
Abstract
Rationale
Recent recognition of the need to improve pain management in cats has led to the investigation of the pharmacokinetics and efficacy of opioid analgesic drugs in this species. The results of these studies may be difficult to interpret because the effect of these drugs varies with dose, route of administration and the method used to assess them. As equipotency of different opioids is not known, it is hard to compare their effects. Animals do not verbalise the pain they feel and, in cats, it may be more difficult to recognise signs of pain in comparison with other species such as dogs.
Aim
This article reviews the use of opioid analgesics in cats. It must be remembered that not all drugs are licensed for use in cats, and that marketing authorisations vary between different countries.
Introduction
In recent years research into pain assessment and management in cats has increased. This interest and focus may have been in response to reports that cats have been undertreated for pain in comparison with other species.1 –4 Advances in knowledge have led to internationally recognised veterinary bodies issuing guidelines on pain management in cats, including those very recently from the American Animal Hospital Association and the American Association of Feline Practitioners. 5 In 2014, the World Small Animal Veterinary Association also published guidelines on the recognition, assessment and treatment of pain. 6
Pain assessment in cats
Pain assessment and quantification in animals is challenging because pain is a subjective sensory and emotional experience and animals are unable to verbalise their suffering. The most reliable way to assess pain in cats is thought to be through a combination of behavioural observations and interaction with the animal. 7 Various scales have been created to try to quantify pain in cats. For example, the Colorado State University Veterinary Medical Center has designed a feline acute pain scale, 8 whereby psychological and behavioural components are evaluated in conjunction with the cat’s response to palpation of the site of surgery and its body tension. In many studies the visual analogue scale (VAS) is used: an assessor marks a point on a 100 mm line that best correlates with the cat’s pain intensity; VAS is based on visual observation and ‘0’ is considered no pain, while ‘100’ is considered the worst pain imaginable. The so-called dynamic interactive visual analogue scale (DIVAS) also includes interaction with the cat, such as palpation of the wound. Recently, a multidimensional composite scale for assessing postoperative pain in cats has been validated. 9 This tool combines evaluations of postoperative psychomotor changes, reaction to palpation of the wound area and vocal expression of pain, together with appetite and arterial blood pressure. It is important to remember that increased arterial blood pressure can be a sign of stress, fear and anxiety, and not necessarily pain. Another method with the potential to assess pain in cats is the evaluation of facial expressions. 10
Limitations of pain assessment using the aforementioned methods include the subjective nature of the evaluation and the difficulties in recognising behavioural clues that may be indicative of pain, particularly in a hospital environment. However, use of a pain scale has the advantages that it focuses the attention of members of staff on pain and also means that an individual cat’s response to analgesic administration can be assessed and monitored.
Nociceptive threshold testing has been used to assess the antinociceptive effects of analgesic drugs in a more objective way. In cats, mechanical, thermal and electrical threshold testing has been employed in experimental settings to evaluate the effects of opioids.11,12 For each of these techniques a baseline nociceptive threshold is measured, an analgesic is then administered and the thresholds are measured again at specific time points. An increase in the threshold is usually accepted as evidence of a drug’s anti-nociceptive effect. Nociceptive threshold testing does have a number of limitations, 13 including the lack of evaluation of the emotional components of pain. Despite these limitations it is a useful tool for identifying drugs and dosages for further evaluation in clinical cases. In a clinical setting, mechanical nociceptive testing has also been used, in conjunction with subjective assessments of pain, in cats undergoing surgery. 14
There are numerous publications investigating the effects of drugs on the minimum alveolar concentration (MAC) of inhalant anaesthetics in cats. However, this is not an effective way to evaluate the analgesic effects of opioids 15 since it only indicates the immobilising potency of the inhalation anaesthetic at the spinal cord level, while pain also involves supraspinal pathways. Several opioids, including morphine, buprenorphine, methadone, butorphanol, hydromorphone, fentanil, alfentanil, remifentanil and tramadol, have been proven to decrease, to different degrees, the MAC of inhalant anaesthetics, but the effects were not always clinically relevant and were not as profound as have been reported in other species, including dogs.16 –23 Thus, a significant reduction in volatile anaesthetic concentration after opioid administration should not be expected in the clinical setting.
When discussing opioids, opioid receptors and comparisons between different opioid drugs, some concepts should be made clear. Affinity refers to how avidly a drug binds to a receptor, efficacy indicates the magnitude of the effect produced by the drug–receptor interaction, and potency indicates the quantity of drug needed to produce a maximal effect. 24
Opioids and cats
Opioids play an important role in the clinical management of pain in cats. Ideally, analgesics should be administered before noxious stimulation (preventive analgesia) with the aim of preventing sensitisation of the central nervous system, which could lead to the development of hyperalgesia. A multimodal approach is also recommended; this involves the concurrent administration of different classes of analgesics, such as opioids, non-steroidal anti-inflammatory drugs (NSAIDs), local anaesthetics and α2-adrenoreceptor agonists, with the aim of decreasing the doses and thus the side effects of individual agents, while improving the control of pain in the animal. 6
In cases of acute pain, opioids are effective and versatile analgesics, with wide therapeutic margins and relatively minor side effects in cats. 6 Their effects can also be antagonised if required. Historically there was a reluctance to administer opioids to cats due to concerns over the potential excitatory effects reported by Wikler in 1944. 25 However, ‘morphine mania’ was elicited at doses 100-fold higher (15 mg/kg) than those used in the clinical setting. 26 Sufentanil and alfentanil administration in cats is associated with an increase in sympathetic outflow and central stimulatory effects,27,28 but a study investigating morphine administered to cats at clinical (0.3 mg/kg) and supraclinical (0.6–2.4 mg/kg) doses reported no excitement. 29 At clinically used doses the behavioural effects of opioids include euphoria, manifesting as purring, rubbing, rolling and kneading with the forepaws.30 –35
Opioids cause mydriasis in cats, 36 which outlasts their analgesic effects and may affect vision. In dogs, the incidence of vomiting and salivation following morphine, hydromorphone and oxymorphone administration was reduced by prior administration of acepromazine. 37 This has not been studied in cats but it is possible that a similar effect may be seen. Decreased intestinal motility is a potential adverse effect of opioids but the clinical relevance of this in healthy cats is questionable, and in a study where buprenorphine was administered with acetylpromazine the orocaecal transit time, assessed by the breath hydrogen method, was not affected. 38
Postanaesthetic hyperthermia, defined as a rectal temperature higher than 39.2°C, has been associated with opioid administration in cats. Moreover, it was shown in a prospective clinical study of 40 healthy adult cats that body temperature at extubation was inversely related to the degree of postanaesthetic hyperthermia; that is, the colder the cat was at the end of anaesthesia, the higher the temperature was reported to be during recovery. 39 In a prospective randomised crossover study, buprenorphine (0.02 mg/kg IM), butorphanol (0.2 mg/kg IM), morphine (0.5 mg/kg IM) and hydromorphone (0.05–0.2 mg/kg IM) caused mild/moderate and self-limiting increases in body temperature (<40.1°C). 40 Alfentanil infusion increased body temperature in isoflurane-anaesthetised cats, 20 but not in propofol-anaesthetised cats. 41 An increase in body temperature has been detected with transdermal fentanyl patches in cats undergoing onychectomy, with mean rectal temperatures ranging from 38.8–39.4°C in the postoperative period. 30 Morphine and pethidine may cause hyperthermia at doses much higher than those recommended.42,43 In the light of these findings, it is recommended that a cat’s body temperature is closely monitored during anaesthesia and in the perioperative period.
Other side effects of opioid therapy in people are opioid-induced hyperalgesia and tolerance, 44 but these have not been reported in cats to date. This may be due to the relatively short duration of opioid administration in animals compared with people (where they may be used for long periods, particularly in the palliative care setting), meaning that opportunities for detecting these phenomena are limited. Challenges associated with determining whether changes in response to opioids are due to hyperalgesia/tolerance or disease progression, or due to different metabolisation of drugs in cats compared with people, might also be a factor. 15
As in people, great variability in the response of individual cats to opioids has been observed;7,45,46 a phenomenon known as ‘pharmacogenomics’. 47 Hence it is important to tailor the analgesic protocol to fit the individual patient’s needs in order to maximise pain relief while minimising side effects. Although adverse events may occur, opioids are effective analgesic drugs to be used in cases of moderate/severe pain and the risk of severe side effects is low in comparison with other classes of analgesics, such as NSAIDs. 48
In this review of the use of opioids in cats, opioids licensed for use in cats are discussed before those that are not licensed. Licensing of drugs is country-specific and readers need to be aware of the prescribing laws pertaining to their own country.
Pethidine (meperidine)
Pethidine is a synthetic full µ receptor agonist 49 that has a marketing authorisation at a dose of 3.3 mg/kg by intramuscular (IM) injection in cats in some European countries, including the UK. It should not be administered intravenously (IV) because it causes histamine release. 50 Vomiting is a rare side effect. 43
Clinical and experimental studies have evaluated various doses of pethidine, ranging from 2–10 mg/kg, alone and in combination with other drugs (Table 1). The onset of analgesic effect is rapid (30 mins) and the duration of action is dose-dependent, ranging from 1–2 h.11,14,55 These characteristics mean that pethidine may be a good option in cats that require short-term pain relief and/or frequent re-evaluation of the neurological system. However, other opioids may be more suitable where a longer duration of analgesia is required, such as after surgery.
Studies evaluating pethidine in cats

‘+’ identifies where drugs were given in combination; where individual drugs were compared in different groups of animals, these are separated by commas
B = buprenorphine; CAR = carprofen; Clp = plasma clearance; DEXM = dexmedetomidine; DIVAS = dynamic interactive visual analogue scale; ENT = electrical nociceptive threshold; KETO = ketoprofen; MNT = mechanical nociceptive threshold; OHE = ovariohysterectomy; P = pethidine; PK = pharmacokinetics; T½ el = elimination half-life; TNT = thermal nociceptive threshold; VAS = visual analogue scale
Methadone
Methadone has recently received marketing authorisation for use in cats at a dose of 0.3–0.6 mg/kg in the United Kingdom, Italy and some other European countries. The results of various studies on methadone in cats are summarised in Table 2. Methadone is a synthetic µ opioid receptor agonist drug, consisting of a racemic mixture of D and L enantiomers. In addition to its interaction with the µ opioid receptor, the D isomer exerts an antagonistic action at the N-methyl-D-aspartate (NMDA) receptor. 60 Moreover, methadone plays a role in the descending pain pathways by inhibiting the reuptake of serotonin and noradrenaline, and by blocking the nicotinic cholinergic receptors.61,62 These receptor interactions could explain the good analgesic and possible anti-hyperalgesic effects that have been demonstrated using mechanical nociceptive testing in cats receiving methadone as part of pre-anaesthetic medication before ovariohysterectomy. 31
Studies evaluating methadone in cats

See footnote to Table 1
B = buprenorphine; BUT = butorphanol; HYDRO = hydromorphone; IVAS = interactive visual analogue scale; MAC = minimum alveolar concentration; MET = methadone; MNT = mechanical nociceptive threshold; MOR = morphine; NRT = numerical rating scale; OHE = ovariohysterectomy; OTM = oral transmucosal; OXY = oxymorphone; TNT = thermal nociceptive threshold; VAS = visual analogue scale
In the experimental setting, methadone administration (0.2–0.6 mg/kg) resulted in antinociception to thermal and mechanical stimuli.32,33 The duration of antinociception to the thermal stimulus was longer than that to the mechanical stimulus, and also depended on the dose and route of administration; the duration of antinociception to the mechanical stimulus after 0.2 mg/kg SC was only 45–60 mins, whereas it was up to 4 h after 0.3 mg/kg IV. This suggests that the IV route is preferable where a longer duration of action is required.
In clinical studies, methadone, at doses of 0.3–0.5 mg/kg IM or SC, provided a dose-dependent period of analgesia lasting from 1.5–6.5 h.31,56 –58
In some countries the levorotatory enantiomer is available; when levomethadone (0.3 mg/kg IM) was compared with racemic methadone (0.6 mg/kg IM) it produced satisfactory postoperative analgesia after ovariohysterectomy. 57 Mechanical nociceptive threshold testing has been used to compare oral transmucosal (OTM) (0.6 mg/kg) with IV (0.3 mg/kg) administration of methadone. 33 A similar duration of antinociception to a mechanical stimulus was reported, although a less profound response for up to 1 h after administration was evident, suggesting a slower onset of full effect after OTM administration. It is worth noting that the OTM dose was double that administered IV, but these data suggest that methadone is absorbed by this route and recently a mean bioavailability of 44.2% was reported after buccal administration of methadone in cats. 59
The OTM route does look promising for administering methadone to difficult-to-inject cats, but further studies are required to determine the efficacy in clinical cases. Assessing the depth of anaesthesia and titrating the amount of anaesthetic agent to obtain a suitable depth of anaesthesia is important in all anaesthetised animals. Methadone (0.3 mg/kg IV) has been reported to decrease the MAC of sevoflurane in cats by 7–25%, so the vaporiser setting may need to be reduced. 17 As already mentioned, MAC reduction cannot be considered as a surrogate for analgesia.
Buprenorphine
Buprenorphine is a highly lipophilic semi-synthetic partial µ agonist opioid, 63 with a marketing authorisation for use in cats in the USA and several European countries. A wide variation in the duration of analgesic and antinociceptive effects has been reported for buprenorphine (Table 3). This variation may be attributed to different doses, routes of administration and methods of assessment, and individual variation between cats.
Studies evaluating buprenorphine in cats

See footnote to Table 1
B = buprenorphine; BUT = butorphanol; CAR = carprofen; CI = confidence interval; Clp = plasma clearance; CSUCPS = Colorado State University Cat Pain Scale; DIVAS = dynamic interactive visual analogue scale; DEXM = dexmedetomidine; EPI = epidural; IVAS = interactive visual analogue scale; KETO = ketoprofen; MAC = minimum alveolar concentration; MEDET = medetomidine; MEL = meloxicam; MET = methadone; MNT = mechanical nociceptive threshold; MOR = morphine; NRS = numerical rating scale; OHE = ovariohysterectomy; OTM = oral transmucosal; OXY = oxymorphone; P = pethidine; PK = pharmacokinetics; SAL = saline; SDS = simple descriptive scale; SRB = sustained release buprenorphine; T½ el = elimination half-life; TD = transdermal; TNT = thermal nociceptive threshold; VAS = visual analogue scale; Vdss = volume of distribution at steady state; VFF = von Frey filaments
In experimental studies buprenorphine 0.01–0.02 mg/kg given IV or IM had a thermal antinociceptive effect lasting from 30 mins to 12 h.34,46,73 The dose-related antinociceptive effects of intravenous buprenorphine have been investigated; buprenorphine 0.02 mg/kg and 0.04 mg/kg produced a greater degree of mechanical antinociception than the 0.01 mg/kg dose, but no dose-related response was found with a thermal threshold model. 70
Clinical studies have indicated that buprenorphine appears to be an effective analgesic in cats undergoing various procedures including ovariohysterectomy, onychectomy and orthopaedic surgery.53,65,69,77,78
The pharmacokinetics of buprenorphine administered by the IV, IM, SC, transdermal and OTM routes have been described.46,52,64,72 Buprenorphine has good bioavailability when administered by the OTM route and experimental studies suggested that it was both effective and well tolerated by cats.46,76,81 Clinical studies have reported conflicting results regarding the analgesic efficacy of OTM buprenorphine.67,68,75 This is possibly due to the timing of drug administration, the concomitant use of α2-adrenoreceptor agonists (which could cause vasoconstriction and potentially reduce the uptake of buprenorphine across the oral mucous membranes), and the volume and dilution of buprenorphine. Experimental data suggested that SC and transdermal administration of buprenorphine resulted in erratic absorption and disposition, and a limited intensity of antinociception.32,64,72
Two studies evaluated the thermal antinociceptive effects of epidurally administered buprenorphine, which lasted from 1–10 h and from 15 mins to 24 h, at doses of 0.0125 mg/kg and 0.02 mg/kg, respectively.71,79 In another study, epidural administration of buprenorphine did not reduce the MAC of isoflurane. 74
Vomiting and dysphoria are rarely associated with buprenorphine administration and its efficacy and long duration of action make it a good analgesic for cats in the perioperative period. The reported variability in intensity and duration of analgesia reflects the different doses and routes of administration used in different studies. These factors, coupled with the differences in response between cats, emphasise why it is important to monitor the response to treatment and titrate analgesic therapy to suit the individual’s needs.
A sustained-release preparation of buprenorphine that may produce analgesia for up to 72 h after SC injection has been produced; this shows promise for providing analgesia in cats following ovariohysterectomy, as it was as effective as the standard formulation of buprenorphine administered by the OTM route q12h. 66 Very recently, the safety of long-acting buprenorphine administered SC has been tested in young cats. 80 Cats were administered buprenorphine for 9 consecutive days at a dose of 0.24, 0.72 or 1.20 mg/kg/day. These doses represent 1 x, 3 x and 5 x the licensed dose and they were reported to be well tolerated by cats.
A review of studies describing the clinical application of buprenorphine in cats is now available. 82
Butorphanol
Butorphanol is a synthetic opioid analgesic with agonist/antagonist activity. 83 Its pharmacology is complex and it has species-specific affinity for the μ-, δ- and κ-opioid receptor subtypes. 84 Butorphanol has a marketing authorisation for use in cats in several European countries and in North America, where it is widely used. In general, butorphanol is administered at doses from 0.1–0.4 mg/kg via the IV, IM or SC route. The OTM route has been investigated but it was not efficacious due to the limited systemic absorption in comparison with IM administration. 85
Many experimental studies have evaluated the analgesic effects of butorphanol. Some of the results are summarised in Table 4. The effects and duration of action vary according to the dose administered, the route of administration, the type of pain studied (visceral, somatic) and the type of pain model (electrical, mechanical, thermal threshold, colonic balloon, surgery).34,45,73,89,90,94,95,98,99 Experimental studies suggest that butorphanol provides short-lasting antinociception lasting from 5–165 mins,34,45,89,90,94,95 with the exception of one study where thermal nociceptive threshold values were increased for up to 8 h after 0.2 mg/kg butorphanol IM. 73 Early clinical studies showed that butorphanol decreased the stress response to surgery,100,101 and provided more analgesia than saline in cats undergoing onychectomy. 102 Subsequent studies reported that butorphanol administered to cats undergoing onychectomy or onychectomy plus neutering provided short-lasting analgesia for up to 2 h.30,96,97
Studies evaluating butorphanol in cats

See footnote to Table 1
ACE = acepromazine; B = buprenorphine; BUPI = bupivacaine; BUT = butorphanol; CAR = carprofen; Cl = apparent clearance; Cmax = maximum plasma concentration; DEXM = dexmedetomidine; DIVAS = dynamic interactive visual analogue scale; F = relative bioavailability; GA = general anaesthesia; HYDRO = hydromorphone; KETA = ketamine; IVAS = interactive visual analogue scale; MAC = minimum alveolar concentration; MEL = meloxicam; MET = methadone; MID = midazolam; MEDET = medetomidine; MNT = mechanical nociceptive threshold; NRS = numerical rating scale; OHE = ovariohysterectomy; OTM = oral transmucosal; PETH = pethidine; PK = pharmacokinetics; SAL = saline; SAP = systolic arterial pressure; SDS = simple descriptive scale; SEVO = sevoflurane; T1/2 el = elimination half-life; T = tramadol; TFP = transdermal fentanyl patch; TNT = thermal nociceptive threshold; VAS = visual analogue scale; Vd = apparent volume of distribution
In a multicentre study, butorphanol (0.4 mg/kg) provided poorer analgesia, and for a shorter time duration, than buprenorphine (0.01–0.02 mg/kg) after a variety of surgeries. 69 In contrast to these findings, another study, of cats undergoing ovariohysterectomy, 65 reported no differences in analgesia between cats receiving butorphanol vs buprenorphine; these results may reflect the fact that an NSAID was administered in combination with the opioid prior to surgery. 65 NSAIDs have been reported to be more efficacious analgesics in the postoperative period than butorphanol in cats undergoing ovariohysterectomy and onychectomy,92,93 but another study showed similar pain-associated behaviour after ovariohysterectomy. 91
Butorphanol has isoflurane and sevoflurane MAC-sparing effects;16,18 moreover, butorphanol is a versatile agent that can be used in combination with other drugs to provide the sedation required to perform clinical and diagnostic procedures when only mild pain is anticipated.51,86,87 Most clinical studies report a few hours’ analgesic effect for butorphanol;93,100,101 those reporting a longer duration of action included repeat dosing.30,97,102 Frequent re-dosing in order to provide analgesia would be impractical when pain is expected to last for a long period postoperatively. 7
Morphine
Morphine is a full agonist at the µ, δ and  opioid receptors.
103
Although morphine is not licensed for use in veterinary species, it is generally considered the ‘gold standard’ opioid.
104
Several of the experimental and clinical studies that have evaluated the use of morphine in cats are summarised in Table 5.
opioid receptors.
103
Although morphine is not licensed for use in veterinary species, it is generally considered the ‘gold standard’ opioid.
104
Several of the experimental and clinical studies that have evaluated the use of morphine in cats are summarised in Table 5.
Studies evaluating morphine in cats

See footnote to Table 1
B = buprenorphine; bpm = beats per minute; BUPI = bupivacaine; BUT = butorphanol; Clp = plasma clearance; EPI = epidural; HYDRO = hydromorphone; MAC = minimum alveolar concentration; MAP = mean arterial pressure; MNT = mechanical nociceptive threshold; MOR = morphine; PK = pharmacokinetics; SAL = saline; SDS = simple descriptive scale; T = tramadol; T½ el = elimination half-life; TNT = thermal nociceptive threshold; VAS = visual analogue scale; Vdss = volume of distribution at steady state
Pharmacokinetic data for morphine (0.2 mg/kg IV and IM) have been reported. 52 In comparison with other species, the production of the metabolite morphine-6-glucuronide is limited in cats. Morphine-6-glucuronide is responsible for some of morphine’s analgesic effects in people, 109 and the lack of production of this metabolite in cats may be the reason why morphine (0.1 mg/kg) appears to be less effective than buprenorphine (0.01 mg/kg) in cats undergoing various surgeries or invasive diagnostic procedures. 77
Thermal nociceptive threshold testing has been used to evaluate morphine (0.2 mg/kg IM); the thermal threshold was increased from 4–6 h after injection. 34 When the same dose was administered SC, an increase in thermal threshold was measured 45 mins and 1 h after injection and pressure thresholds were increased compared with baseline at 45–60 mins and 3–6 h after injection. 32 Adverse effects after IV injection are vomiting and histamine release. 49 Morphine’s relative hydrophilicity means that its administration by the epidural or subarachnoid route provides long lasting analgesia.49,71,103,107 Morphine can also be combined with bupivacaine and administered by the epidural route. 108 Hypotension is a side effect of epidural anaesthesia with local anaesthetic agents, while very rarely reported side effects of morphine also include urinary retention, pruritus, and chronic urinary and bowel dysfunction.105,106,108
Morphine can also exert a significant isoflurane MAC-sparing effect when administered at a dose of 1 mg/kg IV, but this dose is considerably higher than that usually used in clinical settings and physiological and behavioural effects were not reported. 16 Until the behavioural and physiological effects of such a high dose are established, it would be prudent to continue to use more conventional doses (0.1–0.2 mg/kg) when administering morphine by the IV route.
Hydromorphone
Hydromorphone is a semi-synthetic full µ-agonist analgesic that is widely used in the United States. It does not have a marketing authorisation for administration to animals in Europe. It has higher potency than morphine. 110 The analgesic effects of hydromorphone are similar to those of oxymorphone, but it is cheaper.111,112
Adverse effects in cats include hypersalivation, nausea, vomiting, respiratory depression and postanaesthetic hyperthermia.111 –113 In patients admitted to an intensive care unit for painful procedures, hydromorphone (0.05 mg/kg) appeared to provide adequate analgesia with a similar efficacy to oxymorphone. 112 IV administration of 0.1 mg/kg hydromorphone was more efficacious than a 0.025 or 0.05 mg/kg dose in a thermal antinociception model. 114 The epidural administration of 0.05 mg/kg hydromorphone caused thermal and some mechanical antinociception without hyperthermia. 115
SC administration of hydromorphone provides a slower onset of peak effect, shorter duration of antinociception and more undesirable side effects (emesis and salivation) than IV or IM administration, so this route of administration is not recommended. 116 Hydromorphone increases skin temperature in cats; patients should be monitored closely for postanaesthetic hyperthermia.39,113 It also has sevoflurane MAC-sparing effects. 18
Studies evaluating hydromorphone are summarised in Table 6.
Studies evaluating hydromorphone in cats

See footnote to Table 1
B = buprenorphine; BUT = butorphanol; Cl = clearance; EPI = epidural; HYDRO = hydromorphone; KETA = ketamine; MAC = minimum alveolar concentration; MNT = mechanical nociceptive threshold; OHE = ovariohysterectomy; OTM = oral transmucosal; OXY = oxymorphone; PK = pharmacokinetics; SAL = saline; T = tramadol; TNT = thermal nociceptive threshold; T1/2β = terminal half-life; Vc = apparent volume of distribution of the central compartment; Vdss = apparent volume of distribution at steady state
Oxymorphone
Oxymorphone is a semi-synthetic derivative of morphine, characterised by higher potency (lower dose required) and a faster onset of action than morphine. 118 Like hydromorphone, it is used in the USA but it does not have a marketing authorisation for administration to animals in Europe.
Pharmacokinetic data after IV administration of 0.1 mg/kg oxymorphone suggest a moderate volume of distribution and a short terminal half-life. 119 Oxymorphone administration does not seem to be associated with vomiting, hyperthermia or adverse behavioural changes and the clinical efficacy of oxymorphone is comparable with hydromorphone, the latter being cheaper.111,112 When compared with buprenorphine in cats undergoing onychectomy or onychectomy and neutering, oxymorphone seemed to be a less effective analgesic; however, as commented by the authors of the study, the results might have been influenced by the methodology of measuring pain, and it would have been appropriate to include other more sensitive evaluations. 78
Studies evaluating oxymorphone are summarised in Table 7.
Studies evaluating oxymorphone in cats

See footnote to Table 1
B = buprenorphine; Cl = clearance; HYDRO = hydromorphone; OXY = oxymorphone; PK = pharmacokinetics; KETO = ketoprofen; T1/2β = terminal half-life; VAS = visual analogue scale; Vc = apparent volume of distribution of the central compartment; Vss = apparent volume of distribution at steady state
Fentanyl
Fentanyl is a very potent short-acting, lipid soluble, synthetic µ agonist. 49 Studies evaluating fentanyl in cats are summarised in Table 8.
Studies evaluating fentanyl in cats

See footnote to Table 1
ALF = alfentanil; BUPI = bupivacaine; BUT = butorphanol; Css = concentration at steady state; Clp = plasma clearance; EPI = epidural; FEN = fentanyl; GA = general anaesthesia; IPPV = intermittent positive pressure ventilation; ISO = isoflurane; LD = loading dose; MAC = minimum alveolar concentration; MAP = mean arterial pressure; MED = medetomidine; MIR = minimum infusion rate; MNT = mechanical nociceptive threshold; OHE = ovariohysterectomy; PK = pharmacokinetics; PPF = propofol; Rab = rate of absorption; SAL = saline; SDS = simple descriptive scale; SUF = sufentanil; T½ el = elimination half-life; TD = transdermal; TFP = transdermal fentanyl patch; TNT = thermal nociceptive threshold; Vdβ = apparent volume of distribution
A pharmacokinetic study of IV administered fentanyl in cats reported rapid distribution and elimination. 128 A more recent study showed that, following a single dose of fentanyl (10 µg/kg IV), the onset of action was rapid and thermal antinociception could be detected from 5–110 mins; antinociception was detected at plasma values higher than 1.07 ng/ml. 122 In conscious cats, the pharmacokinetics and pharmacodynamics of a 5 µg/kg/h fentanyl infusion, following a 5 µg/kg loading dose, and its effect on mechanical and thermal threshold have recently been studied. 120 Side effects consisted of mild sedation and salivation following the loading dose in 1/7 cats; antinociception could be detected at fentanyl plasma concentrations higher than 1.3 ng/ml. In an experimental setting an infusion of fentanyl at 6 µg/kg/h combined with a continuous rate infusion of propofol resulted in satisfactory anaesthesia in cats. 41 One clinical study in injured cats undergoing anaesthesia reported that a fentanyl infusion (20 µg/kg/h) combined with a propofol infusion (12 mg/kg/h) maintained the haemodynamic variables better than fentanyl and isoflurane anaesthesia, although respiratory depression was more marked and intermittent positive pressure ventilation was required. 121
The analgesic and cardiovascular effects of epidural fentanyl (4 µg/kg) have been evaluated in isoflurane-anaesthetised cats. Electrical threshold was increased 20 mins post-injection and no side effects were reported in one study. 129 In a separate study by the same investigators cardiopulmonary effects included a decrease in mean arterial pressure, heart rate and respiratory rate from 5–120 mins post-injection, and an increase in arterial partial pressure of carbon dioxide from 15–120 mins post-injection. 130
The need for a ‘hands off’ approach to longer-term analgesia in cats led to an interest in transdermally administered fentanyl and many studies have been carried out over the past 15 years.19,30,97,123 –128 In a pharmacokinetic study, steady state plasma concentrations were reached 12–24 h after the application of a fentanyl patch (25 µg/kg). Sustained plasma fentanyl concentrations were detected throughout a 5 day period, with a mean concentration at steady state of 1.58 ng/ml. The mean calculated delivery rate of fentanyl was 8.48 µg/h, with high variability among cats. 128 A few clinical studies have suggested that fentanyl patches can be considered effective analgesics in cats undergoing onychectomy or ovariohysterectomy;30,97,123,127 however, if a fentanyl patch is chosen to provide perioperative analgesia, the patch has to be applied 12–24 h before the surgical procedure.7,19,124,128
It is important to note that the presence of a fentanyl patch does not negate the need for pain assessment. In fact, this becomes imperative since there is considerable variability in the absorption of fentanyl, and thus analgesic efficacy. Also, a cat with a painful condition will require administration of additional analgesics, particularly in the time before the fentanyl patch becomes effective. The primary advantages of administering fentanyl by the transdermal route are the avoidance of repeated injections and a decrease (approximately 18%) in the MAC of isoflurane, which may promote more stable haemodynamics during anaesthesia.19,30 Moreover this method of fentanyl delivery can be used in cats weighing less than 4 kg by decreasing the amount of patch-exposed surface area. 124
However, there are also some disadvantages associated with the use of fentanyl patches. As mentioned, there is great individual variability in drug absorption by this method.19,128 Although anaesthesia and/or surgery do not appear to alter plasma fentanyl concentrations, hypothermia during anaesthesia can cause a reduction in serum fentanyl concentration.125,126 Skin permeability, altered skin perfusion and hypovolaemia are other factors that may affect plasma levels of fentanyl. 7 For all of these reasons, cats with transdermal fentanyl patches should be carefully monitored (mental status, behaviour, physiological variables) to assess efficacy and any potential adverse effects.126,128
There are also important safety considerations associated with the use of fentanyl patches, particularly if cats are discharged into their owners’ care after application of the patch. Fentanyl is an addictive drug that can be abused by people, and the risk of ingestion by the treated animal, other animals or humans has to be considered. There are reports of fatalities caused by ingestion of fentanyl patches by children and drug addicts, among others, as well as by monkeys.131 –133 There may also be legal implications associated with dispensing fentanyl patches; in the UK, fentanyl is a Schedule 2 controlled drug.
MAC reduction reported 24 h after placement of a 25 µg/h fentanyl patch (corresponding to a possible delivery dose of 5.8 µg/kg/h) and antinociception after fentanyl infusion of 5 µg/kg/h were achieved with different fentanyl plasma levels, of 0.54 ± 0.41 and >1.3 ng/ml, respectively.19,120
Fentanyl analogues
Alfentanil, remifentanil and sufentanil are potent µ agonists of the anilidopiperidine family and are characterised by a more rapid onset of action and shorter context-sensitive half-life after prolonged infusion in comparison with the structural analogue fentanyl. 134 They are used mainly in the intraoperative period. 49 These are Schedule 2 controlled drugs in the UK and do not have marketing authorisations for administration to animals. In the UK they can only be prescribed under the ‘cascade’ when their use can be justified in an individual animal and with informed owner consent. Further information on the use of the cascade and unlicensed drugs in the UK can be found on the Veterinary Medicines Directorate website (www.gov.uk/government/organisations/veterinary-medicines-directorate).
Alfentanil
Studies evaluating alfentanil in cats are summarised in Table 9. Alfentanil administered IV to conscious cats at a dose of 50 µg/kg produced analgesic effects for approximately 21 mins, as assessed by applying a clamp to the base of the tail, and the alfentanil was rapidly metabolised. 137 Recently the disposition of alfentanil in isoflurane-anaesthetised cats was studied. 135 The results were broadly similar to those published by Pascoe et al, 137 but the volume of the central compartment and volume of distribution at steady state were greater. 135 The same research group showed that plasma levels of alfentanil of 500 ng/ml had MAC-sparing effects on isoflurane, which, compared with isoflurane alone, increased heart rate, mean arterial pressure, stroke index, cardiac index, haemoglobin and oxygen delivery index, and blunted haemodynamic responses to a noxious stimulant. 28 Another study showed that a plasma alfentanil concentration of 500 ng/ml produced a maximal isoflurane MAC reduction of 35%; mild metabolic acidosis and decreased arterial partial pressure of oxygen were reported as adverse effects. 20
Studies evaluating alfentanil in cats
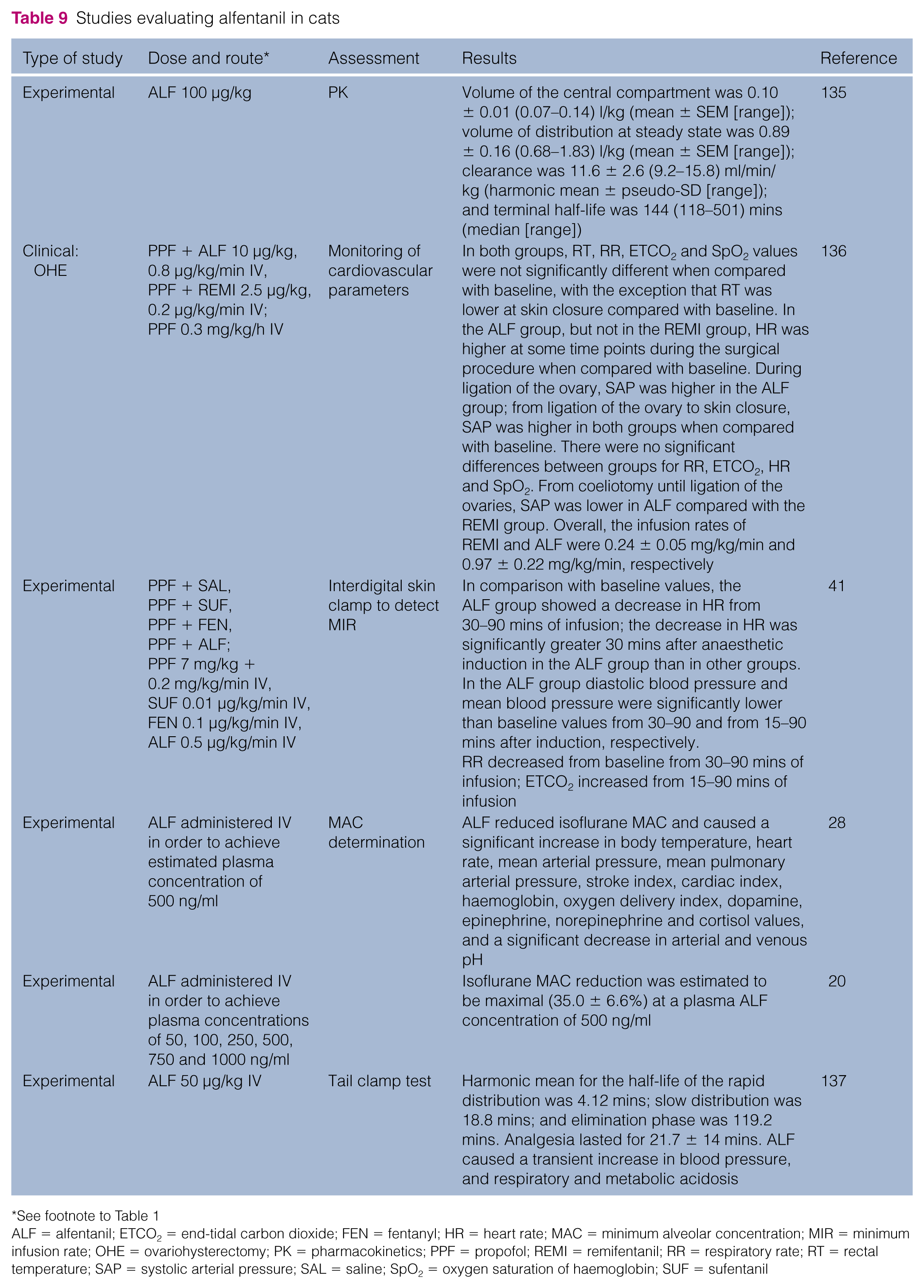
See footnote to Table 1
ALF = alfentanil; ETCO2 = end-tidal carbon dioxide; FEN = fentanyl; HR = heart rate; MAC = minimum alveolar concentration; MIR = minimum infusion rate; OHE = ovariohysterectomy; PK = pharmacokinetics; PPF = propofol; REMI = remifentanil; RR = respiratory rate; RT = rectal temperature; SAP = systolic arterial pressure; SAL = saline; SpO2 = oxygen saturation of haemoglobin; SUF = sufentanil
A clinical study evaluated total IV anaesthesia with propofol (0.2 mg/kg/min) alone or in combination with fentanyl (0.1 µg/kg/min), alfentanil (0.5 µg/kg/min) or sufentanil (0.01 µg/kg/min) infusions. In cats treated with alfentanil, diastolic blood pressure and mean blood pressure were significantly decreased compared with baseline from 30–90 and from 15–90 mins after induction, respectively. 41 More recently, a clinical study evaluated the combination of alfentanyl and propofol in cats undergoing ovariohysterectomy: propofol was infused at 0.3 mg/kg/h while the overall infusion rate of alfentanil was 0.97 ± 0.22 µg/kg/min. 136 In this study intermittent assisted ventilation was provided during anaesthesia in order to maintain normocapnia.
Remifentanil
Remifentanil is metabolised by non-specific plasma and tissue esterases. 138 In people and dogs it is characterised by a short context-sensitive half-time (time required for the plasma concentration to decrease by 50% after termination of an infusion) that does not depend on the duration of the infusion; thus there are no cumulative effects after prolonged infusions.139,140 Moreover, the extrahepatic metabolism of remifentanil is potentially advantageous in cats that lack some hepatic metabolic pathways,52,141 and especially in cats with liver and kidney disease.
Studies evaluating remifentanil in cats are summarised in Table 10. Pharmacokinetics data have been published. In conscious and isoflurane-anaesthetised cats an IV infusion of remifentanil at 1 µg/kg/min over 5 mins resulted in a rapid distribution to peripheral compartments, and a high clearance and a relatively short terminal half-life (17.4 and 15.7 mins in awake and anaesthetised cats, respectively). 142 Anaesthesia decreased the volume of the central compartment. 142 However, another study in cats showed that the MAC of isoflurane decreased significantly after a 30 min remifentanil infusion; 21 according to the authors this might have been caused by a ‘cumulative effect of repeated infusions of remifentanil or by a modified response to the repeated electrical stimulation’ (electrical stimulation was the method used to determine MAC), or by the use of ‘high doses which might have facilitated the cumulative effects’. 21 In the same study, three remifentanil constant rate infusions (CRIs) were examined, 0.25, 0.5 and 1 µg/kg/min, and the MAC reduction from baseline ranged from 23–30% with no statistical difference between groups. This may mean that there is a ceiling to the isoflurane-sparing effect. The study also reported that the remifentanil CRI was associated with an increase in heart rate of 26% and an increase in systolic arterial pressure of 23%. 21
Studies evaluating remifentanil in cats

See footnote to Table 1
ALF = alfentanil; Cl = clearance; ETCO2 = end-tidal carbon dioxide; HR = heart rate; ISO = isoflurane; LD = loading dose; MACREMI 0.25 = isoflurane minimum alveolar concentration determined during infusion of 0.25 µg remifentanil/kg/min; MAC = minimum alveolar concentration; MACBASAL = basal isoflurane minimum alveolar concentration; MACREMI 0.5 = isoflurane minimum alveolar concentration determined during infusion of 0.5 µg remifentanil/kg/min; MACREMI 1 = isoflurane minimum alveolar concentration determined during infusion of 1 µg remifentanil/kg/min; mmHg = millimetres of mercury; OHE = ovariohysterectomy; PK = pharmacokinetics; PPF = propofol; REMI = remifentanil; RR = respiratory rate; RT = rectal temperature; SAP = systolic arterial pressure; SBP = systolic blood pressure; SpO2 = oxygen saturation of haemoglobin; TNT = thermal nociceptive threshold; T1/2β = terminal half-life; Vc = apparent volume of distribution of the central compartment; Vss = apparent volume of distribution at steady state
IV infusion of remifentanil was shown to result in a dose-dependent increase in thermal threshold in conscious cats. 15 Behaviours suggestive of euphoria were apparent in conscious cats when infusion rates were equal to or higher than 1 µg/kg/min. In the same study a relationship between the immobilising potency of remifentanil, assessed as a MAC-sparing effect, and analgesic potency was not detected; nor was hyperalgesia detected on termination of the infusion. 15 Another study evaluated remifentanil infusions in association with propofol anaesthesia (0.3 mg/kg/min). 143 Remifentanil infusion rates ranging from 0.2–0.27 µg/kg/min were necessary in cats undergoing ovariohysterectomy to prevent cardiovascular responses, while a remifentanil CRI of 0.3 µg/kg/min was necessary to prevent motor responses to electrical stimulation. Bradycardia (lowest heart rate recorded = 68 beat per minutes) and hypotension (lowest mean arterial pressure = 49 mmHg) were noted in some cats. 143 Similarly, in an investigation involving propofol-anaesthetised cats (0.3 mg/kg/min) undergoing ovariohysterectomy, the time to extubation of the trachea was faster in cats that received a remifentanil infusion at 0.24 ± 0.05 µg/kg/min than in those that received an alfentanil infusion at 0.97 ± 0.22 µg/kg/min. 136
It must be emphasised that in the aforementioned clinical studies intermittent positive pressure ventilation was required as remifentanil produces a significant degree of respiratory depression. 140
Sufentanil
Sufentanil has a more rapid onset and shorter duration of action than fentanyl in people. 144 Sufentanil administration can elicit centrally mediated sympathetic stimulation, resulting in effects such as an increase in blood pressure and heart rate. 27
Studies evaluating the use of sufentanil in cats are summarised in Table 11. To the authors’ knowledge, there are currently no published studies evaluating the analgesic or antihyperalgesic effects of sufentanil in cats. Very recently an experimental study evaluated the pharmacokinetics of sufentanil in isoflurane-anaesthetised cats and demonstrated that the drug has a rapid disposition due to a small volume of distribution and moderate clearance. 135 An experimental study evaluated the cardiorespiratory effects of propofol (induction dose of 7 mg/kg, followed by an infusion at 0.2 mg/kg/min IV) alone or in combination with sufentanil (loading dose of 0.1 µg/kg, followed by an infusion at 0.01 µg/kg/min IV). 41 The cats breathed spontaneously during the 90 min study period, although an increase in expired carbon dioxide level, up to 69 mmHg, was noted, as well as a decrease in respiratory rate and heart rate in comparison with baseline values. Mean blood pressure and oxygen saturation did not change from baseline. 41
Studies evaluating sufentanil in cats

See footnote to Table 1
ALF = alfentanil; ETCO2 = end-tidal carbon dioxide; FEN = fentanyl; HR = heart rate; MIR = minimum infusion rate; PK = pharmacokinetics; PPF = propofol; RR = respiratory rate; SAL = saline; SUF = sufentanil
Tramadol
Tramadol is a centrally acting analgesic, consisting of two enantiomers, which exerts its analgesic effect by binding to the opioid receptors (mainly µ) and by interfering with the neuronal release and reuptake of serotonin and noradrenaline in the descending inhibitory pathways. 145 The (+) enantiomer and its metabolite O-desmethyltramadol (M1) bind the opioid receptors and appear to contribute significantly to the analgesic effect of tramadol. The opioid effect of tramadol is believed to be related, at least in part, to its metabolite O-desmethyltramadol. In cats O-desmethyltramadol rapidly appears in plasma following tramadol administration and has a moderate half-life. 146
Tramadol does not have a marketing authorisation for use in cats, but is licensed for use in dogs in some European countries. There is a great deal of interest in using tramadol for analgesia in companion animals. It is available in tablet form, facilitating administration by owners at home, and could be an alternative to NSAIDs in cats in which these drugs are poorly tolerated and/or contraindicated, or used in addition to NSAIDs in animals with more severe pain.
Tramadol has recently been classified as a Schedule 3 controlled drug in the UK, but exempted from the safe custody requirements, and is a Schedule IV drug under the Federal Controlled Substances Act in the United States. The potential for human abuse should be carefully considered, as well as the potential for toxicity in cats. Recently, symptoms related to serotonin syndrome secondary to tramadol overdose (80 mg/kg administered PO twice) have been reported for the first time in a cat. 147 The serotonin syndrome is induced by pharmacological treatment with serotonergic agents that increase serotonin activity, including selective serotonin reuptake inhibitors, tricyclic antidepressants (amitriptyline), monoamine oxidase inhibitors, lithium, carbamazepine, amphetamine and derivatives, dextromethorphan, tramadol and meperidine; and also by St John’s wort (Hypericum perforatum). In people symptoms include cognitive behavioural changes, neuromuscular excitability and autonomic instability. 148
Studies evaluating the use of tramadol in cats are summarised in Table 12. Experimental studies have investigated the antihyperalgesic and MAC-sparing effects of various doses of tramadol administered by the SC, epidural or PO route. Steagall and colleagues reported that tramadol (1 mg/kg) administered by the SC route had no effect on mechanical nociceptive thresholds and only a limited effect on thermal thresholds, which increased above the 95% confidence interval only at 45 mins, 3 and 6 h. 35 Moreover, large variability in the antinociceptive response to tramadol was detected between cats. In the same study tramadol combined with acepromazine increased the pressure threshold values from 30 mins to 3 h after administration. This finding was unexpected since no antinociceptive effects were detected when tramadol was administered alone, and acepromazine is generally considered not to be analgesic. 154 It is possible that the acepromazine enhanced the tramadol-induced analgesia.
Studies evaluating tramadol in cats

See footnote to Table 1
ACP = acepromazine; BUT = butorphanol; CPS = composite pain score; EPI = epidural; HYDRO = hydromorphone; IVAS = interactive visual analogue scale; MAC = minimum alveolar concentration; MNT = mechanical nociceptive threshold; MOR = morphine; OHE = ovariohysterectomy; PK = pharmacokinetics; SAL = saline; SDS = simple descriptive scale; T = tramadol; TNT = thermal nociceptive threshold; VFF = von Frey filaments; VAS = visual analogue scale; VEDA = vedaprofen
In another study the thermal antinociceptive effects of 0.5–4 mg/kg tramadol administered PO were investigated. 150 A dose-dependent antinociceptive effect was detected and significant analgesic effects that lasted up to 6 h were reported with doses of 2 and 4 mg/kg. In the same study a pharmacokinetic simulation was performed and it was predicted that a dose of 4 mg/kg q6h would maintain adequate analgesia in cats.
Orally administered tramadol (8.6–11.6 mg/kg) produces a significant reduction in the MAC of sevoflurane from 2.45 ± 0.2% to 1.48 ± 0.2%, and so it could be used in a multimodal anaesthetic protocol. 18 Another experimental study compared the effect of 1 mg/kg tramadol or 0.1 mg/kg morphine administered by the epidural route in cats with the use of a tail clamp test. 107 Tramadol provided analgesia comparable to morphine for up to 6 h, while morphine provided superior analgesia from 6–12 h after administration. The use of preservative-containing preparations of tramadol for epidural injection should be avoided as the toxicity of the preservatives on neuronal tissue in cats has not been established. Preservative-free preparations of tramadol are available in some countries.
In a clinical study, cats undergoing elective ovariohysterectomy received tramadol (2 mg/kg SC q8h for 3 days) or vedaprofen (0.5 mg/kg PO q24h for 3 days) alone or in combination. Cats receiving the two drugs combined had lower pain scores than cats that received one or other of the drugs on its own. 151 Haemostatic, biochemical and gastrointestinal function was not affected by the perioperative use of vedaprofen and/or tramadol in cats. 152 More recently, tramadol (2 mg/kg IV) provided adequate analgesia after neutering for up to 6 h. 149 In the aforementioned studies respiratory depression was not noted; however, in an experimental study in cats, tramadol at 2 and 4 mg/kg administered IV in α-chloralose-urethane anaesthetised cats exerted a depressant effect on ventilation by reducing the sensitivity of peripheral and central chemoceptors to carbon dioxide and increasing the apnoeic threshold. 153
Naloxone
Naloxone is a pure opioid antagonist, with no intrinsic effect, used to antagonise the effects of opioids. It antagonises the analgesic effects as well as the adverse effects such as excessive sedation, bradycardia and respiratory depression.49,155 Naloxone has a rapid onset of action (1–2 mins) and a duration of effect of approximately 30–60 mins. 155 It should be administered slowly IV (0.002–0.04 mg/kg). Renarcotisation can occur when the duration of action of the opioid agonist is longer than the antagonist. 155 The appropriate dosage in cats has not been evaluated. The authors would suggest preparing a syringe with 0.002 mg/kg of naloxone diluted with saline and titrating administration to effect; ie, until the adverse effects of opioids have disappeared. Some clinicians have suggested that if naloxone is not available, butorphanol can be used for antagonism of respiratory depression, while maintaining a certain degree of analgesia, but there are no studies evaluating this in cats. Nevertheless, butorphanol was used to reverse the effects of fentanyl and sufentanil in rats and rabbits.156 –158 By contrast, in dogs, butorphanol was not proven to reverse oxymorphone-induced postoperative respiratory depression. 159
The effects of a combination of buprenorphine and naloxone have recently been investigated. In people and rats naloxone can enhance the analgesic/antihyperalgesic effects of buprenorphine. 160 However, this did not appear to be the case in cats and the study showed that naloxone antagonised the thermal antinociceptive effects of clinically analgesic doses of buprenorphine in cats (Table 13). 161
Studies evaluating naloxone in cats

See footnote to Table 1
B = buprenorphine; N = naloxone; MNT = mechanical nociceptive threshold; TNT = thermal nociceptive threshold
Conclusions
In summary, opioids can be used in cats, especially in cases of moderate to severe pain. Their effects should be closely monitored so that pain treatment is tailored to best suit the individual animal’s needs.
Footnotes
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
JFMS Premier Reviews are invited state-of-the-art review papers on key issues in feline medicine and surgery. Written by expert international authors, these reviews are made freely available to maximise their impact.