
Abstract
Practical relevance:
The field of veterinary medicine is constantly evolving. New medications are being introduced into clinical practice, and novel uses for established medications are frequently being discovered as new information comes to light.
Clinical challenges:
Therapeutic options for our feline patients can be restricted based on inadequate clinical evidence, adverse effects and patient compliance concerns. Additionally, with the reduced availability of commonly used medications in some regions, clinicians are forced to utilize alternatives with which they may have limited experience.
Audience:
This review article is directed towards primary care veterinarians working with feline patients. The selection of medications discussed is based on many of the clinical challenges commonly encountered in practice.
Evidence base:
The evidence for use of some of these medications is limited due to their novelty. Known mechanisms of action, pharmacokinetic and pharmacodynamics data, adverse effects and clinical uses are reviewed where possible, with clinical recommendations made based on the evidence of data available.
Robenacoxib
Non-steroidal anti-inflammatory drugs (NSAIDs) are frequently used medications in veterinary medicine, especially for the treatment of pain and inflammation associated with musculoskeletal disorders. Mechanistically, NSAID effects are achieved through the inhibition of cyclooxygenase (COX), the enzyme needed in the conversion of arachidonic acid to prostaglandins and thromboxane A2 (see box below). COX-1 is constitutively expressed in most tissues in the body and is responsible for the mediation of many physiological reactions including gastrointestinal (GI) mucosal defense. As such, many of the toxicities associated with NSAIDs (primarily GI) are thought to be due to inhibition of COX-1. COX-2 is expressed by cells involved in inflammation and is an inducible isoform that is largely responsible for the production of inflammatory prostaglandins; however, it is also expressed in other tissues, such as the kidney, rendering the kidney susceptible to toxicity as well.


Selective COX-2 inhibitors (the coxibs) were developed to block inducible cyclooxygenase, thus in theory leaving COX-1 and mucosal defenses intact. Subsequent investigation into the COX isomers has shown that the molecules are actually very similar, leading to the idea that it may be difficult to attain true selectivity. 1 Robenacoxib (Onsior; Novartis Animal Health) is a new highly selective COX-2 NSAID2,3 available for use in cats >2.5 kg and >6 months of age. In the United States, robenacoxib is approved by the Food and Drug Administration (FDA) for the treatment of postoperative pain and inflammation at a dosage of 1–2 mg/kg/day for a maximum of 3 days. In Europe, the 6 mg flavored tablets are approved for the treatment of acute pain and inflammation associated with musculoskeletal disorders in cats for 6 days. The 20 mg/ml solution for injection may be given at a dose of 2 mg/kg subcutaneously for up to 2 consecutive days for pain associated with both orthopedic and soft tissue surgery in Europe. Currently, there is no approval for injection followed by oral administration of robenacoxib.
When administered orally on an empty stomach, the bioavailability of robenacoxib is approximately 50%, and it decreases significantly when given after a meal. 4 The drug appears to be absorbed rapidly and reaches peak plasma concentrations in 30 mins in fasted patients. Food causes high variability in the time to reach maximum concentration (up to 8 h). 4 Consequently, robenacoxib should be given to cats on an empty stomach or with only a small amount of food. Although the drug has a short elimination half-life of approximately 45–60 mins, depending on route of administration, mean residence time in exudate at sites of inflammation is close to 24 h regardless of administration type. 5 This extended pharmacodynamic effect of robenacoxib allows for once daily dosing in cats.
Robenacoxib has been used effectively in cats for the treatment of acute pain and inflammation associated with musculoskeletal disorders,6,7 ovariohysterectomy 8 and other surgical procedures. 9 It is important to note that robenacoxib has not been evaluated for the treatment of chronic pain and inflammation; therefore, its current recommended use is limited to acute pain management. Robenacoxib appears to be well tolerated in these clinical trials as well. A safety study showed that oral robenacoxib is well tolerated in cats at doses as high as 10 mg/kg q12h for 42 days. 10 However, the population of this study was comprised of young, healthy cats all less than 1 year of age, making it extremely difficult to extrapolate this safety information to an older population.
NSAIDs should be used judiciously in cats with comorbidities such as renal, GI, hepatic or cardiac disease. 11 Evaluation of serum renal and liver parameters is recommended prior to use of robenacoxib. In cases of known renal or hepatic disease, dose reduction or alternative therapy (which may be achieved by adjunctive analgesia), as well as monitoring following treatment, is recommended.
With specific regard to renal disease, COX-2 is constitutively expressed in the mammalian kidney and is responsible for maintaining renal blood flow in response to states of actual or perceived decreases in intravascular volume. 12 NSAIDs will inhibit formation of prostaglandins and their compensatory effects in the kidneys in response to hypovolemia, which will lead to renal ischemia and acute kidney injury. As such, NSAIDs including robenacoxib should not be used in patients that are dehydrated or prior to anesthetic events where hypotension is a risk factor (Figure 1). Opioids should be considered for preoperative or perioperative analgesia. 11 It is our recommendation that NSAIDs be used in the postoperative period when the risk of hypotension is minimized. Additionally, owners should be specifically instructed to discontinue robenacoxib if the patient develops any clinical signs of systemic illness including anorexia, vomiting and diarrhea.

Due to the increased risk of acute kidney injury, robenacoxib, as well as other NSAIDs, should only be given to patients undergoing orthopedic (or soft tissue) surgery after recovery from general anesthesia. Courtesy of Sarah Dowling

Pradofloxacin
Fluoroquinolones are commonly used antibiotics in veterinary medicine. FDA-approved fluoroquinolones include enrofloxacin, orbifloxacin, difloxacin (dogs only), marbofloxacin and, recently, pradofloxacin. They are classified into generations based on differences in chemical structure that influence their spectrum of activity. 18 Enrofloxacin, difloxacin, marbofloxacin and ciprofloxacin are second-generation fluoroquinolones. Third-generation fluoroquinolones have an increased gram-positive and anaerobic spectrum, with orbifloxacin and pradofloxacin falling into this category. Pradofloxacin (Veraflox; Bayer HealthCare) is now licensed in Europe for a broad range of bacterial infections in dogs and cats, but is only licensed for cats in the USA.
The antibacterial action of fluoroquinolones is achieved through inhibition of topoisomerase activity. Pradofloxacin inhibits both topoisomerase I (DNA gyrase) and topoisomerase IV, resulting in a broader spectrum of activity compared with earlier generation fluoroquinolones. Pradofloxacin maintains excellent gram-negative coverage and has shown efficacy against Mycoplasma,19,20 Bartonella 21 and some intracellular bacteria such as Mycobacterium. 22 In addition, pradofloxacin has shown good anti-anaerobe activity in vitro; 23 however, its clinical efficacy in the treatment of anaerobic infections in vivo remains to be determined.
Reported indications for pradofloxacin in cats include infected wounds and abscesses, bacterial urinary tract infections, bacterial upper respiratory tract infections and hemotropic mycoplasmosis.19,24,25
In cats with upper respiratory infections due to Chlamydia felis or Mycoplasma species, pradofloxacin showed similar efficacy in terms of resolution of clinical signs as doxycycline; however, in some cats treated with pradofloxacin C felis DNA persisted. 20 Pradofloxacin has also shown equivalent efficacy (ie, clinical disease recovery) as doxycycline therapy in the treatment of experimental Mycoplasma hemofelis infection. In cats experimentally infected with M hemofelis, 6/12 cats treated with pradofloxacin (four administered 5 mg/kg/day, two administered 10 mg/kg/day) tested M hemofelis negative with quantitative PCR of blood at the end of the study, while none of the cats treated with doxycycline tested PCR negative, 19 suggesting that pradofloxacin may be effective in the treatment of M hemofelis infection in cats. However, negative PCR results alone should not be interpreted as a reliable marker of clearance of infection due to the potential for organism sequestration.
Rational indications for the clinical use of pradofloxacin include infections where gram-negative enteric organisms and anaerobes are expected, such as hepatobiliary infections, aspiration pneumonia and septic peritonitis, with empirical use reserved for serious life-threatening infections that are likely to be resistant to first-generation antibiotics. Pradofloxacin may also be a good choice for the treatment of pyothorax where Pasteurella and mixed anaerobes are expected. Pradofloxacin is unlikely to be clinically effective in the treatment of Nocardia infection despite lower mean inhibitory concentration (MIC50 and MIC90) values for Nocardia isolates compared with enrofloxacin and ciprofloxacin. 22 As with any antibiotic use, there is the concern of selecting for bacterial resistance with overuse or inappropriate use (see box on page 222); therefore, culture and susceptibility testing is recommended when possible to support the need for treatment with a third-generation fluoroquinolone.
Pradofloxacin is reported to be well tolerated in cats.19,24 A unique concern with this class of antibiotics in feline patients is acute diffuse retinal degeneration. This species-specific adverse reaction is dose-dependent and results from a deficiency in the ATP-binding cassette subfamily G member 2 protein (ABCG2). This protein’s role is to prevent xenobiotics, which include the photosensitive fluoroquinolones, from crossing the blood– retinal barrier into the retina. 26 Cats treated with high doses or given a moderate overdose of a fluoroquinolone, given rapid intravenous infusions, treated with a prolonged antibiotic course, or those with decreased clearance due to a decreased glomerular filtration rate are at increased risk of acute retinal degeneration and blindness. 27 This adverse reaction has not been reported with pradofloxacin or marbofloxacin. Pradofloxacin appears to have low retinotoxic potential, with no retinal changes noted at 50 mg/kg/day. 28 However, all fluoroquinolones should be considered to have the potential to cause retinal toxicity in cats (Table 1).
Summary of post-approval studies that have evaluated the dosage of veterinary-approved fluoroquinolones associated with retinal degeneration in young healthy cats
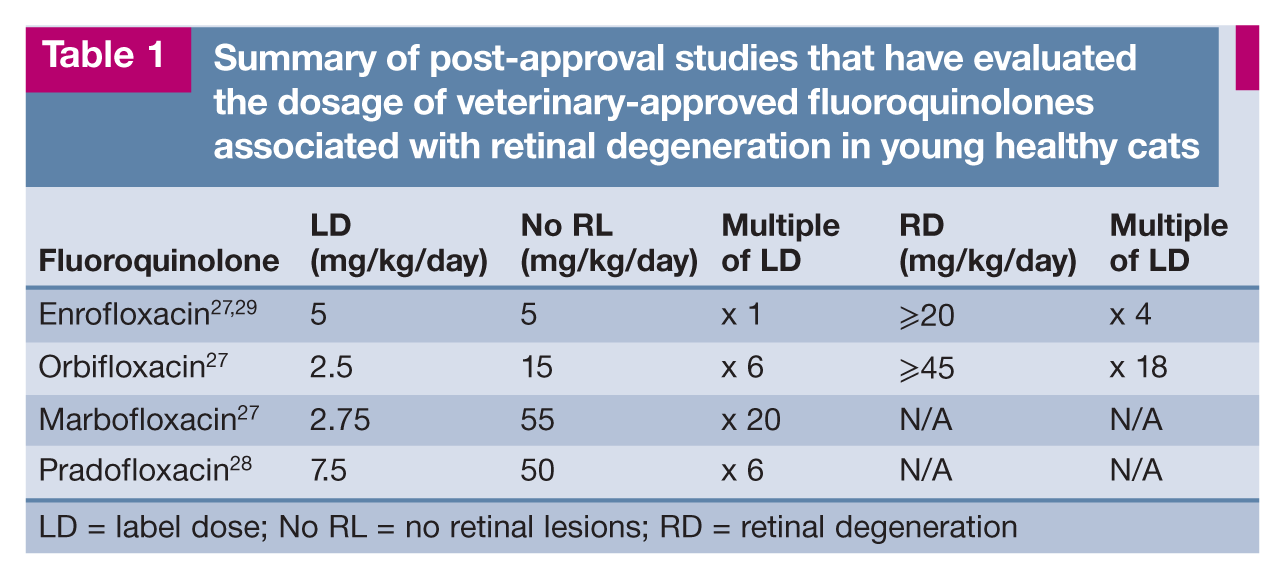
LD = label dose; No RL = no retinal lesions; RD = retinal degeneration
Cefovecin
Cefovecin (Convenia; Pfizer Animal Health) is a semi-synthetic third-generation cephalosporin approved for use in cats for skin and soft tissue infections such as pyoderma, wounds and abscesses,30,31 as well as for lower urinary tract infections. 32 It has bactericidal activity against gram-positive, gram-negative and anaerobic bacteria. However, its spectrum of activity is closer to first-generation antibiotics of this class, with coverage for Escherichia coli, Staphylococcus pseudintermedius and Pasteurella multocida but poor activity against Pseudomonas aeruginosa. As with other cephalosporins, cefovecin lacks activity against Enterococcus species. 33
Cefovecin is fully bioavailable when administered subcutaneously in cats. It reaches peak plasma concentrations in approximately 2 h and is over 99% bound to plasma proteins. 34 As a result, its half-life is extended (nearly 7 days), allowing it to maintain therapeutic concentrations against P multocida in plasma and dermal transudate as well as against E coli in urine for 14 days. Cefovecin’s extended elimination half-life enables less frequent dosing but precludes drug withdrawal after the development of adverse reactions as well as early antibiotic de-escalation, which may contribute to the development of antimicrobial resistance. Consequently, cefovecin is not an appropriate choice for surgical infection prophylaxis where only short-term therapy is required and the risk of colonizing postoperative patients with resistant bacterial strains may be increased. For example, the impact of cefovecin on fecal enteric flora was evaluated in healthy dogs following the administration of a single 8 mg/kg subcutaneous dose. 35 In the cefovecin-treated dogs the number of E coli isolates decreased and Enterococcus species isolates increased. In addition, significantly more cefovecin-resistant E coli was isolated in the cefovecin-treated dogs on days 7, 14 and 28.
Cefovecin is often an appealing antibiotic choice in cats because of its long duration of action and ability to ameliorate the concern for patient and client compliance, but its use in the treatment of common feline conditions that can be successfully treated without antibiotics or with narrower spectrum antibiotics needs to be questioned. For example, reported uses of cefovecin have included the treatment of conditions with low incidence of bacterial infections (ie, upper respiratory tract disease, most commonly caused by an underlying viral etiology, and lower urinary tract disease, commonly an inflammatory disease in this species). 14 Although the development of a secondary bacterial infection can complicate upper respiratory tract disease in some cats, the more common bacterial species associated with feline upper respiratory disease (eg, Mycoplasma species, Bordetella bronchiseptica and Chlamydophila felis) are not expected to be effectively treated with cefovecin. Both doxycycline and amoxicillin–clavulanic acid have displayed higher efficacy when compared with cefovecin for the treatment of upper respiratory tract disease in shelter cats in a randomized prospective clinical trial. 36
In our veterinary patients this long-duration-of-action cephalosporin should be considered a second-line antibiotic and used clinically based on culture and susceptibility testing. In the cephalosporin class, the third and fourth generations are considered to be critically important antimicrobial groups in human medicine that should be reserved to treat life-threatening diseases that have a limited number of therapeutic options.
Minocycline
Minocycline is a semi-synthetic antibiotic in the tetracycline class produced from natural antibiotics such as tetracycline and oxytetracycline. It is a broad-spectrum bacteriostatic antibiotic that inhibits protein synthesis by reversibly binding to the 30S ribosomal subunit. 37 It is highly lipophilic and able to cross the blood–brain barrier much more readily than doxycycline in dogs. 38 As a result of its highly lipophilic nature, it is a poorer choice for urinary tract infections compared with other tetracyclines.
Minocycline has a similar spectrum of activity as doxycycline. Susceptible organisms include some gram-positive species (eg, staphylococci and streptococci), gram-negative species (eg, Bartonella, Bordetella, Brucella and Pasteurella), as well as other species including spirochetes (Borrelia and Leptospira), Chlamydia, Mycoplasma, Rickettsia and Wolbachia. Common resistant species include E coli, Klebsiella, Bacteroides, Enterobacter, Proteus and Pseudomonas.
Tetracycline is routinely used as the class indicator for in vitro susceptibility testing. Tetracycline can reliably predict susceptibility to doxycycline and minocycline, but some bacterial isolates reported to be resistant to tetracycline may still be susceptible to doxycycline and minocycline. For example, methicillin-resistant S pseudintermedius (MRSP) isolates continue to be susceptible to minocycline despite developing resistance to tetracycline and doxycycline. 39 To differentiate antimicrobial susceptibility within this tetracycline class, a specialized assay is required to identify the presence of inducible resistance gene(s), and not all microbiology laboratories have a validated induction susceptibility assay.
Doxycycline is a widely used antibiotic in veterinary medicine. Due to the recent decrease in availability and increased cost of doxycycline in the United States, the use of minocycline as an alternative for doxycycline may increase in our veterinary patients in some geographic regions. The range of dosages recommended for cats varies anywhere from 5–25 mg/kg orally (PO) q12h, with most sources recommending doses within the lower half from 5–12.5 mg/kg. 40 Currently, there are no published studies on the pharmacokinetics of minocycline in cats. However, a pharmacokinetics study in cats that was recently presented as an abstract recommends a dosage of 8.8 mg/kg PO q24h (or 50 mg/cat PO q24h). 41 This dosage recommendation is consistent with a recent pharmacokinetics/pharmacodynamics study in dogs that indicated 5 mg/kg q12h should be an effective dosage in the treatment of S pseudintermedius with a minimal inhibitory concentration of <0.25 µg/ml. 42
The main side effect of minocycline appears to be GI upset, which may be ameliorated by administering the drug with or after a meal. In dogs, the concurrent administration of sucralfate significantly decreases the oral bioavailability of minocycline. However, oral bioavailability is not affected when sucralfate is given 2 h after minocycline. 43 It is recommended to avoid administration of minocycline as a rapid intravenous bolus because it has caused urticaria and hypotension in dogs. 44 Hepatotoxicity has also been reported secondarily to tetracycline administration in a cat; 45 therefore, clinicians should be cognisant of increases in serum alanine aminotransferase after prescribing this medication.
In cats, the risk of focal esophageal strictures associated with oral minocycline is unknown. This adverse effect has been reported with the hyclate (hydrochloride) salt of doxycycline when administered orally in cats.46,47 The mechanism responsible for this adverse effect in cats is thought to be similar to that in humans where the dissolution of a retained capsule or tablet coating in the esophagus leads to a caustic burn of the mucosa, resulting in fibrosis and a focal stricture. The risk of doxycycline-induced stricture formation can be reduced by use of an oral suspension or by following capsule or tablet administration with food or water. The administration of an oral suspension should be considered when prescribing minocycline (a hydrochloride salt) to a cat until more clinical experience is gained.
Tetracyclines can chelate calcium from teeth and bone, inhibit calcification and can cause tooth discoloration. As a member of the tetracycline class of antimicrobials, minocycline is excreted in the milk and has the potential to retard fetal skeletal development and discolor deciduous teeth. Therefore, use is best avoided in pregnant and nursing queens or young kittens unless the benefits outweigh the risks. Reproductive and nursing safety information specific to minocycline is unknown. In relation to drug safety during pregnancy, the FDA classifies tetracycline antibiotics as category D, meaning they are contraindicated (in pregnant humans) unless benefits outweigh the risks. Amoxicillin, amoxicillin–clavulanic acid, ampicillin, cephalexin, clindamycin, erythromycin and azithromycin are examples of antibiotics that are relatively safe and should be used in lieu of minocycline in pregnant or nursing queens or young kittens if possible.
Ciclosporin
Ciclosporin (cyclosporine) A (CsA) is a commonly used immunomodulatory medication in veterinary medicine. CsA binds to intracellular protein cyclophilin-1, forming a complex that inhibits calcineurin. As a result, the nuclear factor of activated T cells is inhibited, leading to decreased production of several principal proinflammatory cytokines such as interleukin (IL)-2, IL-4, tumor necrosis factor-α and interferon-γ. Sandimmune (Novartis Pharmaceuticals) was found to have both poor and highly variable oral bioavailability in human studies,48,49 and is not routinely used in dogs or cats. The microemulsion or modified CsA formulation (Atopica; Novartis Animal Health) enhances the oral absorption of this otherwise poorly soluble drug and is approved by the FDA for the treatment of allergic dermatitis in cats. An oral solution (Atopica for Cats; Novartis Animal Health), reported to be well tolerated in cats, is available.
In cats, microemulsified CsA is rapidly absorbed after oral administration, with bioavailability between 25% and 29% and an elimination half-life of approximately 8 h at a dose of 3 mg/kg PO q12h. 50 Transdermal CsA has inconsistent absorption and does not reach therapeutic blood concentrations in most cats. 51 In a small population of cats, ketoconazole given at 10 mg/kg PO with CsA at 4 mg/kg intravenously (IV) increased blood concentrations of CsA approximately two-fold as well as doubling the half-life from 10.7–22.2 h. 52 Clarithromycin also appears to increase the bioavailability of CsA, reducing the dose needed to maintain therapeutic trough levels by 65% and the frequency of administration from q12h to q24h. 53
CsA appears to be a well-tolerated medication. 54 The most common side effects include vomiting, diarrhea, anorexia and weight loss. GI upset following the initiation of oral CsA therapy in some cats is often transient or responsive to dose reduction and may not require drug discontinuation. Anecdotally, we have had a positive response to giving metoclopramide at a dose of 0.3–0.4 mg/kg PO 20–30 mins prior to administration of oral CsA to cats experiencing GI upset. Rare side effects of CsA, including gingival hyperplasia, 55 as well as the development of toxoplasmosis56,57 and possible hemolytic uremic syndrome after renal transplantation, 58 require drug discontinuation. Anaphylaxis associated with intravenous CsA has been reported in one cat. 59 CsA is also suspected to be associated with the development of malignant neoplasia such as lymphoma in cats receiving the medication following renal transplantation, 60 but this has not been definitively proven. 61
The true incidence of opportunistic infections with CsA therapy is unknown. Clinicians should be judicious with the use of CsA and rule out concurrent infections as best as possible prior to initiating therapy, using history, physical examination and available indicated diagnostics (eg, complete blood count, biochemistry panel, urinalysis, feline leukemia virus antigen and feline immunodeficiency virus antibody testing, as well as any additional infectious disease testing as required). Vaccine titers are adequate in CsA-treated cats receiving boosters for feline calicivirus, feline panleukopenia virus, feline herpesvirus-1 (FHV-1), feline leukemia virus and rabies, but not for feline immunodeficiency virus. 62
Reports of CsA use in cats have encompassed a variety of immune-mediated to allergic diseases. CsA has been used effectively in conjunction with glucocorticoids in cats with idiopathic pure red cell aplasia (PRCA) 59 and in a cat with primary immune-mediated thrombocytopenia. 63 The drug appears to be effective when given topically for treatment of proliferative feline eosinophilic keratitis. 64 In a single case report, it improved clinical signs in a cat with chronic progressive polyarthritis. 65 CsA also seems to be effective for the treatment of refractory feline stomatitis, based on a small population of cats that had already undergone premolar–molar or full-mouth extractions, at a dose of 2.5 mg/kg PO q12h, compared with placebo. 66 CsA trough levels >300 ng/ml were associated with significant improvement in that study. Furthermore, CsA given at doses in order to maintain trough levels between 500 and 850 ng/ml prior to antigen challenge in Ascaris suum-sensitized cats (ie, cats with experimentally induced asthma) inhibited airway hyperresponsiveness, airway inflammation and airway remodelling in the acute and chronic (6 weeks) setting. 67 Targeted trough levels for CsA are extrapolated from human medicine, with very few studies equating clinical status to blood concentrations, thus making it difficult to make generalizations and recommendations for monitoring therapy. In one retrospective study, a median trough CsA level of 218 ng/ml (range 96–368) was effective in the treatment of PRCA in cats. 59
CsA is commonly used in veterinary dermatology. In a small retrospective study, CsA and glucocorticoids were shown to be effective but not superior to chlorambucil and glucocorticoids for the treatment of feline pemphigus foliaceus; however, the study’s low statistical power may have contributed to the result of non-superiority. 68 CsA reduced the severity of clinical signs in cats with atopic dermatitis and performed similarly to prednisolone in a randomized double-blinded clinical trial, but this population was small as well. 69 In a large population of cats (n = 100) with atopic dermatitis, CsA at a dose of 7 mg/kg PO q24h appeared to be effective and well tolerated, with more cats improving with regard to their lesions and pruritus compared with CsA at 2.5 mg/kg PO q24h or placebo. 70 Cats induced with CsA at a dosage of 7 mg/kg PO q24h had their dose tapered to q48h after 4 weeks of therapy and then again to twice weekly after another 4 weeks, with over 50% of patients remaining clinically stable. 71
CsA continues to emerge as a promising adjunctive/second-line immunomodulatory agent for a variety of conditions. Most reported uses in our feline patients (with the exception of allergic dermatitis in cats) are limited to case reports or case series with small populations. Larger prospective, placebo-controlled clinical trials are needed in order to determine the extent of this drug’s efficacy as well as for comparison with other immunomodulatory agents. Consequently, glucocorticoids should still be considered the cornerstone of therapy for the treatment of immune-mediated disease in cats. CsA can be considered as adjunctive therapy along with glucocorticoids. It can be considered as sole therapy in patients that cannot tolerate glucocorticoids, such as cats that develop diabetes mellitus secondarily to glucocorticoid-induced insulin resistance.
Pimobendan
Although commonly used in feline medicine, pimobendan (Vetmedin; Boehringer Ingelheim) has yet to be approved for use in cats. It is a calcium sensitizer with both positive inotropic and lusitropic effects. Pimobendan works by inhibiting phosphodiesterase III (PDE III), resulting in decreased breakdown of cyclic adenosine monophosphate. This process increases myocardial contractility through increased release and reuptake of calcium. PDE III inhibition also causes arterial and venous dilation.
The most appropriate dosing regimen for pimobendan in cats has yet to be established. Pimobendan has been used clinically in cats with evidence of ventricular systolic dysfunction, 72 diastolic dysfunction 73 and other cardiac diseases 74 at a dose of approximately 0.25 mg/kg PO q12h and appears to be well tolerated. However, plasma concentrations at this dose are 10-fold higher than those observed in dogs, and the elimination half-life of 1.3 h is almost three times as long. 75 Side effects appear to be uncommon. One cat with systolic anterior motion of the anterior mitral valve leaflet developed severe hypotension in association with pimobendan administration. 72 Other reported adverse effects include anorexia and constipation 74 as well as ptyalism and vomiting. 75
Median survival time (MST) for cats with congestive heart failure (CHF) secondary to all types of cardiomyopathy treated with pimobendan is reported to be between 151 and 167 days.72,74 These reports have no comparator group; therefore, it is difficult to draw conclusions from these studies on whether or not treatment with pimobendan significantly improves survival. However, improved survival has been shown in cats with non-taurine responsive dilated cardiomyopathy treated with pimobendan (MST 49 days) compared with controls (12 days) in a retrospective study. 76 Additionally, in a retrospective review, cats with hypertrophic cardiomyopathy (and a few with hypertrophic obstructive cardiomyopathy) treated with pimobendan after the onset of CHF had a significantly longer survival time (626 days) vs those not treated with pimobendan (103 days). 73 Despite the retrospective nature of the latter studies, pimobendan appears to be a favorable treatment for acute and chronic CHF in cats.
Pimobendan should be beneficial in cats with many different types of cardiomyopathy but theoretically should be avoided in cats with hypertrophic obstructive cardiomyopathy as it may potentially worsen the obstruction. Although one study reports a possible benefit of pimobendan for CHF secondary to hypertrophic obstructive cardiomyopathy, 73 there are too few cats in this population to make any generalizations at this time. Pimobendan in cats remains an extra-label therapeutic, and consultation with a veterinary cardiologist is always recommended.
Clopidogrel
Clopidogrel bisulfate (Plavix; Bristol-Myers Squibb) is a thienopyridine class platelet inhibitor that works by irreversibly inhibiting the adenosine diphosphate receptor P2Y12 on the platelet membrane. It is a prodrug that is metabolized via cytochrome P450-dependent pathways into active metabolites. Clopidogrel inhibits platelet aggregation as well as causing platelet aggregates to disaggregate more easily. 77 In healthy cats, platelet aggregation was inhibited by clopidogrel by day 3 when administered at high doses (75 mg/kg PO q24h) and moderate doses (37.5 mg PO q24h). 78 Cats given a low dose of 18.75 mg PO q24h demonstrated inhibition of platelet aggregation at day 7 (earlier time points were not evaluated in these low-dose cats). Platelet aggregation for all doses was similar to baseline by day 7 after discontinuation of the medication. No adverse effects were appreciated. Based on these results, the dosage of clopidogrel recommended for cats is 18.75 mg/cat PO q24h. Clopidogrel should be discontinued for 7 days prior to any procedure where hemorrhage is an anticipated complication.
The main use of clopidogrel in cats has been for the prevention of arterial thromboembolism (ATE), a devastating condition that affects our feline patients. The most common cause of thromboembolic disease in cats is cardiomyopathy, but conditions in which there is loss of antithrombin such as protein-losing nephropathy and protein-losing enteropathy may also result in hypercoagulability and thromboembolic disease. ATE is associated with a high morbidity and mortality rate and often occurs without prior warning. In a recent retrospective study evaluating 250 cats with ATE that were brought to primary care facilities, 61.2% were euthanized on presentation. 79 Of the remaining cats in which treatment was attempted, 30% died or were euthanized within 24 h and 40% within 7 days. MST for the remaining 30% was 94 days. Overall, 98% of the 250 cats died or were euthanized within 12 months of initial presentation. No factors were identified that predicted survival for ⩾7 days. Although receiving heparin and not receiving aspirin or clopidogrel were reported as independent predictors of mortality within the first week after presentation, these results must be interpreted with caution as there may have been bias towards giving oral medications to those patients thought to have clinically less severe disease.
Clopidogrel unfortunately was not shown to increase the thrombolytic rate of tissue-plasminogen activator in an in vitro study using feline whole blood. 80 As a result, it is not expected to significantly enhance the breakdown of preformed blood clots but, rather, is used to try to prevent new thrombus formation.
Veterinary clinical trials have failed to reveal a clear-cut superior antithrombotic agent for the prevention of ATE. Because of the increased number of platelets associated with arterial clots vs venous clots, platelet inhibitors such as clopidogrel or aspirin theoretically are a good treatment option. Recently, a prospective, double-blinded, multicenter study evaluated the use of clopidogrel (18.75 mg PO q24h) and aspirin (81 mg PO q72h) for the prevention of recurrent cardiogenic ATE and mortality in cats. 81 Treatment with clopidogrel resulted in significantly improved outcomes, with an MST to a recurrent ATE event of 443 days for the clopidogrel group vs 192 days for the aspirin group.
Both aspirin and clopidogrel are reported to be well tolerated in cats. With the recent availability of generic clopidogrel, it has become an even more appealing therapeutic now that the difference in cost is minimal. Additionally, while there is no clear advantage to using both medications concurrently, this treatment regimen can be considered because of their slightly different mechanisms of action.
There is no reliable and readily available method for monitoring feline patients receiving clopidogrel. However, a recent study evaluating the use of Plateletworks, a screening assay used in human medicine to assess platelet aggregation, has shown that it holds some promise as a diagnostic tool to monitor clopidogrel therapy in cats. 82 Clopidogrel appears to be well tolerated in cats. 78 Nevertheless, bleeding remains a potential complication with the use of any anticoagulant. The development of non-regenerative anemia in cats on long-term clopidogrel therapy has also anecdotally been reported. 77
Mirtazapine
Anorexia is a common presenting complaint in our feline patients, and a comprehensive diagnostic evaluation is recommended to identify the underlying cause in each case. In some instances a progressive, irreversible disease such as chronic kidney disease (CKD) is identified. The clinical approach to management of anorexia in cats is to treat the identified underlying disease and provide supportive care, which may include placement of a feeding tube and/or administration of an appetite stimulant. Mirtazapine is a tetracyclic antidepressant causing antagonism at central pre-synaptic α2 receptors, 5HT2, 5HT3, and H1 receptors. Antagonism of 5HT3 receptors likely accounts for the majority of mirtazapine’s antiemetic and anti-nausea effects, while antagonism of α2 receptors contributes to appetite stimulation through an increase in norepinephrine concentration.
Until recently, recommended dosing for cats was extrapolated from humans or based on anecdotal reports. In young healthy cats, doses of 1.88 mg/cat and 3.75 mg/cat were shown to produce similar increases in appetite compared with placebo; however, there was a significant increase in side effects (vocalization and interaction/sociability) with the higher dose compared with the lower dose. 83 The half-life of mirtazapine in the population dosed at 1.88 mg/cat was 9.2 h. In cats with CKD, the half-life was 15 h, with a significant negative correlation found between serum creatinine and clearance of mirtazapine. 84 Drug accumulation is possible with daily dosing in cats with renal disease, but not with q48h dosing. In a placebo-controlled, double-blinded, crossover clinical trial, mirtazapine administered at 1.88 mg PO q48h for 3 weeks significantly increased activity, appetite and weight, and decreased vomiting compared with placebo in cats with CKD. 85 There is also some evidence that metabolism of mirtazapine is decreased in older cats without renal insufficiency, 84 but the need for dose reduction in this population has not been shown yet.
Mirtazapine undergoes hepatic metabolism and renal excretion. Dosing mirtazapine q48h seems to be tolerated well in cats with CKD. 84 There are currently no reports evaluating differences in pharmacokinetics in cats with hepatic dysfunction. In human patients with hepatic dysfunction the half-life of mirtazapine increased by 39%, suggesting dose adjustment is needed in patients with impaired hepatic function. 86 Similarly, it is reasonable to consider dose reduction in feline patients with advanced hepatic dysfunction or markers of hepatic failure.
No reports to date evaluate the efficacy and safety of long-term use of mirtazapine in cats with CKD. However, it is of anecdotal benefit to many cats with CKD, without the development of adverse effects requiring discontinuation of the medication. Risk of development of serotonin syndrome is considered to be low, and cyproheptadine has been considered as an antidote. 87 Consequently, it is not recommended that mirtazapine and cyproheptadine are given concurrently for appetite stimulation, considering their actions may cancel each other out. 88
Famciclovir
FHV-1 is a common cause of upper respiratory tract disease and ophthalmic disease in cats. Famciclovir (Famvir; Novartis Animal Health) is an antiviral that, although not currently licensed for use in cats, is commonly used to treat this infection. In cats, oral famciclovir is absorbed and converted to penciclovir, reaching maximum plasma concentrations in approximately 3 h.89,90 Penciclovir is then converted into penciclovir triphosphate by virus-induced thymidine kinase present in cells infected by α-herpesviruses. It is penciclovir triphosphate that inhibits viral DNA polymerase, thus inhibiting viral DNA synthesis and viral replication. As such, famciclovir is considered virostatic along with all other antivirals currently used for the treatment of FHV-1 infections.
Based on in vitro data, the target plasma concentration or half maximal inhibitory concentration (IC50) of penciclovir against FHV-1 is 3.5 μg/ml. 91 Penciclovir maximum observed plasma concentration (Cmax) and time to Cmax for doses of 40 mg/kg PO and 90 mg/kg PO are similar at around 1.3 μg/ml and 2.8 h. 90 These results suggest that famciclovir metabolism may become saturated at these doses and that efficacy of the lower dose may be similar to that of the higher dose. A prior study evaluated penciclovir pharmacokinetics in cats at a lower dose (15 mg/kg PO) but found the Cmax to be 0.35 μg/ml, a value even further from the target concentration. 89
In a prospective, placebo-controlled clinical trial in cats experimentally infected with FHV-1, cats treated with famciclovir (90 mg/kg PO q8h for 21 days) had lower disease scores, lower conjunctivitis histologic scores, shed less herpetic DNA, and at the end of the study had lower levels of circulating anti-FHV-1 antibodies compared with controls. 92 Famciclovir-treated cats also gained weight throughout the study, whereas control cats lost weight. In a case series famciclovir was reported to be effective and well tolerated in the treatment of clinical signs associated with FHV-1 infections involving the eyes (ie, conjunctivitis, keratitis, corneal sequestra), upper respiratory tract (ie, rhinosinusitis) and skin (ie, dermatitis). 93 All nine adult cats treated with oral famciclovir experienced clinical improvement that was considered superior to their previous reported response to other supportive therapies. The treatment regimens used for famciclovir varied between cats and included 62.5 mg/cat PO q24h for 7 days, then q48h for 10 days; 62.5 mg/cat PO q12h for 21–30 days; 62.5 mg/cat PO q24h for 7 days, then q12h for 7–43 days; 62.5 mg/cat PO q24h for 120 days; and 125 mg/cat PO q8h for 14–42 days. 93
Reported adverse effects of famciclovir are limited to those from small studies or described in anecdotal observations. Famciclovir has been used successfully in kittens and queens for the treatment of FHV-1 in the shelter setting. 93 However, safety studies evaluating the administration of famciclovir to pregnant queens have not been conducted. Famciclovir appears to be well tolerated in adult cats. Reported side effects include a decrease in packed cell volume and total protein as well as an increase in white blood cell count due to an increase in neutrophils and monocytes. 89 These changes may, however, be due to multiple blood draws and stress. Another study showed no changes in lab work (complete blood count, biochemical panel, urinalysis) suggestive of drug toxicosis. 92
Famciclovir appears to be a viable option for both kittens and adult cats in the treatment of many of the manifestations of FHV-1 infections including keratitis, conjunctivitis, rhinosinusitis and dermatitis. Its use in kittens is advised to be limited to those with severe or persistent disease. 94 A dosage recommendation of 40–90 mg/kg PO q8h is reported to be well tolerated; 95 however, the most appropriate treatment regimen for famciclovir has yet to be determined.
Oclacitinib
Oclacitinib (Apoquel; Pfizer) is approved in the United States and Europe for the treatment of pruritis and inflammation associated with atopic dermatitis in dogs. It is a novel Janus kinase (JAK) inhibitor that has activity against JAK1-dependent cytokines. JAK enzymes are important in cytokine signaling, particularly those involved in pro-inflammatory, pro-allergic and pruritogenic conditions. As such, it has shown promise as a safe and effective treatment for atopic dermatitis in dogs. 96
Although no published studies are available reporting the pharmacokinetics or clinical use of JAK inhibitors in cats, an abstract described the use of a JAK inhibitor as a novel treatment for feline asthma. In an experimental model of asthma in 24 cats, a novel JAK inhibitor administered at a dose of 0.5 mg/kg or 1 mg/kg PO q12h for 28 days significantly reduced eosinophilic airway inflammation compared with placebo (unpublished data presented at the American College of Veterinary Internal Medicine Forum 2013, Seattle, WA). There was no significant difference in the reduction of inflammation between the two doses, and there was no significant difference between the study drug and placebo with regards to ventilator-acquired pulmonary mechanics with methacholine challenge. No adverse effects or clinically relevant laboratory abnormalities were observed.
In a group of 21 cats with IL-31 induced pruritis, oclacitinib administered at 0.4 mg/kg and 1 mg/kg PO 1 h prior to IL-31 injection significantly reduced pruritis by 63% and 62%, respectively. However, oclacitinib administered at a dose of 0.4 mg/kg PO 12 h prior to IL-31 injection failed to reduce pruritis (unpublished data presented at the American Academy of Veterinary Pharmacology and Therapeutics Biennial Symposium 2013, Potomac, MD).
JAK inhibitors may prove to be a beneficial adjunctive therapy with glucocorticoids or a potential alternative to glucocorticoids for the treatment of feline asthma. There may also be a potential role for oclacitinib in the treatment of feline allergic dermatitis. Prospective studies in cats with naturally occurring disease are needed before this medication can be recommended for clinical use.
Summary
Clinical indications, adverse effects and dosing recommendations for the 10 medications discussed in this review are summarized in Tables 2 and 3.
Ten novel pharmaceuticals: summary of the clinical indications and reported adverse effects in cats

Approved uses in the United States and in Europe are denoted by USA and EU, respectively; IV = intravenous; Gl = gastrointestinal; CKD = chronic kidney disease
Ten novel pharmaceuticals: reported doses in cats based on pharmacokinetic/pharmacodynamic studies and clinical use

USA and EU denote labeled dose in the United States and in Europe, respectively; PO = orally; SC = subcutaneously; IV = intravenously; CKD = chronic kidney disease
Key Points
Veterinary medicine continues to be a dynamic field requiring clinicians to constantly modify their clinical practice.
The pharmaceuticals discussed in this review article are only a select few out of many with new information pertaining to their clinical use.
It is likely that knowledge of even these medications will continue to expand over the next several years.
Feline practitioners are strongly encouraged to familiarize themselves with any novel therapeutic and to seek evidence-based guidance whenever possible.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors have no conflict of interest to declare.