
Abstract
Objectives
The objective of this study was to report the use of computed tomography (CT) in conjunction with clinical signs to assess the severity of pectus excavatum (PE) in kittens and to guide surgical decision-making; also to report medium-term outcome in a prospective cohort of kittens undergoing surgical correction.
Methods
This was a prospective study of 10–15-week-old kittens (n = 10) diagnosed with moderate/severe PE.
Results
CT provides additional information that is useful for selecting patients for surgical correction and for planning the surgery. Traditional radiographic indices (vertebral, frontosagittal) provide reasonable approximations of the CT-determined dimensions but these seem to correlate poorly with the severity of clinical signs. Kittens commonly have lateralised deformities, which are associated with less severe clinical signs, while those with midline deformities are associated with more severe clinical signs. Six of seven kittens with severe PE that had a ventral splint applied for 4 weeks had excellent medium-term outcomes.
Conclusions and relevance
Restriction of diastolic filling by midline sternal deviation may be an important cause of exercise intolerance in cats with PE. CT can be used to assess affected kittens and to plan surgery when indicated.
Introduction
Pectus excavatum (PE) is an uncommon, congenital thoracic wall deformity that has been previously documented in a variety of species, including humans, dogs and cats.1–4 PE is characterised by a palpable dorsal deviation of the caudal sternebrae resulting in a loss of thoracic volume and potential respiratory compromise.
In humans, PE is the most commonly observed thoracic wall abnormality occurring in between 1 in 400 and 1 in 1000 live births, and is commonly associated with connective tissue disorders such as Marfan and Ehlers–Danlos syndromes.5,6 Although familial tendencies have been demonstrated, it may well be a phenotypic response to a variety of underlying conditions, and its aetiology is incompletely understood. 6 The incidence of PE in kittens is unknown, although the defect seems to be more commonly seen in Bengal cats than domestic shorthair (DSH) cats, which is suggestive of there being a familial component to its expression. 7 The presence of PE is also positively correlated with flat-chested kitten syndrome in Burmese cats. 8
In cats, the severity of the deformity is traditionally graded using the vertebral (VI) and frontosagittal (FSI) indices as measured from orthogonal view thoracic radiographs (Table 1). 1 In humans, however, computed tomography (CT) is commonly employed to assess both the severity of the deformity and to assist with preoperative surgical planning.9,10
Vertebral (VI) and frontosagittal (FSI) indices for assessment of pectus excavatum (PE)

FSI = ratio of the thoracic width at T10 as measured on a dorsoventral radiograph and the distance from the centre of the ventral surface of T10 or vertebra overlying the deformity and the nearest point on the sternum; VI = ratio of the distance from the centre of the dorsal surface of the vertebral body overlying the deformity to the near point of the sternum and the dorsoventral diameter of the centrum of the same vertebra. Mean values for normal range are given in parentheses
We had noted an apparent discrepancy between the severity of clinical signs and radiographically determined vertebral and frontosagittal indices. This study describes the use of CT in assessing severity of PE in cats with the hypotheses that standard radiography accurately approximates CT-determined indices but that CT will provide additional information to explain the discrepancy between the radiographic and clinical severity of PE. We also provide short- and medium-term follow-up details for a cohort of 10 kittens that underwent CT with or without surgical correction.
Materials and methods
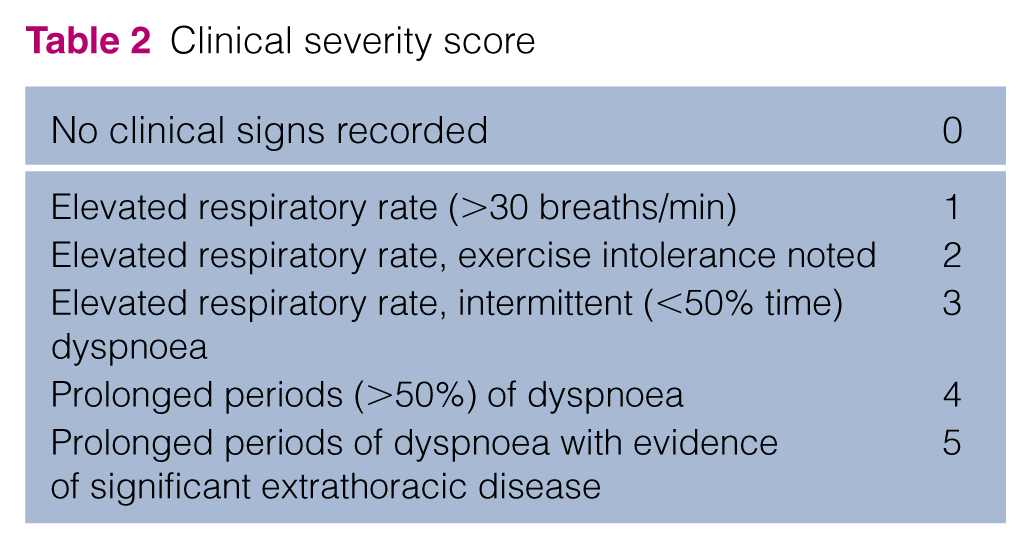
Kittens seen by the primary author (TMC) in the period 2012–2014 that were between 10 and 15 weeks of age diagnosed with moderate or severe PE (using published VI/FSI ranges) were eligible for inclusion in this study. Full patient data (age, breed, weight, history, results of clinical examination) were recorded and cases were allocated a clinical severity score (CSS) (Table 2). Kittens that had not had thoracic radiographs taken by the referring veterinarian were radiographed by the primary author (TMC) during the initial patient assessments. All radiographs were reviewed and the VI/FSI calculated by the primary author (TMC).
Clinical severity score
After a full clinical examination, kittens were premedicated with a standard protocol of 0.01 mg/kg acepromazine (ACP; Novartis) and 0.02 mg/kg buprenorphine (Vetergesic; Alstoe) and preoxygenated in an oxygen cage before induction with propofol (PropoFlo; Abbott Animal Health). Anaesthesia was maintained with isoflurane (IsoFlo; Abbott Animal Health) and supportive intravenous fluid therapy (Hartmann’s solution) was administered at 10 ml/kg/h. CT images were acquired using a two-slice GE Lightspeed scanner and standard helical thoracic protocol with 2.5 mm slice thickness with 1.25 mm slice interval with the kittens placed in dorsal recumbency. Postcontrast series were acquired using 2 ml/kg ioversol 64% (Optiray 300; Covidien) given as an intravenous bolus immediately prior to scanning. The kittens’ lungs were not hyperinflated prior to scanning and no attempt was made to induce a respiratory pause.
All CT scans were assessed at a later date by a board-certified diagnostic imager who was blinded to the clinical history/previous radiographs of each kitten. Images were evaluated using dedicated DICOM viewer software version 5.8.5–64 bit (Osirix; Geneva) on a computer workstation (Apple Mac Pro; Apple) with a calibrated 30 inch liquid crystal display flat screen monitor (Apple Cinemax Display; Apple). During the course of image evaluation, multi-planar reconstructions and variable windowing were used according to the preference of the diagnostic imager.
All CT studies were assessed for diagnostic quality and for concurrent musculoskeletal abnormalities. CT-determined VIs and FSIs were recorded for each kitten and compared with the radiographically determined VI/FSI using either recent (within 48 h of CT) radiographs or CT ‘scout’ images (planning radiographs) if judged to be of sufficient quality. Anticipated low case numbers precluded meaningful statistical analysis so scatter plots were used to illustrate any relationships between the measured radiographic and CT VI and FSI values. Correlation coefficients were calculated with an r value >0.5 taken as positively correlated and <0.5 as a negative correlation. Bias was assessed using Bland–Altman plots.
Additional CT analysis included measurement of lung volume and assessment of the nature of the sternal deformity. Lung volume was calculated by drawing an region of interest (ROI) around the surface of each lung and then using the ROI volume calculator tool of the imaging software. Results (cm3/kg) were compared with a control population of adult cats that had undergone thoracic CT for non-respiratory disease. The nature of the dorsal deviation of the caudal sternebrae (midline or lateralised) was also recorded, as was the location/number of the deviated sternebrae and their proximity to the visible overlying major cardiovascular structures. The presence/absence of lateralisation of the defect was compared with the CSS.
Two kittens had an additional dynamic CT performed to assess the degree of movement of the sternum during the respiratory cycle. A cine protocol was used to take sequential transverse sections at the estimated point of maximum sternal deformity with images acquired every 0.5 s for 20 s. The distance between the sternum and vertebral body was measured at the points of greatest inspiration and expiration for the two dynamic CT studies and the percentage change calculated.
Surgical methods
Cases that had a severe (<6) VI and clinical signs attributed to PE (CSS 1–5) were considered to be surgical candidates. The surgical technique was based on that published elsewhere.11,12 In brief, the kittens were placed in dorsal recumbency and a ventral sternal cast (Dynacast Prelude; BSN Medical) was made conforming to the anticipated postoperative position of the sternum, which was facilitated by applying moderate laterolateral compression to the thorax during the casting process. Circumsternal 3.5 M polypropylene sutures (Prolene; Ethicon) were then placed as single interrupted sutures starting cranially and progressing caudally. The ends of the sutures were left long and passed through the cast before tying under tension while simultaneously applying moderate laterolateral thoracic compression. Cases that had no detectable safe corridor for suture passage underwent a minimal dissection to the caudal sternebrae, which were then directly retracted ventrally allowing the circumsternal sutures to be passed. This wound was closed using subcutaneous 1.5 M or 2 M glycomer 631 (Biosyn; Covidien) before routine cast placement. All casts were covered by chest bandages and postoperative thoracic radiographs were taken.
Kittens that underwent surgery were discharged the next day on 5 day courses of 0.05 mg/kg meloxicam q24h (Metacam; Boehringer Ingelheim) and 20 mg/kg potentiated amoxicillin q12h (Synulox Palatable Drops; Zoetis). The casts were maintained for 4 weeks at which point they were removed under anaesthesia using an identical anaesthetic protocol as above. Thoracic radiographs were taken to assess the degree of PE correction, and postoperative VIs were calculated by the primary author (TMC).
Medium-term follow-up was obtained by email/telephone contact with the owners/referring veterinarians and the kittens were allocated new CSSs. Pre- and postoperative CSSs were then compared.
Results
Ten kittens met the inclusion criteria during the study period. Breed distribution was as follows: Bengal (n = 5), DSH (n = 4) and Maine Coon (n = 1). There were four female and six male kittens. Median weight at time of surgery was 1.17 kg (range 0.65–2.00 kg). Clinical signs reported included palpable abnormality (n = 10), tachypnoea (n = 7), exercise intolerance (n = 4), at least one previous episode of antimicrobial responsive dyspnoea (n = 3), stunting/poor growth (n = 3), dehydration (n = 3), chronic dyspnoea (n = 2), constipation (n = 2) and polyuria/polydipsia (n = 1). Allocated CSSs were as follows: 1 (n = 4), 2 (n = 3), 4 (n = 2) and 5 (n = 1).
All CT scans were deemed to be of diagnostic quality. Two kittens (G, H; see Table 3) did not have radiographs or CT ‘scout’ images of sufficient quality for VI and FSI to be accurately measured and so these cases were omitted from the analysis. Radiographic and CT measurements/indices are given in Tables 3 and 4. CT and radiographically determined indices (VI, FSI) were compared, and the results are shown in Figures 1 and 2. CT consistently gave a lower value for the VI, with a mean difference of −0.53. The FSI calculated from CT images tended to be higher than the value calculated from radiographic measurements.
Clinical data and radiographically determined indices at presentation
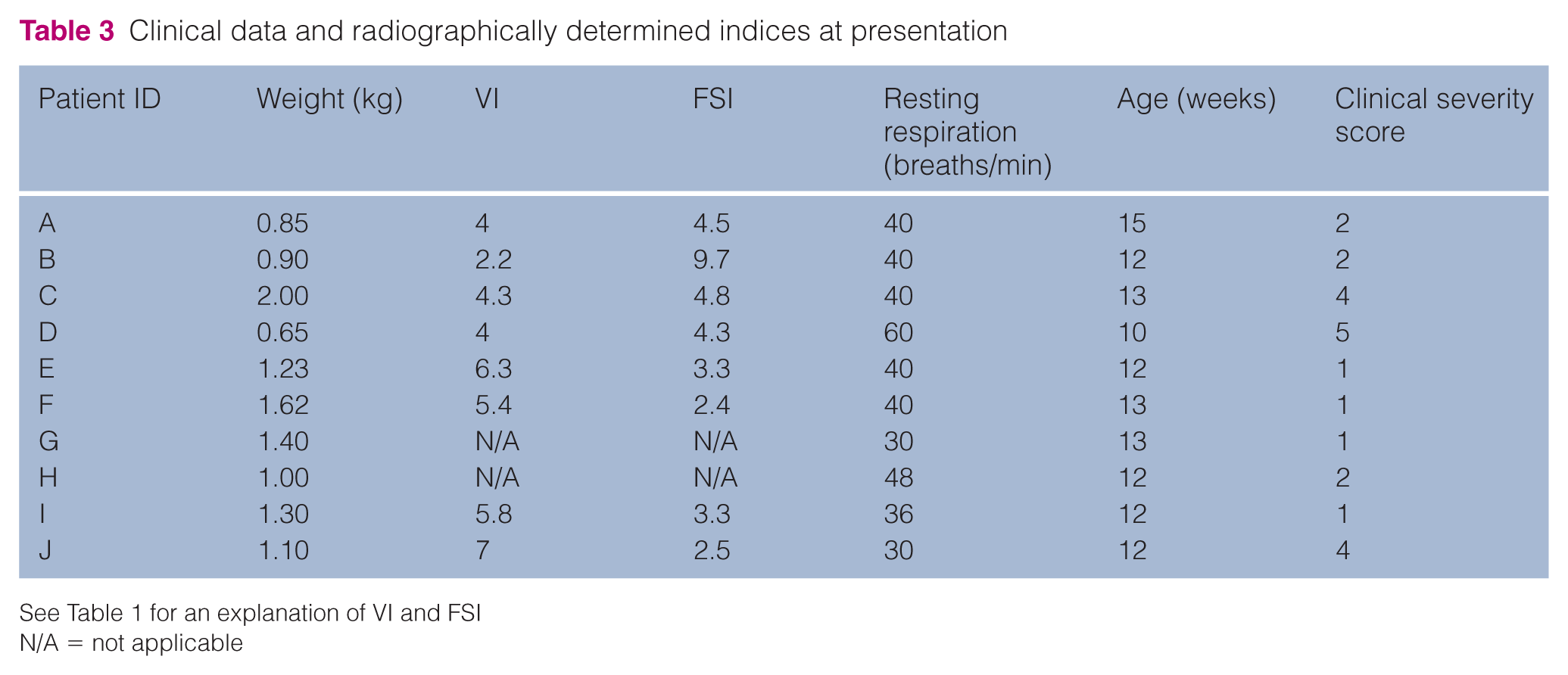
See Table 1 for an explanation of VI and FSI
N/A = not applicable
Calculated indices from computed tomography measurements
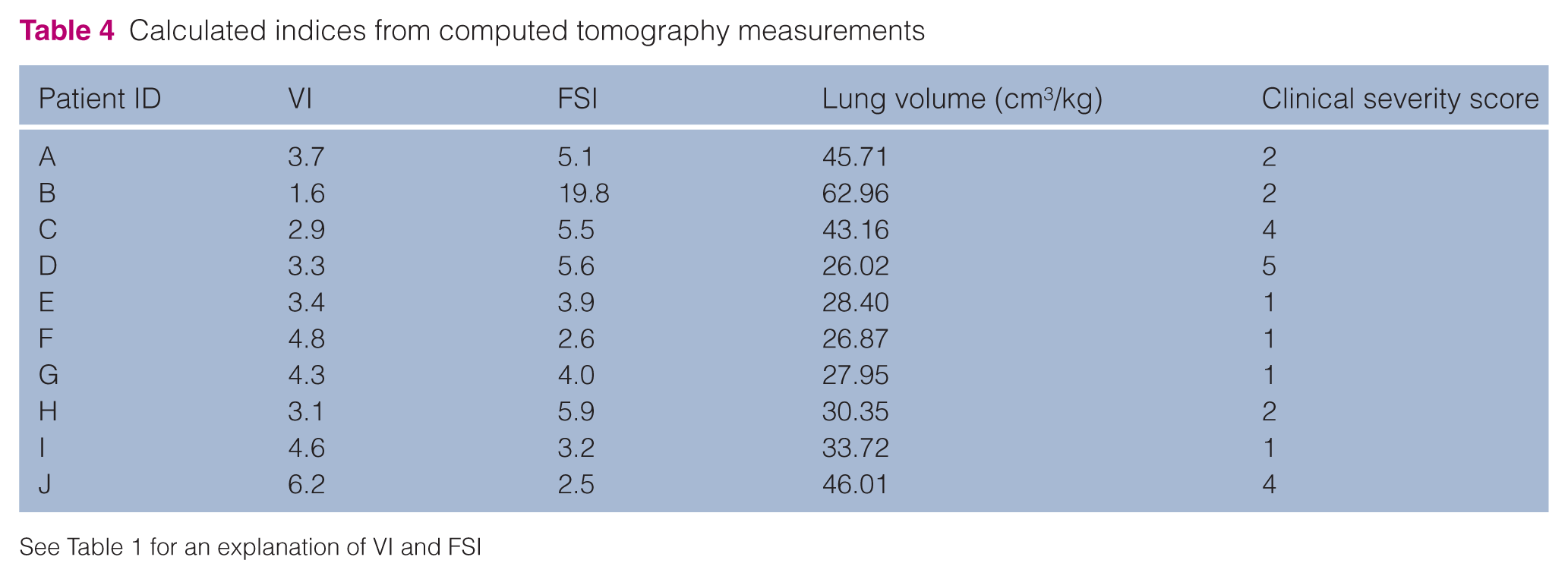
See Table 1 for an explanation of VI and FSI

Bland–Altman plot of the data obtained from eight paired measurements of the vertebral index (VI) using computed tomography (CT) or radiographic imaging. r = 0.20 (P = 0.64); slope = −0.058 (P = 0.64); intercept = −0.28 (P = 0.62)

Bland–Altman plot of the data obtained from eight paired measurements of the frontosagittal index (FSI) using computed tomography (CT) or radiographic imaging. r = 0.983 (P <0.01); slope = −0.422 (P = <0.01); intercept = −1.35 (P = <0.01)
The distance between the dorsal-most point of the deviated sternum and the overlying vertebra (‘c’) was determined at maximum inspiration and expiration for each of three respiratory cycles for two kittens for which a cine scan was performed. In the first kitten, ‘c’ changed by an average of 3.16% and by 0.68% in the second.
Lung volume/kg body weight did not appear to be significantly different from that of the control population (mean PE 37.1 cm3/kg, mean control 45.3 cm3/kg), although low case numbers precluded statistical analysis. CT review showed that the dorsal sternal deviation was lateralised in 5/10 kittens and this was dextral in 4/5 cases. The kitten with sinistral deviation was diagnosed with complete situs inversus. No other musculoskeletal deformities were detected. Kittens that had a lateralised sternal deformity tended to have a lower CSS than those that did not (1, 1, 1, 1 and 2 vs 2, 2, 4, 4 and5).
The sternebrae closest to the overlying major cardiovascular structures were 5–7 (four kittens), 5–8 (two kittens), 6–8 (two kittens), 6–7 (two kittens), 4–6 (one kitten) (see Figure 3). The dorsal aspect of the sternal deformity was judged to be in contact with a major cardiovascular structure in 9/10 cases. The tenth case was judged to have a safe corridor for needle passage of 2 mm.

Sternebrae closest to overlying cardiovascular structures in each of the 10 kittens
Short-term/medium-term follow-up
Cases A, B, C, F, G, H and I underwent surgery. Case D was polyuric/polydipsic, anorexic and significantly dehydrated at the time of presentation and was euthanased at the owner’s request. A post-mortem CT examination was performed in this case with the owner’s consent. Cases E and J were judged to have PE of medium severity based on VI. Case E had a CSS of 1 and surgery was not recommended. Case J presented with a CSS of 4 and surgery was recommended but was declined by the owner.
There were no intraoperative complications in any of the cases that underwent surgery.
One week after surgery, case A developed furosemide-responsive dyspnoea that required hospitalisation and oxygen supplementation. Dyspnoea partially resolved but required continued medication. Case A developed cardiorespiratory arrest under anaesthesia for cast removal and did not respond to resuscitation attempts. VI was improved (higher) in all cases that underwent surgical correction (Table 5).
Follow-up data
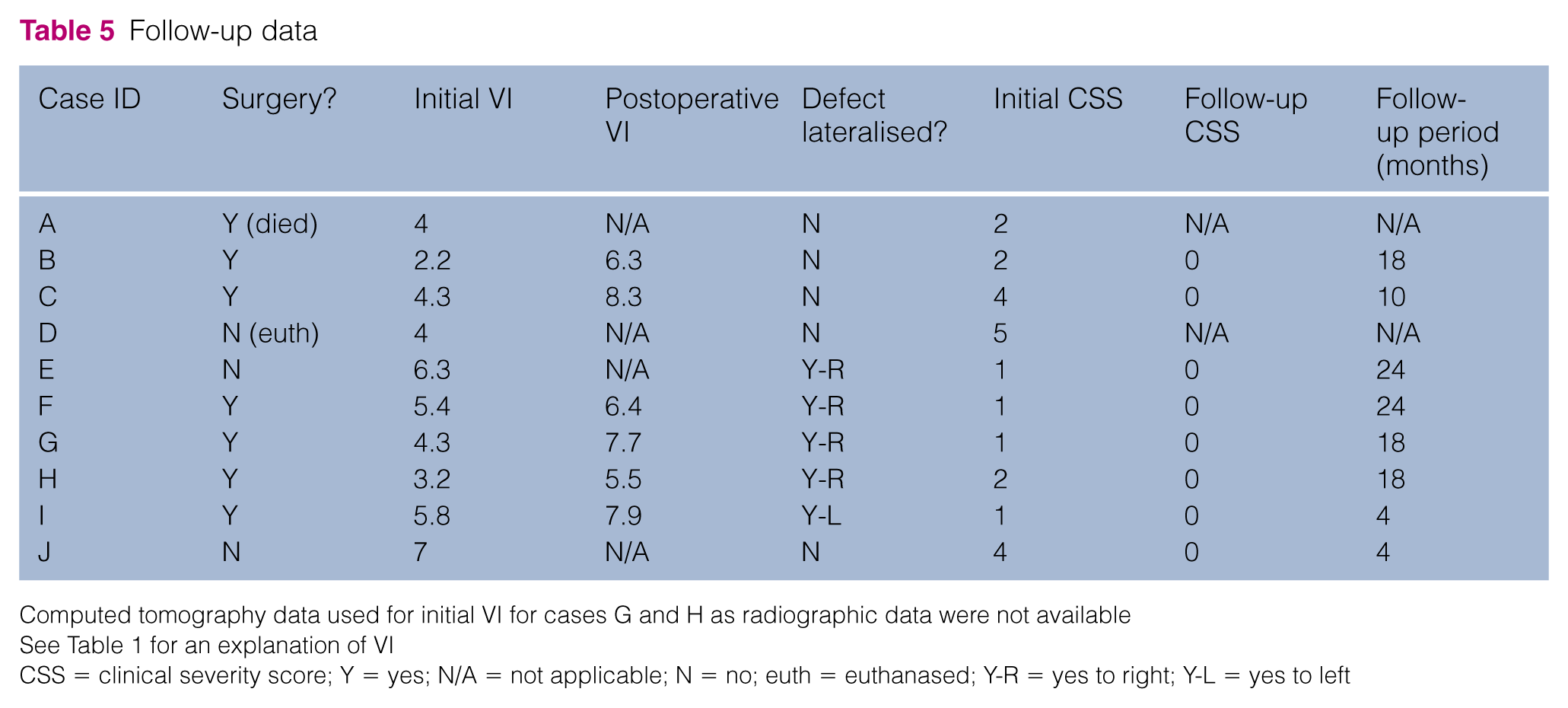
Computed tomography data used for initial VI for cases G and H as radiographic data were not available
See Table 1 for an explanation of VI
CSS = clinical severity score; Y = yes; N/A = not applicable; N = no; euth = euthanased; Y-R = yes to right; Y-L = yes to left
No moist dermatitis or pyoderma secondary to cast placement occurred in any of the cases. The owners did not report any clinical signs of PE in all surviving kittens.
Follow-up data and CSSs are listed in Table 5.
Discussion
Ten kittens were recruited into this study, five of which were Bengals. Although adequate population data are not available for statistical analysis, this tends to support Bengal kittens being at increased risk of PE, 7 although bias in the referred population is possible.
The clinical signs reported by the owners and/or breeders were variable. Although some inter-observer variation is probable, all clinical histories were taken by the same veterinary surgeon, and the severity of historical signs reported seemed to correlate with clinical signs at presentation. Tachypnoea was the most common clinical sign reported after ‘palpable deformity’, which is a diagnostic feature of PE. Tachypnoea was presumed to be due to decreased lung volume and impaired alveolar exchange, and forms part of a continuum of signs progressing to exercise intolerance and respiratory distress presumably with increased severity of deformity. This spectrum of signs formed the basis for the CSS that was used in this study. Surprisingly, however, the lung volume (as a proportion of body weight) of affected kittens was not significantly different from a control population of unaffected cats. Larger case numbers and, ideally, an age-matched control population would allow statistical analysis and verification of these preliminary findings. Results could be further confounded by a compensatory increased depth of respiration seen in affected kittens. More information could be obtained by lung plethysmography but this is not widely available for veterinary patients, particularly those with small tidal volumes.
Three of the 10 kittens had at least one previous episode of antimicrobial-responsive dyspnoea. In each case, dyspnoea responded rapidly to the administration of potentiated amoxicillin. The exact site and cause of the presumed infection is not known but this could be caused by ventilation impairment, failure to clear alveolar secretions or other functional abnormalities.
Although only assessed in 2/10 cases, the sternum did not move significantly during the respiratory cycle, with ‘c’ values varying by only 3.16% and 0.68%, respectively. This suggests that radiographically determined VIs should be relatively constant independent of the respiratory phase at which they were taken.
There was reasonable correlation between radiographically determined and CT-determined VIs and FSIs: CT consistently gave a lower value for the VI, with a mean difference of 0.53, and FSI calculated from CT images tended to be higher than the value calculated from radiographic measurements. The mean difference in FSI was 0.83 but there was a significant association between the variation and the value of the FSI. These findings suggest that separate reference intervals for normality and severity of VI and FSI are appropriate depending on the imaging modality used but that an appropriate reference interval for CT-calculated FSI can be inferred from the published radiographic FSI values.
No significant concurrent musculoskeletal deformities were identified in any of the affected kittens. In each case the sternum started to deform in the caudal half and the deformity was dorsal but also lateral in 5/10 cases, with 4/5 being deviated to the right hemithorax. The case with sinistral deviation of the xiphoid was the cat with situs inversus. The cause of this lateralisation away from the heart is uncertain, but possible explanations include displacement of the caudally deviated sternebrae by the heart and/or traction from the diaphragmatic crura during development.
Cardiac perforation is a recognised complication of placing a ventral corrective splint. 12 The deformed sternum was judged to be in contact with either the heart or the caudal vena cava in 9/10 cases, with case 10 having a safe corridor for suture placement of only 2 mm. Having demonstrated how close the dorsal sternebrae were to the heart in all our surgical cases, we modified our surgical technique accordingly. No intraoperative complications were encountered and no postoperative complications relating to this approach were seen.
VI and FSI are useful for initial screening of cases into an anatomic severity category – mild, moderate or severe – but they do not appear to be useful for determining whether cases with moderate-to-severe anatomical defects are likely to have severe clinical signs. This would imply that there may be other factors beyond simple musculoskeletal deformity that are contributing to the severity of the clinical signs observed. Cats with lateral deviation of the xiphoid seemed to be associated with a lower clinical score than those kittens with a midline deviation. It has been suggested that clinical signs of PE in humans may be partially due to a direct compressive or restrictive effects of the displaced sternebrae on the heart itself. 13 Athletic performance is compromised by the inability of the heart to increase diastolic volume to meet increased oxygen demands, and direct compression of the right side of the heart in humans is considered to be an indication for surgery.9,13 It is possible that clinical signs seemed to be more severe in cats with a midline pectus deformity due to a similar mechanism, whereas the kittens with a lateralised defect had more space available for the heart to increase diastolic volume as required. Cardiovascular compromise may therefore be a more significant driver of clinical signs associated with PE in kittens than altered pulmonary function. This could be why case J, which had a midline sternal deviation, had severe clinical signs despite a ‘moderate’ VI (7) and it may be that a different threshold (higher VI) should be used when deciding if kittens with midline defects should undergo surgery.
One case (A) developed significant postoperative furosemide-responsive dyspnoea and then died at the time of cast removal. The apparent initial response to diuretics is suggestive of pulmonary oedema, which could be caused either by pulmonary re-expansion, concurrent cardiovascular disease or pulmonary hypertension. 14 Although no significant concurrent cardiovascular disease was detected on the initial CT scan, this modality is not as sensitive as echocardiography when assessing cardiac function. The cause of death at the time of cast removal remains unknown as no post-mortem analysis was permitted.
All cases that survived showed full resolution of clinical signs with no exercise intolerance or episodes of dyspnoea reported at the time of follow-up. While we used a combination of VI and CSS to determine which cases would benefit from surgery, there was no control population for which treatment was intentionally withheld in order to demonstrate a difference in postoperative outcome as this would have been unethical. We suspect that many cases of severe PE are euthanased owing to perceived poor prognosis and financial concerns about treatment costs. This, and the rarity of the condition, resulted in only low numbers of cases being recruited, despite internet-based advertising for case enrolment. We are therefore limited to making broad recommendations about patient selection and treatment efficiency. In our study, patients were selected for surgery based on VI and clinical signs. All cases had a sternal cast maintained for 4 weeks, and all cases that survived are currently asymptomatic at a mean follow-up time of 15 months. One of the risks of uncorrected PE is the development of pulmonary hypertension and right-side heart failure, which we have observed in multiple cats aged <12 months. It is possible that some of our cases could develop respiratory signs at a later stage and we intend to publish longer-term follow-up (5 year) data when available.
Conclusions
Conventional radiography yields reasonable approximations of CT-determined VI and FSI. CT was useful in determining the presence/absence of safe corridors for circumsternal suture placement leading to a minor modification of the surgical approach employed for ventral cast placement. CT also allowed detection of cats with midline sternal deviation that may be at risk of developing more severe clinical signs due to diastolic restriction despite relatively mild skeletal deformity. Ten- to 15-week-old kittens with severe deformity as judged by VI and with compatible clinical signs can be treated by placement of a sternal splint for a 4 week period, which is associated with an excellent medium-term outcome.
Footnotes
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
This research received no grant from any funding agency in the public, commercial or not-for-profit sector.