
Abstract
Practical relevance:
Oral examination in the cat is a process of observing both normal and abnormal, and should be an integral part of any wellness examination as well as a response to any specific complaint(s). The basis for an accurate diagnosis is meticulous attention to detail. It is essential that the clinician performs a whole body examination prior to examining the head and neck region.
Stages of examination:
A thorough oral examination involves four stages. The first stage is to review the current oral problem(s) by asking questions and listening carefully to the owner’s responses; gaining a thorough medical/dental history may shed more light on the current problem(s). The second stage is an extraoral physical examination to visualise and palpate the head and neck regions in the awake patient. In the third stage the clinician performs an intraoral examination in the awake patient, before proceeding to the final stage, which is an extraoral and intraoral examination under general anaesthesia.
Aim:
This article describes a systematic approach to the oral examination, based on these four stages. The aim of this process is not only to facilitate the making and recording of observations, but also to help avoid missing important clues that may aid in reaching a diagnosis. Common tooth pathologies in the feline patient are also briefly reviewed, paving the way for accompanying articles in this two-part Special Issue, which will provide further insight into these pathologies and discuss management approaches.
Review of current oral problem(s)
The first part of the process of oral examination is concerned with gathering general information relating to the specific problem and its relationship to any previous or current ongoing condition. This requires the immediate involvement of the owner and gives clues that will assist when carrying out the direct oral examination. Suggested questions for eliciting relevant dental and medical history are listed in the box.
At this stage information related to the onset and duration of clinical signs can be obtained. one of the most common clinical signs in the cat is in appetence or anorexia – and while this can be associated with many systemic diseases, it may have a dental or oral cause.
Many oral conditions have associated clinical signs. Periodontal disease and tooth resorptions are seen most frequently, followed by oral/mucosal ulcerations, tooth fractures with or without pulp exposure, gingival recession, and inflammation of the gingiva/mucosa and oropharynx. oral pain may additionally produce signs such as head shaking, pawing at the mouth, tongue thrusting, hypersalivation or rubbing the head along the ground.

Another commonly reported sign of oral disease in cats is halitosis. Periodontal disease is a main contributor due to plaque accumulation and the resultant production by anaerobic bacteria of volatile sulphur compounds (see later), but there are various other possible causes that should be considered (see below).

Chronic drooling or ptyalism is commonly due to either oral irritation or a lack of swallowing, rather than an absolute increase in saliva production, and may be seen in cats with oral infection, oral neoplasia, pulp exposure, jaw fractures, severe inflammatory disease of the oropharynx, foreign bodies, upper respiratory tract disease and toxicity.
Uneven jaw movement on opening and closing the mandible may be due to jaw, head or dental fractures, malocclusions or temporomandibular joint dislocations. Cats that are observed to be hesitant in eating, unable to prehend, masticate or swallow food, not grooming with poor coat condition or losing weight should be examined for any signs of oral/dental disease. Sometimes neurological disorders including cranial nerve dysfunction can affect mastication and swallowing. Tongue thrusting, jaw chattering, excessive chewing, or preferential chewing on one side of the mouth may indicate pain associated with jaw or dental fractures, inflammation, tooth resorptions or a periodontal or endodontic disease. Sometimes, plaque and calculus accumulation on one side of the mouth is indicative of disease on that side of the mouth. Any abnormal findings will warrant further investigation. In cats, common diseases that manifest with many of these signs are tooth resorption and generalised gingivostomatitis. Facial swelling may be due to periodontal or endodontic disease, neoplasia, foreign bodies, trauma, stings, bites, allergies or salivary diseases.

Medical/dental history
The collection of a comprehensive history prior to direct oral examination is salient in the process of reaching an accurate diagnosis as, unlike other disciplines where patients may present with signs obvious to the owner (eg, alopecia and pruritus with flea allergy dermatitis, a surgical lameness or vomiting and diarrhoea), in dentistry often the disease is insidious and hidden inside the oral cavity (eg, a fractured tooth, oral neoplasia or periodontal disease).
The history should include the patient’s signalment, in particular breed, sex and age; a full clinical history, including past and present vaccination status; dietary history; and previous and any currently prescribed medications. The owner should also be asked about the number of cats in the household; where the cat was acquired from; any access to catteries or infectious disease; if the cat is confined to indoors or roams outside the house; the level of previous professional care and any past dental procedures; and the past and current dental homecare programme.
Age (see Table 1) is an important factor as disease relating to malocclusions, teething and juvenile infections such as respiratory disease, eruption gingivitis or periodontitis may be observed in young kittens. Breed can be a factor when considering early tooth resorptions and/or gingivitis, which are often seen in Burmese and orientals. The Burmese breed appears also to be overrepresented for feline orofacial pain syndrome. Early malocclusions and tooth crowding can be found in some lines of Persians and other brachycephalic breeds. Cats from breeding catteries as well as rescue facilities or multi-cat house- holds may have been exposed to feline respiratory disease or feline leukaemia virus (FeLV). Cats with outdoor access may have been exposed to feline immunodeficiency virus (FiV). Records of previous dental programmes will give information on any abnormal findings or missing teeth, while the owner’s current homecare protocol will aid in determining the complexity of any planned treatment and future homecare compliance.
Oral conditions most commonly seen in the cat by age

FCV = feline calicivirus, FHV = feline herpesvirus, FeLV = feline leukaemia virus, FIV = feline immunodeficiency virus
Owners can be directed to the Veterinary oral Health Council website (www.vohc.org) for a list of approved dental diets and other oral health aids.

General and extraoral physical examination
The second part of the oral examination of the cat – a general physical and extraoral assessment – is conducted prior to checking the mouth itself.
– Suborbital and ventral mandibular swellings or draining fistulas may be due to periapical infection (apical periodontitis) involving the maxillary canines (104/204) or fourth premolar teeth (108/208), or the mandibular canine teeth (304/404), respectively.
– Heart murmurs, liver disease or kidney infections can be associated with advanced periodontal disease.2–6
– Joint swelling or inflammation and arthritis may be worsened with periodontal disease.3,4

Major salivary glands in the cat: 1 = parotid, 2 = mandibular, 3 = sublingual, 4 = zygomatic. Of these glands, only the mandibular glands are palpable in the cat. The other glands are either too diffuse to palpate easily (parotid and sublingual) or too deep to palpate (zygomatic)

Open-mouth view in an anaesthetised cat demonstrating the membranous molar pad (circled) containing the molar gland, lingual to the molar tooth

Intraoral examination (conscious)
The third part of the oral examination involves visualisation of the oral cavity and internal structures while the patient is awake. Generally, this is performed in the examination room.
An examination of the conscious cat may not always be possible, depending on the cat’s temperament or degree of oral pain. it is helpful for an assistant gently to restrain the cat to allow the clinician to perform the intraoral examination. However, if the cat is strongly resisting it may be necessary to move on to the oral examination under general anaesthesia.
Initial inspection of teeth
Initially with the mouth closed and teeth together, lift the upper lips and observe for the following:
– do the incisors line up? Check that the incisal edges of the lower incisors rest on the cingulum of the upper incisor teeth and that there is no midline deviation on a front (rostral) view.
– Canine occlusion – is the mandibular canine (304/404) sitting equidistant in the space between the maxillary third incisor (103/203) and canine tooth (104/204)?
– Premolar/molar relationship – the maxillary premolar/molar teeth should be lateral (buccal) to the mandibular premolar/molar teeth.
– Carnassial relationship – is there any traumatic occlusion and gingival irritation?
– When counting the teeth observe for extra (supernumerary) teeth, persistent deciduous teeth and missing teeth.

Front (rostral) view showing normal incisor and canine occlusion

Lateral view of the incisors (103/403), canines (104/404), maxillary premolars (106/107/108) and mandibular premolars (407/408)
Inspection of intraoral structures
Inspection of the intraoral hard and soft tissue structures should follow, focusing on the dentition, lips, gingiva, mucosa, tongue, hard and soft palate, incisive papilla, hard palate rugae, tonsils, palatine arches, fauces (lateral walls of the oropharynx, located medial to the palatoglossal folds) and sublingual tissues (Figure 5).

Open-mouth views. (a) Observing the dorsum of the tongue, the dentition, the oropharynx, the hard and soft palate, and the incisive papilla mid- palatal to incisors 101/201. (b) Observing the tongue (with its large filiform papillae), hard and soft palate, oropharyngeal area and palatoglossal folds

Heavy calculus deposits on the maxillary third and fourth premolars (107/108)
On visual inspection, a cat with periodontal disease (Figure 7) may show evidence of gingival swelling, redness and altered gingival contour around the teeth. There may also be areas with gingival recession, furcation exposures (in multi-rooted teeth) or purulent discharge from periodontal pockets. Variable amounts of plaque and calculus may be present. Any inflammation/ulceration that appears to be localised to one area of the mouth should not immediately be classified as periodontal disease but viewed with suspicion and warrants further detailed investigation. As a general rule, any soft/hard tissue lesion found in the oral cavity (Figure 8), especially where no known cause can be found, should be biopsied to rule out neoplasia or immune-mediated disease.

Periodontal disease. Note the accumulation of calculus on teeth 404, 407, 408 and 409, the mild gingivitis associated with tooth 404 and the advanced severe inflammation (gingivitis and hyperaemia) of the gingiva associated with teeth 407, 408 and 409

Oral mass adjacent to the mandibular molar tooth (309)
Extraoral and intraoral examination (under anaesthesia)
The fourth part of the oral examination is to evaluate the extraoral structures and oral cavity under general anaesthesia and record observations on a dental chart (see page 879). Essentially, a similar examination to that performed in the awake patient is repeated in the anaesthetised patient (see box below), although in much greater detail. often disease can be more readily observed once the cat has been anaesthetised.
A preoperative assessment of systemic health and level of anaesthetic risk is essential prior to this stage of the examination. it is prudent, especially in the senior cohort, to include preoperative blood work (haematology and biochemistry, T4 levels) and urine analysis. Perioperative intravenous fluid therapy, patient monitoring including core temperature, and gaseous anaesthesia with airway protection using a cuffed endotracheal tube should be a minimum standard when performing this intraoral examination.


Examination of the dorsal surface of the tongue in an anaesthetised cat

With the cat under anaesthesia, a more detailed examination of abnormalities observed in the awake patient can be made. (a) Rostrally deviated maxillary canine (204) (malocclusion/ mesioversion). (b.)Supernumerary maxillary canine tooth. (c) Gingival enlargement overlying areas of tooth resorption at the cervical region of the maxillary third and fourth premolar teeth (107/108)
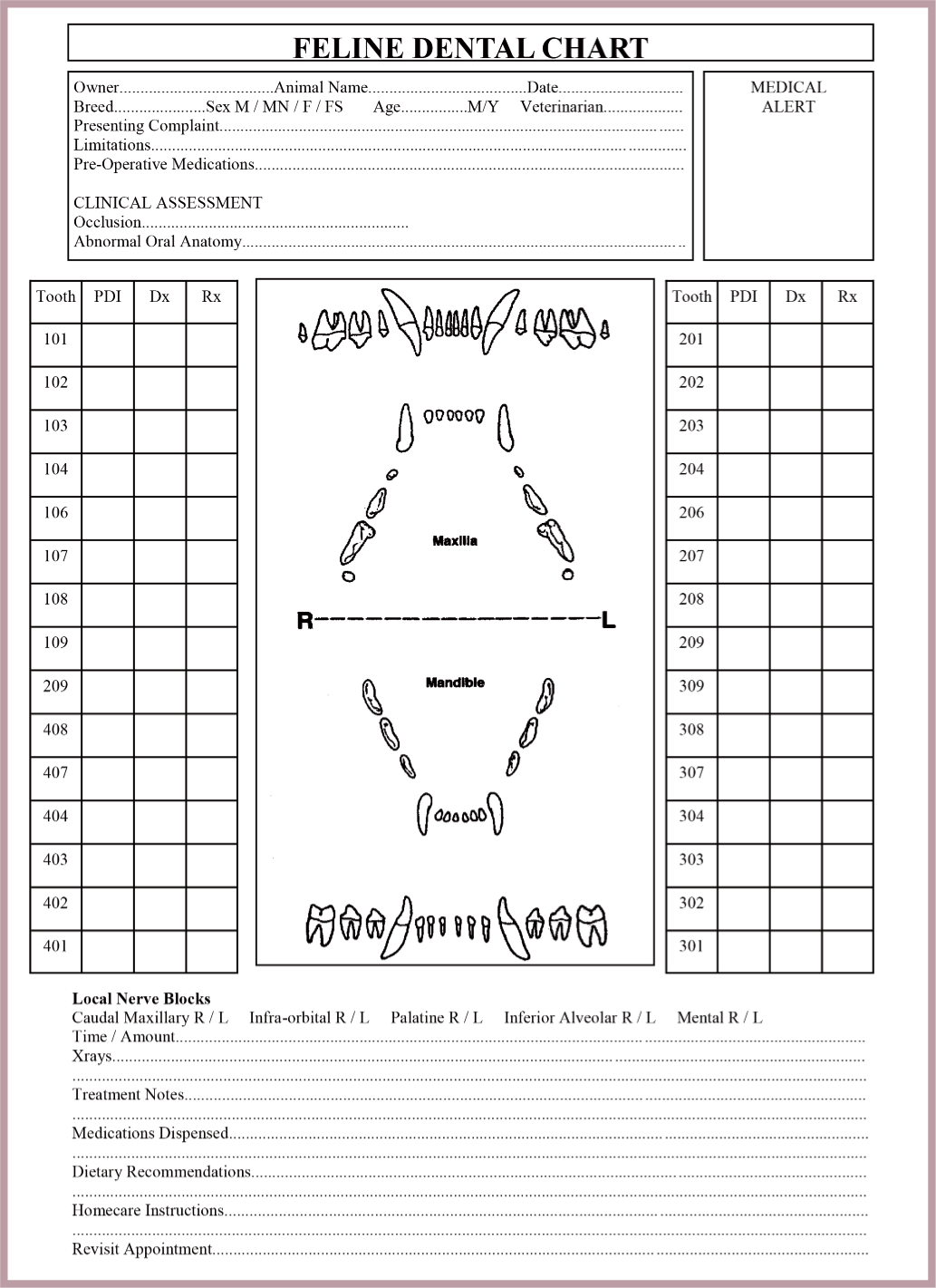
Feline dental chart, available as Supplementary material accompanying this article at jfms.com

Individual tooth examination is performed after the whole mouth has been evaluated. Initially the space that the tooth occupies is observed to confirm the presence or absence of an adult or deciduous tooth. The important observations pertaining to each tooth include: plaque accumulation, calculus accumulation, gingival index and gingival inflammation, gingival sulcus or periodontal pocket depth (see box below), and any pathology of the tooth crown and root. Observations are recorded on the dental chart.
When a deciduous tooth and the permanent adult tooth are present at the same time, the deciduous tooth is termed persistent and requires extraction. If no tooth is present, then the history should inform the clinician as to whether the tooth has been previously extracted; if not, the area should be radiographed to confirm the tooth’s absence or whether it is retained subgingivally.

Diagram of a single-rooted tooth


Formation of a periodontal pocket. Note the plaque and calculus accumulation on the tooth root and loss of attachment including periodontal ligament and alveolar bone

Determination of gingival sulcus or periodontal pocket depth
Periodontal probes are tactile instruments used to determine the position of the epithelial attachment and thereby measure the depth of the gingival sulcus or periodontal pocket. They are typically a metal or plastic tapered rod with a blunt end and graduated in millimetre markings (see box on page 882).

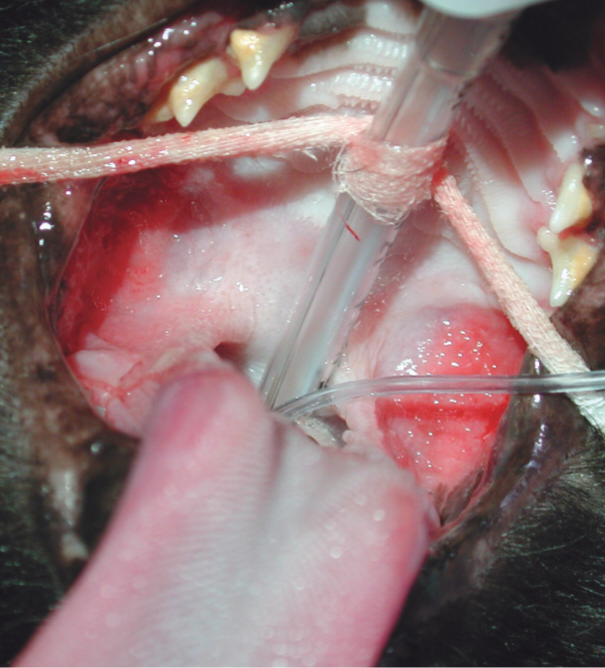
To determine sulcus or pocket depth, the periodontal probe is placed parallel to the root surface, under the free gingival margin (Figures 14 and 15), until it meets resistance from the epithelial attachment. Gentle force should be used, as it is easy to penetrate through inflamed tissues. The depth of the sulcus is measured in millimetres from the gingival margin to the epithelial attachment. Measurements are made in two or three places on the buccal surface and two or three places on the lingual/palatal surface of each tooth. if the gingiva has receded, then the measurement from the epithelial attachment to the cemento-enamel junction gives the loss of attachment. The depth of the pocket, as well as the extent of gingival recession, should be recorded on the dental chart.

Diagram of periodontal probing

(a) Holding and using a periodontal probe; note the tip of the probe is at the gingival margin. To measure the periodontal sulcus/pocket, the probe is advanced subgingivally to the epithelial attachment. (b) Placement of a periodontal probe into the periodontal pocket on the mesiopalatal surface of the maxillary canine tooth (204)

Williams periodontal probe (a and b) and explorer probe (a and c)

Nabers probe (without graduations)

Healthy periodontal tissues exhibit sulcus depths of 0–0.5 mm. Thus, measurements of greater than 0.5 mm indicate attachment loss and the presence of a periodontal pocket.
Assessment of gingivitis
During the process of probing, haemorrhage may occur. This is termed ‘bleeding on probing’ (BoP) and its presence or absence, together with any spontaneous bleeding, gives the clinician a guide as to the degree or severity of gingivitis (Figure 18). This contributes to the gingival index,12,13 which can be recorded on the dental chart.

Gingival inflammation/hyperplasia of the maxillary premolar and molar teeth (204/207/208) and marked gingivitis and ulceration involving the mandibular premolar and molar teeth (307/308/309)

Other gingival observations or pathology that should be recorded are:
Any purulent or bloody discharge.
Hyperaemia, hyperplasia or ulceration.
Exposure of areas between multi-rooted teeth (furcation); this is assessed using a periodontal probe or Nabers probe placed perpendicularly to the long axis of the tooth into the furcation area (see later).
Loss of tissue and exposure of alveolar bone and tooth root cementum.
Plaque and calculus scoring
Plaque and calculus may also be indexed and recorded on the dental chart.
Plaque, a biofilm of salivary glycoproteins, bacteria and saliva, takes about a week to form a mature colony. Plaque is not a food residue, as it actually forms more rapidly during sleep and less rapidly when food is consumed. Plaque cannot be seen unless it is stained. Either erythrosine (a red food dye) or fluoresein in combination with a long-wave ultraviolet light source (see box, right) may be used. one stage dyes stain all plaque the same colour. Two stage dyes stain new and mature older plaque different colours – red and blue, respectively. Although sold on the human market (eg, PlaqSearch Liquid disclosing Solution drops; TePe) they can safely be used in cats.
Plaque scoring is performed in research studies and may also be used as a guide to the effectiveness of an owner’s homecare protocol. it is additionally useful for comparing diets that claim plaque-reducing effects. Many authors have put their personal stamp on plaque scoring, with the most accepted method in veterinary dentistry being the Logan and Boyce modification of the Turesky plaque index that is used for human teeth. This simple method uses a disclosing solution that is placed gently onto the crown surface and immediately rinsed with water. A numerical value is assigned based on the degree of coverage and thickness on the tooth surface:

Once plaque scoring is completed, plaque can be gently brushed off with a toothbrush and the calculus accumulation given a score. As calculus deposits can be grossly observed, no disclosing agents are required. The Warrick Gorrel method is used, which likewise simply assigns a number to the surface area covered in calculus:


Assessment of furcation exposure
Periodontal disease, as discussed earlier, results in loss of the periodontal attachment apparatus (gingiva, periodontal ligament or alveolar bone), producing a periodontal pocket. it may also cause loss of the periodontal ligament and alveolar bone. When bone is lost around the roots of a multi-rooted tooth, the resulting furcation exposure can be assessed. A Nabers probe or explorer probe is used and the degree of furcation exposure (see left) assigned to the tooth is recorded on the dental chart.

Tooth mobility
Tooth mobility is also directly associated with the loss of supporting structures, including bone and periodontal ligament. Likewise, a number can be assigned to, and recorded for, each tooth (see right).

Assessment of individual tooth pathology
Once the above assessments have been made, the teeth are individually evaluated for endodontic or traumatic disease (eg, fractures, enamel hypoplasia, tooth resorption). Using a dental explorer, the clinician uses tactile feel to identify any loss of tooth structure both supra- and subgingivally. The explorer or other fine- tipped instruments can also be used to locate supracrestal tooth resorption, subgingival calculus deposits and pulp exposures. Similarly, they can be used after scaling and polishing to assess the presence of residual subgingival calculus. A dental mirror can be used to view areas of the mouth that are not normally easily accessible such as the palatal and lingual surfaces of the teeth (Figure 19).

Use of a dental mirror to assess areas that are otherwise difficult to examine
Commonly observed tooth pathology
Tooth fracture, abrasion or attrition
Tooth fractures, due to trauma from fighting, road traffic accidents, bone chewing or falls, are frequently observed. The fracture may involve enamel only, enamel and dentine, or may extend into the pulp chamber (Figure 20). Worn teeth may also be observed, with pathology classified as abrasion or attrition. Abrasion of the enamel/dentine is due to wear from an external source, whereas attrition is caused by tooth-to- tooth contact.

Complicated crown fractures of canine teeth 204, 304 and 404
If the fracture or area of abrasion/ attrition is confined to the enamel or dentine then restoration and smoothing of any sharp edges is required. if it extends into the pulp chamber, the pulp may appear pink if the injury is recent; if chronic, the pulp may be necrotic (grey/black dis-colouration in centre of tooth). once the pulp has become necrotic, there is no pain on probing the exposure. if fractures are recent, the teeth are often painful and the cat may be inappetent and resist oral examination when awake. Although not often seen in cats, chronic abrasion due, for example, to dermatitis results in the production of tertiary or sclerotic dentine so that the tooth pulp continues to be protected by a dentinal layer. Pulp exposure requires treatment by extraction or root canal therapy to extirpate any infected pulp tissue and prevent subsequent osteomyelitis and periapical infection.
A tooth that has suffered trauma without fracture may develop pulpitis and eventual pulpal necrosis. Some of these teeth will appear darkened through the enamel and require root canal treatment to prevent periapical pathology. A tooth that is not treated once fractured may result in a draining sinus adjacent to the medial canthus of the eye or lateral bridge of the nose (maxillary canine 104/204 or premolar 108/208) or ventral surface of the mandible (mandibular canine 304/404).
No endodontic examination is complete without dental radiographs to confirm pulp exposure and to assess the degree of periapical pathology prior to treatment. Teeth with advanced periapical lesions may benefit from extraction over root canal treatment.
Tooth resorption
Resorptions of feline teeth occur commonly in Burmese and Siamese cats under 12 months of age and in a number of other breeds over 6 years of age.15 External resorption is more common in the cat than internal resorption and results in loss of the enamel and root structure of the tooth. The lesions are very painful and easily detected using an explorer probe. When the dentine or pulp is contacted, often the jaw will ‘chatter’. While the aetiology remains uncertain, studies have suggested that many cats have subgingival resorptions that are only detected by radiography;15–17 thus relying on clinical signs alone is often insufficient.
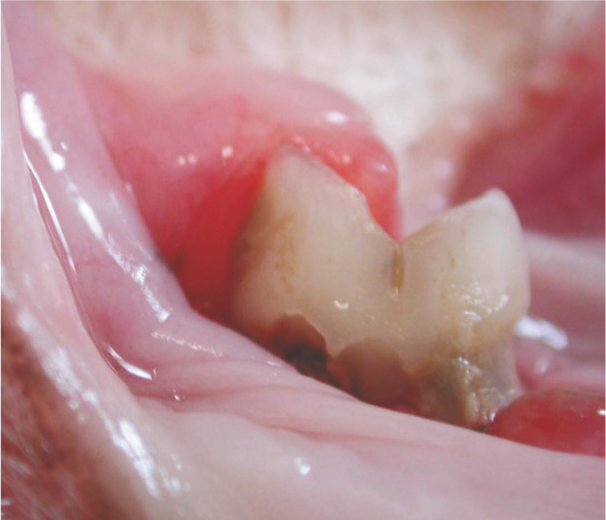
Typically, resorptive lesions are found beneath haemorrhagic, hyperplastic gingiva adjacent to a surface enamel defect that is often covered in calculus (Figures 21 and 22). The finding of one tooth resorption will raise the level of suspicion that other teeth are affected. in advanced cases the resorption may result in complete loss of the crown and the tooth may appear clinically to be absent, although the roots are still present subgingivally. Treatment requires whole dentition radiography to confidently classify the variants of the resorption lesions and to define if an absent tooth has retained roots. Radio- graphic evaluation assesses the integrity of the root and surrounding tissues, in particular the periodontal ligament and periapical area.

Tooth resorptions associated with teeth 407 and 408. Note the inflammation of the gingiva surrounding these teeth
Inflamed molar salivary gland adjacent to tooth 409, due to tooth resorption
Resorptions have been classified as type 1 lesions, which may present with a complete and radiographically visible periodontal ligament; type 2 lesions, where the root is being resorbed, and which show characteristic ankylosis (replacement resorption) of the root to the surrounding alveolar bone so radiographically appear to have lost the periodontal ligament (Figure 23); and type 3 lesions, which are a combination of type 1 and 2 lesions in multi-rooted teeth. Tooth resorptions may also be staged according to hard dental tissue destruction and pulp involvement. Classification/staging is important for decision-making prior to extracting the tooth root.
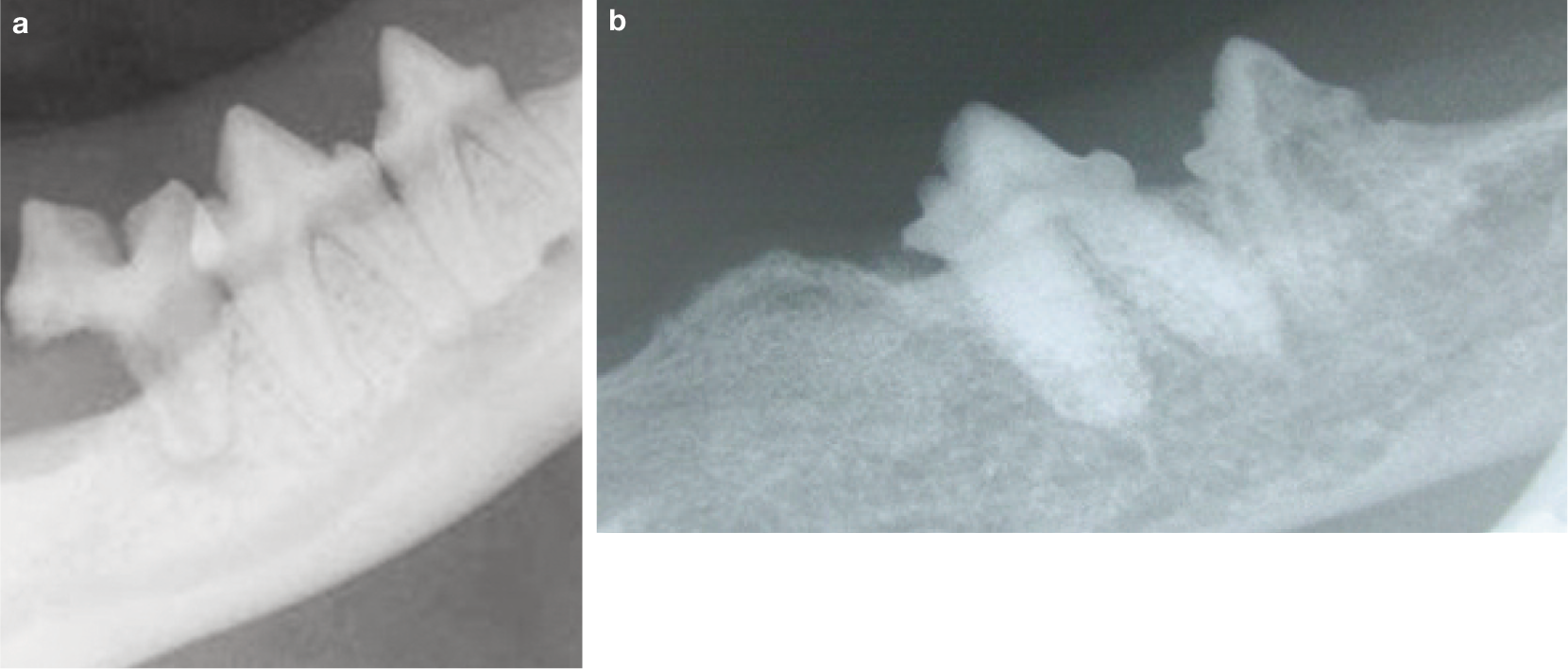
(a) Radiograph of type 1 tooth resorption; note loss of distal root of the mandibular molar tooth 409. (b) Radiograph of type 2 tooth resorption, revealing complete loss of mandibular molar tooth 409 and incomplete loss of premolar tooth 407
Ulceration and inflammation
Ulceration and inflammation is a frequent finding in many feline patients. individual areas of ulceration or inflammation should be looked on suspiciously for neoplasia or eosinophilic granuloma complex, trauma, or caustic chemical or electrical burns.
Eosinophilic granuloma complex is a common disease affecting young to middle-aged cats that consists of three entities: eosinophilic granuloma, eosinophilic ulcer and eosinophilic plaque.18 The disease has been associated with concurrent insect bites (fleas and mosquitoes), food allergy, atopy and chronic feline calicivirus (FCV) infection. The lesions may occur on the hard palate, soft palate or tongue and comprise raised red plaques with yellowish accumulates (Figure 24). A peripheral blood eosinophilia is sometimes found. Ulcers are often located on the upper lip, termed a ‘rodent ulcer’, but may also be caused by trauma from the mandibular canine teeth (304/404) with resultant secondary infection.

Eosinophilic granuloma buccal to tooth 409
Generalised oral inflammation may be due to bacterial (eg, Porphyromonas species and spirochete) infections,19,20 viruses (including feline herpesvirus [FHV], FCV, FeLV and FiV; Figure 25), allergic diseases and systemic diseases such as diabetes mellitus or renal disease, but often gingivostomatitis is of an idiopathic nature. Biopsy of all oral inflammatory disease should be recommended as it is not possible to make a diagnosis on clinical presentation alone. Eosinophilic granuloma may present as a gingivostomatitis. Squamous carcinoma, the most common oral neoplasm in the cat, may occur sublingually (Figure 26) or gingivally.
Inflammation lateral to the palatoglossal folds in an FIV-positive male cat

Sublingual squamous cell carcinoma
Key Points
Feline oral disease often has an insidious onset, with cats showing few or no oral signs at all. Cats may, however, seem more lethargic. Owners typically might complain of their cat ‘not being their normal self’, and may simply perceive this as being part of the normal ageing process.
Vigilant owners may recognise a change in eating behaviour (spitting food out, preferentially chewing on one side of the mouth, constant chewing, difficulty swallowing). In some cases, persistent drooling, increased pawing at one side of the face unrelated to grooming or repeatedly rubbing the same side of the face along the ground may be observed.
Any of the above signs can point to the presence of severe oral pathology and warrant oral examination.
A comprehensive oral examination in the cat involves systematic gathering of information, and a dental and medical history, prior to a thorough whole body and oral examination in the conscious patient and then a complete examination of the anaesthetised patient.
Two indispensible diagnostic tools for identifying oral pathology are the periodontal probe and intraoral radiographs.
All findings should be recorded on a dental chart.
A decision will need to be made as to whether treatment is performed under the one anaesthetic episode in consultation with the owner, or whether the cat is woken up and the owner is appraised of the clinical findings, costs and prognosis associated with any future treatments, which can then be scheduled.
Supplemental Material
Click here for Supplementary PDF
Measuring gingival sulcus depth using a periodontal probe
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.