
Abstract
The objective was to review surgical techniques and postoperative complications of surgical correction for patellar luxation (PL) in cats. A retrospective study evaluating 85 surgeries in 71 cats was performed. The records from four referral centres were searched for cats with surgical management of PL. Signalment, history, PL grade and direction, corrective surgical techniques and outcome were retrieved. Binary logistic regression analysis was used to interrogate relationships between case features, surgical correction methods and outcomes. The outcomes were classified as minor and major complications (requiring revision surgery), including continued PL (reluxation). Postoperative complications occurred in 26% of cases; 20% had major complications, including 5% patellar reluxation, and 6% had minor complications. Cats with previous ipsilateral femoral fracture were significantly more likely to suffer complications, including minor (P = 0.02, odds ratio = 12.67), major (P = 0.03, OR = 7.2) and patellar reluxation (P = 0.01, OR = 19.25). Minor complications were significantly more likely with grade 4 PL (P = 0.03, OR = 8.5). Major complications were significantly more likely with tibial tuberosity transposition (TTT; P = 0.03, OR = 5.57). Patellar reluxation was significantly more likely if stifle surgery had been performed previously (P = 0.05, OR = 8.00). The presence of bilateral PL, hip dysplasia, grade 1, 2 or 3 PL, corrective surgery using an anti-rotational suture or femoral sulcoplasty did not influence complications. Complications were more likely for grade 4 PL, previous ipsilateral femoral fracture, if TTT was performed and for cases with previous stifle surgery. This information allows consideration of risks and complicating factors.
Introduction
Patellar luxation (PL) in cats has been infrequently reported in the literature when compared with canine PL studies.1–9 A prevalence study of 78 cats investigating the association of PL and hip luxation found PL in 58% (45 cats); of those, 78% had a grade 1 luxation based on the Putnam grading system,1,10 and only 11 had pelvic limb lameness due to PL. Medial patellar subluxation was reported in 31/33 cats (94%) with otherwise normal stifle joints and no lameness. 1 Patellar subluxation is a common finding in the normal cat stifle and is distinct from grade 1 PL;1,9 cats with low-grade PL or subluxation may not exhibit clinical signs. There is conflicting evidence in the literature as to whether PL is developmental or traumatic in cats. There has been a weak association between hip dysplasia and PL in cats. It has also been reported that Abyssinian and Devon Rex breeds are more prone to PL.1,2,7
Surgical techniques available for the correction of PL in dogs include femoral trochlear sulcoplasty, tibial tuberosity transposition (TTT), soft tissue imbrication and/or release, and femoral corrective osteotomies.11–13 Combinations of these techniques are performed on a single stifle to achieve stable patellar tracking. The same techniques are used for correction of PL in cats, and surgical correction of grade 2 and higher PL in cats can result in excellent clinical outcomes.6,9 In the study by Loughin et al, 9 grade 1 PLs were not managed surgically. However, there is nothing published to indicate whether these techniques should be applied differently in cats, or whether the outcome is different. The purpose of this study was to review the outcome of surgical correction of PL in cats, and to report the outcome in terms of complications and recurrence of PL, as previously reported in dogs. 12
Materials and methods
Medical records from January 2000 to April 2011 from four referral institutions (X1, X2, X3 and X4, redacted) were searched for cases of PL in feline patients. Cats were included if they presented for pelvic limb lameness attributable to PL and had had surgical correction for PL. Sex, age, breed, pelvic limb lameness, direction and grade of PL, concurrent orthopaedic disease, history of previous pelvic limb surgery, type of corrective surgery for PL, outcome and details of further stifle surgery were retrieved and compiled. Cats were excluded if they did not have surgical management or had incomplete records. Grade of PL, as described by Putnam, 10 was either taken as documented numerically if graded out of 4 in the records, or a grade from 0 to 4 was assigned by interpreting the written clinical description. Individual components of surgeries such as TTT and sulcoplasty technique were subjected to separate analysis. Outcomes and postoperative complications were classified as minor, major and patellar reluxation. A major complication was defined as a complication that required revision surgery, including implant removal. Minor complications were defined as those that did not require further surgical management. The complication of recurrent PL (reluxation) necessitating revision surgery was interrogated separately as a subset of major complications.
Statistical analysis
Binary logistic regression analysis was used to determine which factors influenced outcome. Univariate analysis was performed; risk factors identified with a P value <0.2 subsequently had multivariable logistic regression analysis preformed. All analyses were performed on standard software (SPSS version 19; IBM); statistical significance was set at P <0.05.
Results
Data from PL corrective surgery on 85 stifles in 71 cats were retrieved and analysed. Fifty-nine cats had unilateral PL surgery, 12 cats had bilateral PL surgery, and two stifles had two operations to correct patellar reluxation. Fifty-five percent of cats were male neutered, 1.4% were male entire, 42.0% were female neutered and 1.4% were female entire. Forty-three cats were domestic shorthairs, 10 were Bengals and four were domestic longhairs. There were three Maine Coons, three British shorthairs, two Abyssinians and one each of British Blue, Birman, Exotic shorthair, Persian, Rex and Siamese. Mean age was 37 months (range 5–138 months).
Medial PL was present in 80 stifles (94%) and lateral PL in five (6%). Surgery was performed on 46 left stifles (54%) and 39 right stifles (46%). Hip dysplasia was present in 15 cats (17 stifles); six cats had previous ipsilateral femoral fracture; five cats had concurrent stifle ligamentous instability, namely cranial cruciate, caudal cruciate and/or collateral ligaments; and one had a distal patellar fracture.
Thirty-two cats (38%) had bilateral PL. None of the cats with bilateral PL had single-session bilateral surgery. When bilateral corrective surgery was performed, the surgeries were staged by at least 6 weeks.
One stifle (1%) had grade 1 PL; 36 stifles (42%) had grade 2 PL, 33 stifles (39%) had grade 3 PL; and 15 stifles (18%) had grade 4 PL. Eighteen stifles (21%) had a known traumatic episode.
Eleven stifles (13%) had previous surgery and 74 (87%) did not. Of the 11 stifles with previous surgery, four (5%) had distal femoral articular fracture repair, five (6%) had soft tissue corrective procedures for PL, one (1%) had soft tissue corrective procedures and block femoral sulcoplasty for PL, and one (1%) had surgery for cranial cruciate ligament instability.
Fifty-four stifles (63%) had TTT and 31 (37%) did not. Forty-two stifles (50%) had femoral trochlear wedge recession sulcoplasty, 30 (35%) had block recession sulcoplasty, two (2%) had chondroplasty and 11 (13%) did not have a sulcoplasty procedure. Thirty-one stifles (37%) had lateral imbrication performed, 36 stifles (42%) had lateral imbrication and medial release, one stifle (1%) had a lateral release and 17 stifles (20%) did not have a soft tissue procedure. Eight stifles (10%) had an anti-rotational suture placed. Three stifles (4%) had partial para-sagittal patellectomy when PL persisted intraoperatively, despite corrective surgery; 14 one of these stifles was a revision of surgery for medial PL that resulted in lateral PL, that is reluxation.
Complications identified with logistic regression analysis
Table 1 shows the results of the binary logistic regression.
Results of binary logistic regression analysis showing the probability of complication occurrence
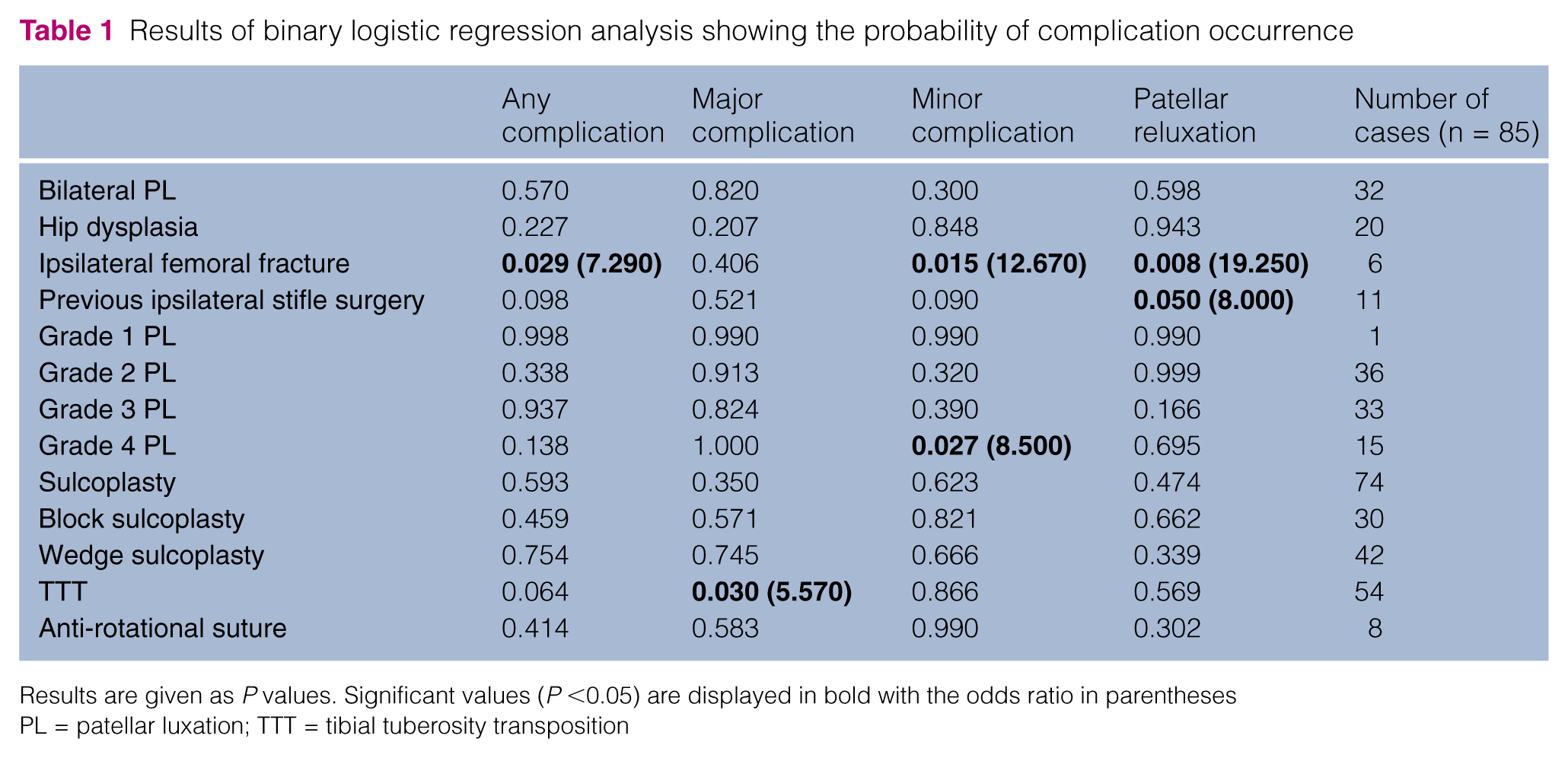
Results are given as P values. Significant values (P <0.05) are displayed in bold with the odds ratio in parentheses
PL = patellar luxation; TTT = tibial tuberosity transposition
Postoperative complications occurred in 22 stifles (26%). Seventeen stifles (20%) had major complications requiring further surgery, including four stifles with patellar reluxation. Five stifles (6%) had minor complications that did not require further surgery.
Eight of 17 stifles (47%) that suffered major complication had further surgery to remove the implants, and two had implant removal and replacement. Three stifles (three cats) suffered tibial fracture; all had surgical stabilisation. Two recovered uneventfully, but the third had pelvic limb amputation because the incision for the tibial fracture stabilisation surgery failed to heal. Four stifles (four cats) developed patellar reluxation; three had revision surgery, of which two were successful, but one cat died during anaesthesia for the revision surgery. The fourth cat with reluxation had the limb amputated owing to persistent lameness. The reluxations were all documented at the postoperative checks; two were seen at 4 weeks postoperatively, one at 6 weeks and one at 8 weeks.
Minor complications occurred in five stifles (6%). Three stifles had seromas or soft tissue swelling. One had suspected surgical site infection, which was culture negative but resolved with antibiotic administration. One case of patellar subluxation was recorded. None of these cases required further surgical management.
TTT
Fifty-four stifles had TTT performed. Twenty-eight percent had major complications, including nine cases that required revision surgery owing to a problem with the implants used to stabilise the TTT; one had chronic lameness due to stifle septic arthritis, three had tibial fractures and two had revision surgery for patellar reluxation. Three (6%) had minor complications (seroma/soft tissue swelling for two stifles and wound infection in one). Thirty-six stifles (63%) did not have any complications. TTT was significantly more likely to result in a major complication than compared to stifles without TTT performed (P = 0.03, odds ratio [OR] = 5.57, 95% confidence interval [CI] 0.04–0.84).
Femoral sulcoplasty
Forty-two stifles had femoral trochlear wedge recession sulcoplasty. Eight stifles (19%) had a major complication, including one (2%) patellar reluxation; two (5%) had a minor complication; 31 (74%) did not have complications. Of the 30 stifles that had block sulcoplasty, four (16%) had major complications, including one reluxation; two (7%) had minor complications; 23 (77%) did not have complications. Performing sulcoplasty did not change the risk of complications compared with no sulcoplasty (P = 0.59).
None of the three stifles that had partial para-sagittal patellectomy suffered complications.
Grade 4 PL
Fifteen stifles (17%) had corrective surgery for grade 4 PL. Three (20%) stifles suffered major complications; two had implants removed, one of which had a synovial biopsy that cultured Staphylococcus aureus, and the other of which had grade 4 patellar reluxation that was treated by amputation. Three (20%) stifles had minor complications consisting of wound infection, seroma formation and patellar subluxation. Nine (60%) of these did not have complications. Corrective surgery for grade 4 PL was significantly more likely to result in minor complications compared with surgery for grades 1–3 combined (P = 0.03, OR = 8.50, 95% CI 1.20–56.35).
Previous stifle surgery
Eleven stifles (13%) had previous surgery; six were for correction of PL. Four stifles (36%) had surgery for ipsilateral femoral fractures. One stifle (9%) had stabilisation surgery for concurrent lateral collateral, cranial and caudal cruciate ligament damage. One stifle (9%) had a major complication resulting in further surgery for implant removal and a positive culture of a synovial biopsy. Two stifles (18%) had patellar reluxation. Two stifles (18%) had minor complications (wound infection and patellar subluxation). Six stifles (54%) did not have complications. Previous stifle surgery was significantly more likely to result in patellar reluxation (P = 0.05, OR = 8.00, 95% CI 0.02–0.99).
Previous femoral fracture
Six stifles (7%) had a history of previous ipsilateral femoral fracture; four had distal articular femoral fractures that involved stifle surgery, and two had proximal comminuted femoral fractures. Of the stifles that had previous ipsilateral femoral fracture, two suffered patellar reluxation and two developed minor complications (one had wound infection and the other had patellar subluxation). Logistic regression analysis revealed that previous ipsilateral femoral fracture was significantly more likely to result in a complication (P = 0.03, OR = 7.29, 95% CI 1.23–43.26), including minor complications (P = 0.02, OR = 12.67, 95% CI 1.62–98.62)and patellar reluxation (P = 0.01, OR = 19.25, 95% CI 2.10–174.19).
Non-significant factors
The presence of bilateral PL, hip dysplasia, grade 1, 2 or 3 PL, corrective surgery using an anti-rotational suture, or type of trochlear sulcoplasty did not significantly affect the likelihood of complications.
Table 2 highlights the procedures performed on the different PL grades and the percentage outcome for each grade.
Cases grouped according to grade of patellar luxation (PL), number of individual surgical procedures performed and the associated complication rate outcome for each grade of PL. Each entry shows absolute case numbers (%)

Uni- and multivariable analysis
Univariate analysis for all complications demonstrated that previous ipsilateral stifle surgery, femoral fracture and TTT were associated with an increased risk of a complication. Multivariable analysis showed that previous ipsilateral femoral fracture (P = 0.03) was an independent risk factor for any complication.
For minor complications, previous ipsilateral femoral fracture, stifle surgery and grade 4 PL were identified as risk factors. Multivariate analysis did not identify independent risk factors.
For patellar reluxation, ipsilateral femoral fracture and previous stifle surgery were subjected to multivariable analysis, which showed that previous stifle surgery was not an independent predictor of reluxation.
Follow-up
Follow-up information was available for 44 stifles (52%). Median follow-up time was 18 months, (range 1–124 months). Thirty-two of the 44 stifles with follow-up information (72%) had information derived from an owner questionnaire and 12 stifles (27%) from examination by the referral veterinary surgeon. Four stifles (9%) were classed as having an excellent outcome with no detectable lameness. Thirty-nine stifles (89%) had a good outcome with mild, intermittent lameness. One stifle (2%) had a poor outcome with consistent lameness.
Discussion
This retrospective study investigated the surgical techniques commonly employed for correction of feline PL, and documented surgical outcomes and risk factors for complications. Seventy-four percent of stifles had successful surgical correction with no complications recorded. We conclude that, in general, the surgical techniques used to correct PL in dogs, namely trochlear sulcoplasty, TTT and soft tissue procedures (lateral or medial imbrication and/or release), can be performed in cats with good success, but with a 26% complication rate. This is in broad agreement with a previous report, which found that 65% of 42 cats with PL treated surgically had an excellent clinical outcome. 9
The overall complication rate of 26% is difficult to benchmark or compare directly as the surgical complication rate for PL has not been previously reported for cats. The rate of 26% is similar, but higher, to that reported in dogs; a similar canine study documented an overall complication rate of 18%. 12 Similarly, our major complication rate of 20% in cats is higher than that previously reported in dogs (13%), but the minor complication rate of 6% in cats is identical to that reported in dogs, and the 5% patellar reluxation rate in cats is lower than the 8% reported in dogs. 12
The most common major complications were TTT-associated implant-related problems (10 stifles). This is different to what has been reported in dogs, where the majority of major complications (65%) were patellar reluxation; 12 in that study, performing TTT reduced the frequency of patellar reluxation/major complications, presumably because of improved quadriceps alignment. In our feline study, only 2/54 cases that had TTT surgery (4%) suffered patellar reluxation, compared with 2/31 (6%) cases that did not have TTT, but this was not statistically significant. In dogs, 7/115 (6%) that had TTT and 4/16 (25%) that did not have TTT surgery had reluxation. This protective effect of TTT surgery against patellar reluxation in dogs did not occur in our feline cases. 12 Conversely, 15/54 (22%) feline TTT cases had implant-related problems or tibial fracture compared with 4/115 (4%) canine TTT cases, 14 indicating that complications associated with TTT surgery occur much more frequently in the cat. Factors that might explain this difference could be the use of relatively oversized implants (tibial tuberosity K-wires) in the cat; different handling properties of the bone; for example, brittleness of feline bone; a relatively smaller and therefore less robust tibial tuberosity fragment created by the osteotomy procedure because of the more slender feline tibia and less pronounced tibial tuberosity; or the feline tibial tuberosity being exposed to proportionately higher avulsive forces and therefore risk of movement and/or fracture, which could be associated with the cat’s behaviour of being likely to jump onto high surfaces, or the feline stance with the stifle held in a more flexed position. We conclude that the benefits of performing a tibial tuberosity in the cat are less than for a dog, and the associated complication rate is higher; that is, the relative benefit compared with risk appears be lower in the cat compared with the dog.
In this study, performing sulcoplasty was associated with a reduced rate of PL (9% reduced to 4%) but the difference was not statistically significant. This is in contrast to a canine study that showed a larger and significant reduction in patellar reluxation rate associated with sulcoplasty compared with no sulcoplasty (21% to 6%). 12 A canine study evaluated surgical treatment of PL without femoral sulcoplasty, but the reluxation rate was 18/91 (20%). 13 The reason that sulcoplasty appears to be more effective in controlling PL in dogs compared with cats is likely due to conformational anatomical differences. The femoral sulcus depth is likely a more important factor in determining correct patellar tracking in the dog compared with the cat; the feline patella is wider and thinner relative to the femoral trochlear sulcus.14,15 Unlike dogs, many clinically normal cats have mediolateral laxity of the patella, and patellar subluxation is a common finding in the normal cat, suggesting that absolute constraint of patellar tracking by the trochlear sulcus is not necessary.1,9,15 Hence, careful case selection for each surgical technique is necessary for good outcomes. It is possible that this study was underpowered for certain procedures; that is, if the numbers of stifles that had a sulcoplasty performed had been greater, a statistically significant difference in complication rate may have been determined.
Cats having suffered a previous ipsilateral femoral fracture had a 19 times increased risk of postoperative patellar reluxation; 66% of the group developed postoperative complications, perhaps due to altered femoral shape or alignment, namely altered alignment of the quadriceps mechanism. It is important that surgeons and owners of cats with PL that have suffered previous ipsilateral femoral fracture are made aware of the increased risk of complications. The major limitation with this subgroup is the small numbers. However, uni- and multivariate logistic regression analysis both identified ipsilateral femoral fracture as having an increased risk of complications, including patellar reluxation.
A limitation of this study is associated with the small case numbers for each group of surgical treatment type. It is very challenging to gather clinical data on high numbers of cats with surgically managed PL as clinically significant PL in cats is not common, with a prevalence of 14%, and the fact that the majority of these cases do not require surgical management. 1 Despite pooling data from four large referral centres and collecting data spanning over more than a decade, only 85 surgical cases were included.
Another limitation of this study relates to its retrospective nature; the data retrieved rely on accurate observations and recording. Case management and surgical techniques were not standardised and were at the clinical discretion of the lead surgeon for each case. The relationship between surgeon and outcome was not interrogated for numerous reasons, including the length of the study period and the number of surgeons involved; this is a limitation of the study. Radiographs were not standardised and were not available for all cases; therefore, radiographic data were excluded. Minor complications may be underrepresented owing to lack of standardisation of follow-up examinations, and owners perceiving a good clinical outcome when conditions such as patellar subluxation may persist. It is less likely that major complications, such as PL, would be under-represented, as this would more likely instigate veterinary follow-up.
The statistical analysis was complex as each surgical case had a different combination of multiple procedures performed, but the components of each surgical procedure were analysed as individual techniques. Some of the surgical procedures were performed in only very small numbers of stifles, making statistical analysis impossible to meaningless; for example, only three stifles had partial para-sagittal patellectomies.
Conclusions
This study has shown that surgical techniques commonly used for correction for PL in dogs can be applied successfully in the cat. In this population, 74% of stifles achieved a successful surgical outcome with no complications, 6% had minor complications and 20% had major complications, including 5% patellar reluxation. Previous ipsilateral femoral fracture, grade 4 PL and performing TTT were significantly more likely to result in complications. This information enables the feline orthopaedic surgeon to more accurately assess the benefits and risks of performing the corrective surgical procedures for PL in the cat, and to counsel owners appropriately.
Footnotes
Acknowledgements
We would like to thank Dr Ruby Chang for all her assistance and advice with the statistical analysis.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.