sequencing step could not be determined as none of the cats of the control group tested positive for FCoV RNA. Sensitivity of the ‘combined RT-nPCR and sequencing approach’ was 6.5% (95% CI 0.8–21.4) in serum/plasma and 65.3% (95% CI 50.4–78.3) in effusion.
Conclusions and relevance
A positive result is highly indicative of the presence of FIP, but as none of the control cats tested positive by RT-nPCR, it was not possible to confirm that the FCoV mutant described can only be found in cats with FIP. Further studies are necessary to evaluate the usefulness of the sequencing step including FCoV-RNA-positive cats with and without FIP. A negative result cannot be used to exclude the disease, especially when only serum/plasma samples are available.
Introduction
Feline infectious peritonitis (FIP) is a fatal immune-mediated disease caused by infection with feline coronavirus (FCoV) that occurs worldwide. 1 FCoV exists as two distinct biotypes, the feline enteric coronavirus (FECV) and the feline infectious peritonitis virus (FIPV).2,3 Whereas antibodies against FCoV are very common in the cat population and prevalence can be as high as 90% in multi-cat households, FIP occurs in only approximately 5–10% of the FCoV-infected cats in multi-cat households.4–8 Regarding FIP pathogenesis, two different theories have been proposed. The ‘circulating virulent and avirulent hypothesis’ assumes that virulent and avirulent FCoV strains coexist within the cat population.9,10 However, there is increasing evidence that FIP develops after spontaneous mutations of the genome of apathogenic FCoV within infected cats, which is referred to as the ‘in vivo mutation hypothesis’.11,12 These mutations allow for sustained virus replication in macrophages, 13 which is regarded as a key event in the pathogenesis of FIP.14,15
Several genes, including spike (S), 7a, 7b and 3c genes have been discussed as sites for the mutations that are crucial for the pathotypic switch and changes in replication capacities in different cells.11,15–23 In contrast to previous studies, in which none of the sequence changes appeared to be consistently associated with the virulent FIPV variant, a recent study found nucleotide differences in two regions in close proximity in the S gene (nucleotide 23531 and nucleotide 23537), that resulted in amino acid variations in the putative fusion peptide. These two mutations were correlated with the FIP phenotype in >95% of cases. 24 Considering the importance of the coronavirus S protein fusion peptide in cell entry, 25 these findings could reasonably explain the alteration in viral tropism. It was also shown that substitutions in a furin cleavage site within the S protein of FCoV can be detected in cats with confirmed FIP, which are likely leading to a modulation of proteolytic cleavage, thereby enhancing virus uptake in macrophages. 26 However, systemic FCoVs with the above-mentioned spike gene mutations have been shown to occur also in cats without FIP.24,27
Once the clinical disease FIP develops, it always leads to death within a few days or weeks, and there is no effective therapy available.28,29 Therefore, a definitive diagnosis ante-mortem is essential but often challenging. Presently, necropsy or immunostaining of FCoV antigen in effusion or tissue lesions obtained by laparotomy are considered the gold standard for the diagnosis of FIP.6,30,31 Immunostaining of fine-needle aspirations of lymph nodes or affected organs is also possible, but diagnostic sensitivity is very low. 32 Thus, in cats without effusion, the definitive diagnosis can only be achieved with invasive laparotomy and biopsies of multiple organs, or might not be possible at all.
Several studies investigated the value of reverse transcriptase polymerase chain reaction (RT-PCR) in the diagnosis of FIP; however, the detection of FCoV RNA does not allow for differentiation between the virulent FIPV and avirulent FECV variant. Thus, conventional RT-PCR is also commonly positive in healthy cats that never will develop FIP.33–39 Detection of the mutated virus, however, could potentially be used to confirm the diagnosis ante-mortem.
Therefore, it was the aim of this study to evaluate the sensitivity and specificity of a combined approach using RT nested PCR (RT-nPCR) followed by sequencing, to detect two previously described mutations in the FCoV S gene in serum/plasma and effusion of cats suspected of having FIP. 24 The combined approach was evaluated in cats with confirmed FIP and a defined control group of cats for which FIP was considered an important differential diagnosis by the clinician, thereby mimicking the real-life clinical situation. It was hypothesised that the combined RT-nPCR and sequencing approach, as it has recently become commercially available to veterinarians, would be a new non-invasive and reliable method to diagnose FIP definitively.
Materials and methods
Animals
Initially, 152 cats were included in the study. However, in 25 of these cats no definitive diagnosis was established and thus these 25 cats were excluded retrospectively. Consequently, the data of 127 cats with signs indicative of FIP, for which a conclusive diagnosis of either FIP or other diseases could be established, were included in the evaluation of sensitivity and specificity (Figure 1). Samples of all cats were investigated by RT-nPCR and sequencing by a person blinded to all data of the cats. Cats were presented either as patients of the Clinic of Small Animal Medicine (n = 101) or directly submitted for necropsy (n = 26) to the Institute of Veterinary Pathology, Ludwig-Maximilians-University Munich, Germany. According to their diagnoses, cats were categorised either in the FIP group or in the control group.

Flowchart illustrating total number of cats included in the study, available samples and results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach. *In one cat, both a thymine (T [mutated]) and an adenine (A [non-mutated]) could be detected at position 23531. †In one cat, serum and effusion were tested positive by RT-nPCR and sequencing revealed two different mutations. FIP = feline infectious peritonitis
The FIP group (n = 64) consisted of cats with a definitive diagnosis of FIP (Table 1), established either by histopathology (n = 25), by histopathology plus immunohistochemical staining of FCoV antigen in tissue samples obtained at necropsy (n = 28)40,41 or by a positive immunofluorescence staining of FCoV antigen in macrophages of effusions (n = 11).34,42,43 In the cats with histopathological confirmation, diagnosis of FIP was achieved based on the occurrence of effusions and/or yellow to white foci or nodules in different organs plus the presence of typical histological lesions, including plasmacellular perivasculitis and/or accumulation of plasma cells with a necro-purulent centre. Typical lesions consisted of an arteriole or venule surrounded by a central area of necrosis that, in turn, was surrounded by proliferation macrophages and lymphocytes, plasma cells and neutrophils. 44
Inclusion criteria, method of confirmation of diagnosis, available samples and results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach for cats of the feline infectious peritonitis (FIP) group

ND = not determined; T = thymine; FCoV = feline coronavirus; G = guanine; C = cytosine; A = adenine
Cats were included in the control group (n = 63) if clinicians suspected FIP due to one or more of the following signs consistent with FIP: effusion (n = 59), fever with ⩽20,000 white blood cells/µl and ⩽1000 banded neutrophils/µl (n = 2), icterus (n = 6), neurological signs (n = 5) or hyperglobulinaemia (n = 1) (see Table 2). Some cats showed several of these signs. Control cats were only included if they were definitively diagnosed with a disease other than FIP that explained the clinical signs (Table 2). These other diseases were confirmed either by full post-mortem examination, including histopathology (n = 28), by histopathology of organ samples obtained either post mortem (n = 1) or in laparotomy (n = 2), by cytology and bacterial culture diagnosing bacterial pleuritis or peritonitis (n = 2), by echocardiography, which identified decompensated cardiac disease explaining pleural or abdominal effusion (n = 16), or by cytology diagnosing neoplasia (n = 12). In addition, cats (n = 2) that survived >3 years after the beginning of the clinical signs listed above were included in the control group.
Inclusion criteria, definitive diagnosis, method of confirmation of diagnosis, available samples and results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach for cats of the control group

ND = not determined
Samples
In total, 53 serum/plasma samples and 101 effusion samples were collected between 2009 and 2014. Blood was either stored as plasma (n = 14; 10 cats with FIP, four control cats) at −80 °C in a 2 ml low-temperature freezer vial (VWR International) until assayed or as serum (n = 39; 22 cats with FIP, 17 control cats) at −20 °C in a 1.5 ml Eppendorf Safe-Lock microcentrifuge tube until assayed. Effusion was collected (54 ascites, 46 pleural effusions, one pericardial effusion) and stored at −80 °C in 55 cats (28 with FIP, 27 controls) or at −20 °C in 46 cats (22 with FIP, 24 controls) (Figure 1). All samples collected ante-mortem were originally obtained for diagnostic and, in the case of effusion, therapeutic purposes.
PCR
Nucleic acid was extracted from 200 µl serum/plasma or effusion using the MagNA Pure 96 DNA and Viral NA Small Volume Kit (Roche) in conjunction with a MagNA Pure 96 Instrument (Roche), according to manufacturer’s instructions. RT-nPCR was performed using specific primers for the S gene region as previously described. 24 RT-nPCR was done as a touchdown PCR using RealTime ready RNA Virus Master Kit (Roche) and FastStart Essential DNA Probes Master Kit (Roche). All enzymes and buffers were used according to the manufacturer’s instructions. Touchdown cycling conditions were 15 mins at 50°C and 10 mins at 95°C; followed by nine cycles of: 20 s at 95°C, 60 s at 62.5–54.5°C for the first round of RT-nPCR and 67.5–59.5°C for the second round (step-downs every nine cycles of 1°C), and 45 s at 72°C; followed by 30 cycles of 20 s at 95°C, 60 s at 54.5°C for the first round and 59.5°C for the second round, and 45 s at 72°C; followed by a 7 min extension at 72°C. All samples were examined for inhibition of the RT-nPCR. Inhibition was detected only in one effusion sample of a cat with cholangiohepatitis.
DNA sequencing to detect the specific mutations
PCR products were purified prior to sequencing using the Min Elute PCR Purification Kit (Qiagen). Sequencing was performed by cycle sequencing using DyeDeoxy Terminator Sequencing Kit (Applied Biosystems) in an automated sequencer ABI 3130 Genetic Analyzer (Applied Biosystems).
Statistical evaluation
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and overall accuracy (sum of true positive and true negative test results divided by the total number of test results) were calculated using a four-field chart. To quantify uncertainty, 95% confidence intervals (CI) were calculated. Statistical analysis was performed using MS Excel (Microsoft) and Prism Version 5.04 (GraphPad Software).
Results
The final study population consisted of 127 cats. Of these, 64 had FIP and 63 were included in the control group.
RT-nPCR of either serum/plasma and/or effusion detected FCoV in 38 cats; all of them had FIP. A mutation was found in 33/38 of the PCR-positive cats. None of the 63 control cats tested positive by RT-nPCR (Figure 1). In two samples of the 38 RT-nPCR-positive cats, the sequence of the PCR product could not be determined; these samples were excluded from calculation of sensitivity, specificity, PPV, NPV and overall accuracy.
Of the 53 serum/plasma samples investigated, three tested positive by RT-nPCR; 2/3 had one of the two mutations in the S gene. For the third PCR-positive serum/plasma sample, no sequence could be determined. Of the 101 effusion samples, 36 tested positive by RT-nPCR; mutations were found in 32/36 of these PCR-positive samples (Tables 1–4). Sensitivity, specificity, PPV, NPV and overall accuracy are shown in Tables 5–7.
Results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach in serum/plasma samples (n = 53)
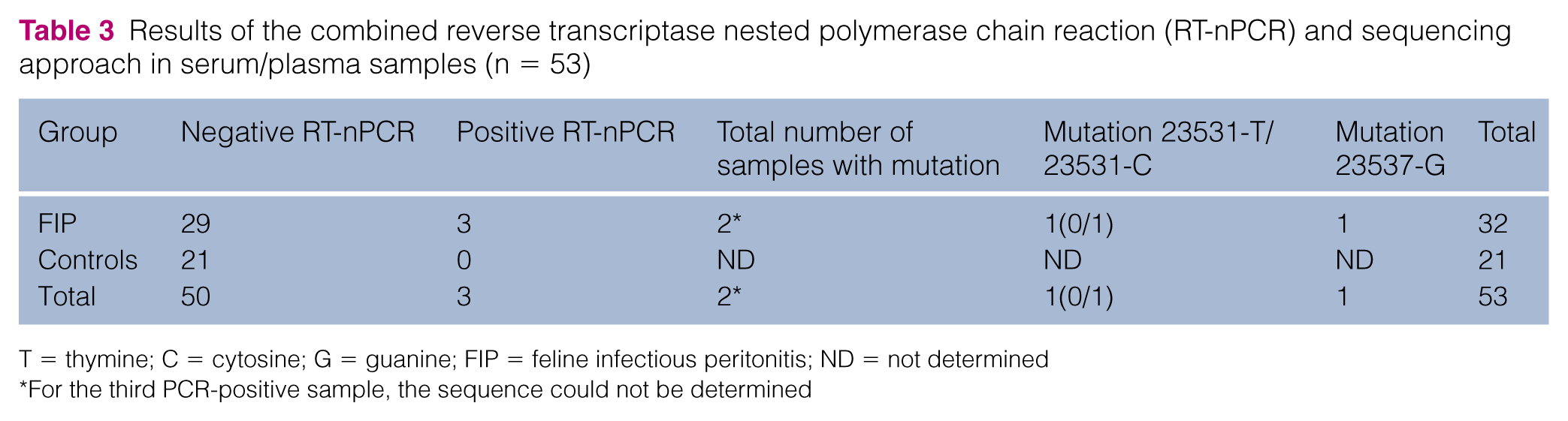
T = thymine; C = cytosine; G = guanine; FIP = feline infectious peritonitis; ND = not determined
For the third PCR-positive sample, the sequence could not be determined
Results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach in effusion samples (n = 101)
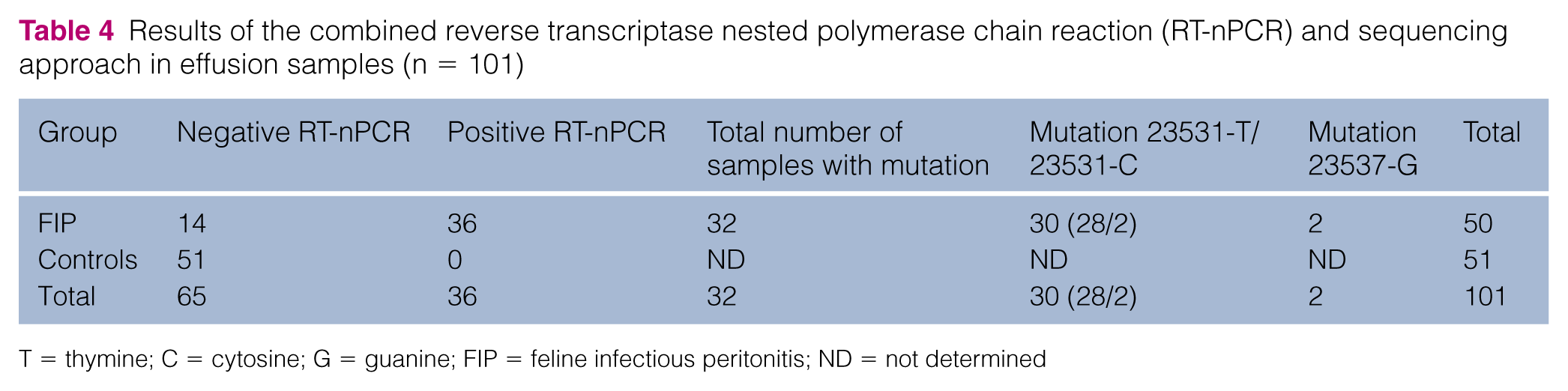
T = thymine; C = cytosine; G = guanine; FIP = feline infectious peritonitis; ND = not determined
Results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach in 52 serum/plasma samples (one serum sample was excluded because sequencing was not possible)
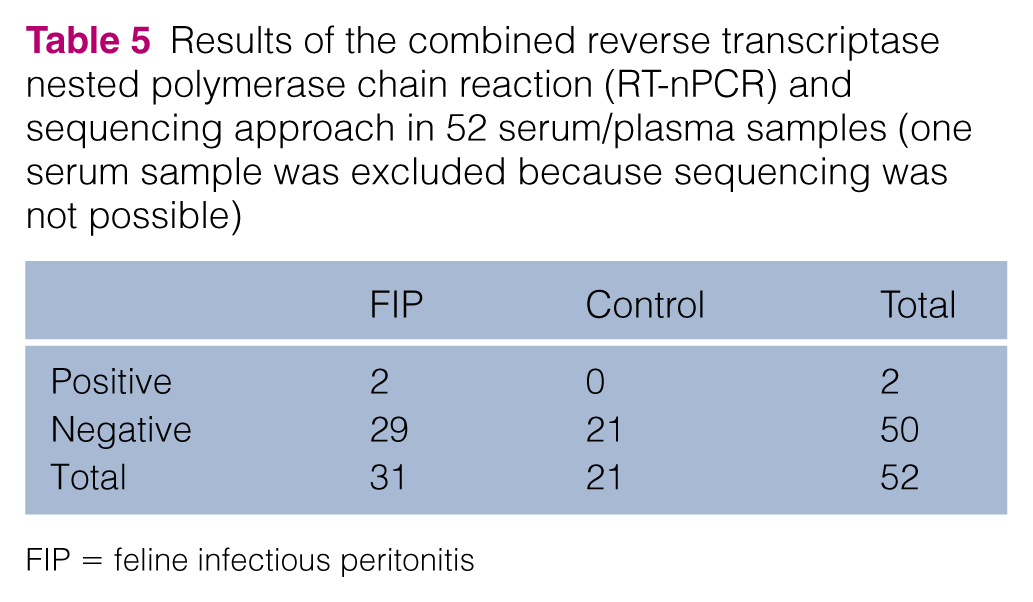
FIP = feline infectious peritonitis
Results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach in 100 effusion samples (one sample was excluded because sequencing was not possible)

FIP = feline infectious peritonitis
Results of the combined reverse transcriptase nested polymerase chain reaction (RT-nPCR) and sequencing approach in serum/plasma and effusion samples, and prevalence of feline infectious peritonitis (FIP) in 152 samples of 125 cats (one serum and one effusion sample were excluded because sequencing was not possible). Sensitivity refers to the RT-nPCR plus sequencing; specificity only refers to the RT-nPCR. Specificity of the sequencing step could not be determined because no cats of the control group were positive in the RT-nPCR

Data are % (95% confidence interval)
Prevalence of FIP in cats for which serum/plasma was available (number of cats with FIP divided by the number of all cats for which serum/plasma was available)
Prevalence of FIP in cats for which effusion was available (number of cats with FIP divided by the number of all cats for which effusion was available)
Two of the 25 cats that had to be excluded retrospectively tested positive by RT-nPCR. In one cat with suspected bacterial pleuritis (cytology of pleural effusion was suggestive of bacterial pleuritis, but bacterial culture was negative), FCoV-RNA was found in effusion by RT-nPCR, but sequencing did not detect a mutation. In another cat with suspected renal carcinoma (cytology of renal aspirate was suggestive of renal carcinoma but full-body necropsy and histopathology were not available and therefore the cat was excluded), RT-nPCR was positive in plasma and sequencing detected a mutation at position 23531.
Both serum/plasma and effusion samples were examined in 27 cats. In 12 of them, RT-nPCR plus sequencing was positive in effusion but negative in serum/plasma. In one cat, RT-nPCR plus sequencing was negative in effusion, while RT-nPCR was weakly positive in serum, but the sequence could not be determined. For another cat, serum, as well as effusion, gave a positive result by RT-nPCR plus sequencing.
Of the 33 cats with positive sequencing, in 30 an adenine (A)→thymine (T) or A→cytosine (C) transition at position 23531 was detected. In three cats, a T→guanine (G) transition at position 23537 was identified. Two cats exhibited two different nucleotides at the critical sites. In one of these cats, sequencing revealed both a T (mutated) and an A (non-mutated) at position 23531 in effusion. In the other cat, mutation 23531-T was found in effusion, while 23531-C was detected in serum.
Discussion
The aim of this study was to determine the diagnostic value of a combined RT-nPCR and sequencing approach in the diagnosis of FIP. FCoVs are separated into two different serotypes depending on growth characteristics in cell culture and on their relationship to canine coronavirus.45-47 Serotypes were not differentiated in the present study, as this is not of clinical relevance, because both serotypes can cause FIP. Therefore, it is possible that cats with FIP caused by type II FCoV were not detected in the present study.
This is the first study evaluating this approach in serum/plasma and effusion of cats that were presented with clinical signs typical of FIP. Thus, the strength of this study is that it mimics the real-life situation in which a clinician would submit a diagnostic sample to diagnose FIP. Diagnostic specificity of the RT-nPCR was very high in both serum/plasma and effusion; however, the specificity of the combined approach including the sequencing step could not be determined owing to the lack of control cats that were positive for FCoV in the RT-nPCR. Diagnostic sensitivity was 65.3% in effusion and only 6.5% in serum/plasma.
In a recent study, tissue and faecal samples of cats with and without FIP were examined with a quantitative RT-PCR and pyrosequencing. 27 A total of 112 tissue and faecal samples of 27 cats with immunohistochemically confirmed FIP and 16 control cats were directly compared. The authors found that nucleotide changes at position 23531 of the S gene resulting in amino acid differences at position 1058 of the predicted spike protein did not correlate with FIP disease phenotype. Both leucine (resulting from a T or C at position 23531) and methionine (resulting from an A at position 23531) codons were found in cats with and without FIP. A leucine codon was found not only in the majority (91%) of tissue samples of cats with FIP, but also in the majority (89%) of tissue samples of cats with other diseases. Additionally, a significant number (9%) of tissue samples from cats with FIP contained a methionine codon at position 1058. The authors therefore suggest that the M1058L substitution is a marker of systemic spread of FCoV rather than of FIP phenotype. However, in 2012 Chang et al found a M1058L point mutation only in cats with FIP. 24 A second substitution (S1060A, resulting from the nucleotide change at position 23537) was described by Chang et al to detect a further 4% of FIP cases. 24
Specificity in the present study was 100%, indicating that the combined RT-nPCR and sequencing approach is a valuable tool to confirm FIP. Interestingly, also the RT-nPCR by itself, even without sequencing, had the same high specificity. Nevertheless, as none of the control cats tested positive by RT-nPCR, a real control group for the sequencing was missing in the present study. Therefore, diagnostic specificity actually could only be determined for the RT-nPCR alone, and not for the combined approach. It is surprising that none of the finally included control cats was FCoV-viraemic and this raises the question of whether sequencing was necessary at all. Several studies investigated the use of RT-PCR assays as diagnostic tools and revealed rather low specificities.33–36,48,49 However, some of these studies used healthy cats originating from shelters or catteries as control group. In contrast in the present study, cats in the control group showed signs consistent with FIP, thus reflecting the population of cats presented to a veterinary practice in which a clinician would regard FIP as a differential diagnosis. The risk of FCoV infection increases in multi-cat environments.50–52 Unfortunately, the investigated control cat population without FIP in the present study did not include any FCoV-viraemic cats. Owing to this limitation the combined RT-nPCR and sequencing approach could not be evaluated in FCoV-viraemic cats without FIP that might be presented to a veterinary practice. Therefore, and therefore it could not be proven that FCoV with S gene mutations occur only in cats with FIP. If these mutations really are a marker for systemic spread of the virus rather than for FIP phenotype, 27 then it is possible that the test specificity would have been lower with a different study population.
Twenty-five cats were retrospectively excluded from the study because a definitive diagnosis could not be established when following very strict criteria. One of these cats was suspected of having bacterial pleuritis and effusion tested positive in RT-nPCR, but no mutation was detected. It is likely that the cat was viraemic with an apathogenic FECV that extravasated from blood into the body cavity. The existence of viraemia in FCoV-infected cats without FIP has previously been described,35,36,53 and inflammation of serosal surfaces might have led to leakage of blood components, including FCoV. Another cat was suspected of having renal carcinoma. The plasma of this cat was positive by RT-nPCR, and sequencing revealed a mutation at position 23531. It is possible that the cat was infected with an apathogenic FCoV and exhibited a mutation due to systemic spread of that virus rather than due to FIP. 27 Nevertheless, it cannot be excluded that the cat suffered from FIP instead of, or additionally to, the carcinoma.
The sensitivity of the combined RT-nPCR and sequencing approach in the present study was low. Sequencing of the PCR product was negative or not possible in only five of the 38 PCR-positive cats, which most likely was a result of a low virus load in the samples. Therefore, the RT-nPCR was mainly responsible for the low sensitivity and not the sequencing, even though the RT-nPCR was performed as touchdown PCR, which is known to have a higher sensitivity than the conventional PCR. 54 If the sensitivity of the PCR technique used had been too low, then positive PCR results could have been missed, also in cats without FIP. One possible explanation for the low sensitivity is likely a low virus load in the samples. The very low sensitivity of the approach in serum/plasma samples is in contrast to previous studies, detecting higher sensitivities of approximately 60–81% when investigating blood components.35,36,49 Monocytes/macrophages are the target cells for viral replication.14,40,55,56 Although serum and plasma have been commonly used, it is therefore possible that the sensitivity might have been higher in whole blood. Nevertheless, even whole blood has been recently identified as a poor sample type.57,58 In the present study, sensitivity was much better in effusion than serum/plasma. This indicates that cats with FIP exhibit much higher virus loads in effusion than in blood, 58 although in a study testing RT-PCR in ascites from cats clinically suspected of having FIP, virus was detected in only 377/854 cats (44.1%). 59 In these cats, however, FIP was not definitively confirmed. In the present study, which included only cats with FIP confirmed by gold standard methods, 36/50 cats with FIP (72%) tested positive by RT-nPCR.
The overall accuracy was calculated as the sum of true positive and true negative test results divided by the total number of test results, thereby being a marker for the overall diagnostic performance of the combined RT-nPCR and sequencing approach. Especially when using serum/plasma, the usefulness of the test is limited, as the overall accuracy was only 44.2%. Owing to the better diagnostic sensitivity, overall accuracy of the approach was much higher in effusion samples, reaching 83.0%.
As all samples collected ante-mortem were only obtained if needed for diagnostic and/or therapeutic purposes, the prevalence of FIP among the groups varied. Of the cats from which serum/plasma was available, 59.6% suffered from FIP, whereas 49.0% of the cats from which effusion was available had FIP. In a previous study, the prevalence of FIP was higher in cats with effusion (51%) compared with cats without effusion (28%). 34
One of the cats with FIP had two different mutations in serum and in effusion (23531-T in effusion, 23531-C in serum). Another cat with FIP showed signals of two different nucleotides at position 23531 upon sequencing of the PCR products in effusion. In this cat, both a T (mutated) and an A (non-mutated) were detected. It is possible that these cats were co-infected with two distinct FCoV variants. Previous studies have reported the existence of different virus strains within the same cat at the same time.19,27,60 As FIPVs likely arise by individual mutation from FECV,11,12 it is possible that the two variants evolved as independent mutations from one single parental virus.
In three cats with FIP, sequencing did not detect the mutations, although RT-nPCR was positive. It is possible that other critical mutations also lead to the development of FIP. A recent study compared FECV and FIPV sequences with regard to variations in a furin cleavage site in the region between receptor-binding (S1) and fusion (S2) domains of the spike gene and indeed found functional S1/S2 cleavage site mutations that were strongly correlated with FIP. 26
One limitation of this study was that in several cats only one sample type (serum/plasma or effusion) was available. Serum/plasma samples could not be obtained in already dead cats submitted directly for necropsy; on the other hand, some of the cats did not have effusions. Another limitation was that blood was only available either as plasma or serum, and whole blood might have given better sensitivities. In some of the cats of the FIP group, the diagnosis was established by a positive immunofluorescence staining of FCoV antigen in macrophages of effusions. A recently published study detected a specificity of only 71.4% for a direct immunofluorescence test. 61 In view of these results, it might seem possible that inclusion of cats with false-positive immunofluorescence test results into the FIP group has occurred, which might have decreased sensitivity of the combined RT-nPCR and sequencing approach.
Conclusions
This study evaluated the use of a combined RT-nPCR and sequencing approach in the diagnosis of FIP. Specificity and PPV of the RT-nPCR were 100% in serum/plasma and effusion specimens. Diagnostic specificity of the combined approach including RT-nPCR and sequencing could not be determined because no cats of the control group were positive in the RT-nPCR. Nevertheless, this result should be interpreted cautiously, as one cat with suspected renal carcinoma, that was retrospectively excluded from the study population, likely showed a false-positive test result. Sensitivity of the approach was rather low, with effusion yielding a much better result than serum/plasma. Therefore, a negative test result can never rule out FIP. The lack of sensitivity when using serum/plasma is disappointing, as this approach was considered especially important to test cats without effusions. Nevertheless, in the case of FIP, which is a fatal disease, specificity is the most important diagnostic parameter. A diagnostic specificity of near to 100% would prevent euthanasia of cats that were misdiagnosed with FIP due to false-positive test results. However, as none of the control cats were tested positive for FCoV in the RT-nPCR in this study, further studies are requested to evaluate the usefulness of the sequencing step in a control group with cats that test positive by RT-nPCR for the non-mutated virus.
Footnotes
Acknowledgements
We would like to thank Prof Dr Herman F Egberink, Department of Infectious Diseases and Immunology, Utrecht University, for fruitful discussions.
Conflict of interest
Dr Elisabeth Mueller is the Managing Director of Laboklin GmbH & Co KG. Dr Karola Weider is employed at Laboklin GmbH & Co KG. This laboratory offered the combined RT-nPCR and sequencing approach on a commercial basis and performed the testing in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.