
Abstract
Practical relevance:
Osteoarthritis, a degenerative non-inflammatory joint disease, is common in cats, usually causing gradual changes in behavior and lifestyle rather than severe lameness. Inflammatory arthritis occurs much less frequently and is nearly always associated with debilitating lameness. It may have an infectious or immune-mediated cause – but, unlike the canine disease, is much more likely to be infectious in origin.
Clinical challenges:
Cats with inflammatory joint disease are presented for evaluation of lethargy, anorexia, reluctance to walk or fever. Synovial fluid collection and analysis is required to confirm joint inflammation, but this is a procedure many veterinarians are not comfortable performing in cats. Once inflammatory arthritis is confirmed, extensive testing is required to diagnose infectious causes and determine appropriate treatment. Immune-mediated polyarthritis can be treated with immunosuppressive drugs only after all infectious possibilities are eliminated. Radiographs are used to characterize the arthritis as erosive or nonerosive, but radiographic changes in cats are often subtle compared with those described in canine rheumatoid-like arthritis.
Audience:
This review, aimed at all veterinarians who treat cats, describes the general clinical approach to feline joint disease, the collection and analysis of synovial fluid, and the diagnosis and management of inflammatory joint diseases affecting cats. The diagnostic approach to an unusual case of erosive polyarthritis is discussed in the Case Notes.
Evidence base:
To date, the veterinary literature on inflammatory joint disease in cats has been limited to older reviews of immune-mediated disorders and multiple single case reports or small case series describing infectious disorders. This article offers a current comprehensive review of these disorders.
Disorders of the joints
Disorders affecting the joints can be either non-inflammatory or inflammatory. Non-inflammatory conditions are most common in both cats and dogs, and include developmental, degenerative and neoplastic disorders, and traumatic injury. Osteoarthritis (OA), a degenerative disorder once thought to be rare in cats, is actually common in this species, but diagnosis can be challenging because many affected cats are minimally symptomatic.1 –3 Lameness is rare in cats with OA, but vague alterations in behavior and lifestyle can be detected by an astute clinician asking the right questions. Age-related (primary) cartilage degeneration or OA secondary to congenital joint deformities or acquired traumatic injury have been identified in 50– 90% of mature and geriatric cats.1 –5
Inflammatory joint disorders can be infectious or immune-mediated, and may affect one joint or multiple joints (polyarthritis). Polyarthritis is further classified as being erosive or non-erosive based on physical examination and radiographic findings. In cats, unlike dogs, infectious causes of arthritis are much more common than primary immune-mediated disorders.6 –8 Infectious causes of arthritis include bacteria, bacterial L-forms, Mycoplasma species, calicivirus, feline infectious peritonitis virus, fungi (primarily cryptococcal and Histoplasma species), and some tick-borne rickettsiae.6,7,9 –14 Most of these infectious agents cause non-erosive arthritis, with the possible exception of Mycoplasma species.10,15,16 Infectious disorders primarily cause arthritis by direct infection of the synovium, but occasionally systemic infections give rise to circulating immune complexes that are deposited in joints, resulting in a sterile synovitis known as reactive polyarthritis.6,9,17
Clinical manifestations of inflammatory joint disease are typically more acute and severe than those seen in cats with OA. Cats with monoarthritis are obviously lame. A shifting-leg lameness or ‘walking on eggshells’ gait can be seen in cats with polyarthritis, although many simply refuse to walk. When inflammation is severe, affected joints are swollen and painful. Erosive disorders may cause palpable joint instability or deformity. Systemic signs of inflammation, including lethargy, anorexia and fever, are common, although some cats with chronic low grade joint inflammation are systemically normal while they develop slowly progressive lameness and joint deformity.18,19

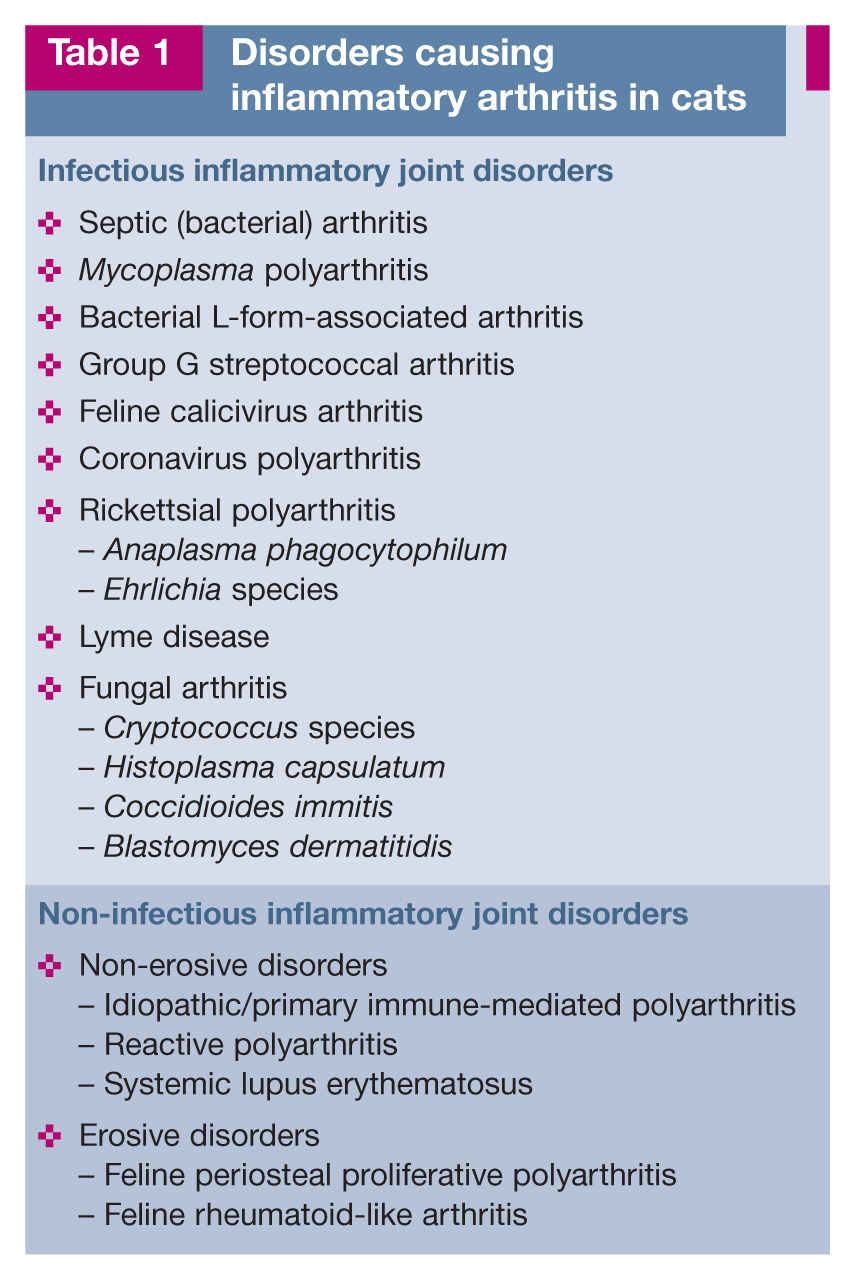
Disorders causing inflammatory arthritis in cats are listed in Table 1.
Disorders causing inflammatory arthritis in cats
Diagnostic approach
Clinical examination
Cats with non-specific pain, lameness, a stiff gait, reluctance to walk, or owner-perceived changes in their normal physical activities should be evaluated with a careful physical and orthopedic examination. 5 Many cats with OA have joints that are normal on palpation, whereas pain and swelling are present in most inflamed joints.3,5,7,9,17 –19 Inflammatory arthritis is uncommon; most cats presenting with vague signs such as lethargy, inappetence and fever have a cat bite abscess, pancreatitis or a viral infection, but the possibility of polyarthritis should not be discounted. Inflammatory arthritis will be missed unless clinicians maintain a high index of suspicion for this disorder.
Arthrocentesis
Synovial fluid collection and analysis is required to confirm a diagnosis of inflammatory arthritis. Synovial fluid should be collected and evaluated from at least five joints, even in cats with apparent monoarticular inflammation, since one joint is often more obviously inflamed and painful than others in cats with polyarthritis. Landmarks vary according to personal preference, but some recommended approaches are outlined in the boxes on pages 549–551. 20
Reluctance by veterinarians to perform arthrocentesis probably results in significant underdiagnosis of inflammatory joint disease in cats, yet with experience many clinicians find synovial fluid collection in cats easier than in dogs. Samples are readily obtained from the radiocarpal and intercarpal joints, elbow, hock, stifle, and even the metacarpophalangeal and interphalangeal joints when they are swollen or painful. Fluid should always be collected from joints that are swollen and painful, although less clinically inflamed joints can also yield a diagnosis. Immunologically mediated disease tends to be most pronounced in the distal small joints, such as the hock and carpus.6,8,18 Bacterial infective arthritis is most likely to affect larger joints like the stifle and elbow in dogs. However, that is not necessarily the case in cats, where infections often occur following cat bite inoculation of distal joints.6,8,9,17
General anesthesia is recommended for collection of synovial fluid. The site should be clipped, the skin surgically prepared, and sterile gloves, needles and syringes used. Most joints can be tapped using 25 gauge 5/8 inch needles, but 22 gauge 1 inch needles will be required for the hip and perhaps for the stifle, elbow and shoulder in large cats. The needle should be connected to a 3 ml syringe and introduced into the joint. Once the tip of the needle is in the joint space, gentle negative pressure is applied to the syringe. 20 Only a very small amount of joint fluid (one to three drops) is needed. Once fluid is obtained, negative pressure is released and the needle is withdrawn from the skin. The needle is disconnected from the syringe, air is drawn into the syringe, the needle is reattached, and the air is used to expel a drop of synovial fluid onto a microscope slide to assess viscosity, color and clarity. A second slide is placed over the drop, compressing it gently, and the two slides are pulled apart to make a smear for cytologic evaluation.



Synovial fluid analysis
The volume of synovial fluid that can be obtained from a normal cat joint is small – one to three drops (0.1 ml) from the carpus, hock and interphalangeal joints, and 0.25 ml from the larger joints. 21 One drop is adequate for determination of color, clarity and viscosity, as well as estimated cell count and differential white blood cell count. Larger volumes of fluid (0.2–0.4 ml) are easily obtained from inflamed joints for culture.
Normal joint fluid is very viscous, colorless and clear (Figure 1). Diffuse hemorrhagic or yellow (xanthochromic) discoloration suggests prior intra-articular hemorrhage. Turbidity suggests an increase in red or white blood cell count. Reduced viscosity suggests inflammation.6,20

Normal joint fluid is very viscous (stringy) due to a high hyaluronic acid content. Reproduced, with permission, from Taylor SM. Small animal clinical techniques. Elsevier, 2010
Absolute cell counts are rarely performed because samples are small. Estimated cell numbers should be less than 3000 cells/µl.6 –9 As reported for dogs, most cells are mononuclear (>95%) and neutrophils represent less than 10% of the total nucleated cell count (TNCC), even when there is mild blood contamination. Synovial fluid from cats with OA may have a slightly increased TNCC but the cell distribution is still predominantly mononuclear cells, with low numbers of neutrophils. 22 An increase in the number of neutrophils, to greater than 10% of the TNCC, indicates that there is inflammation of the synovial lining. The more inflamed the synovium, the greater the number of white blood cells and the greater the percentage of neutrophils.6,9
Neutrophils in synovial fluid from joints with immune-mediated disease will have a normal appearance, as will neutrophils from joints affected by rickettsial polyarthritis, but occasionally intracytoplasmic organisms (morulae) are observed within cells in cats with anaplasmosis or ehrlichiosis.6,8,14 In acute or severe septic arthritis, neutrophils may appear toxic, ruptured or degenerate and intracellular bacteria may be seen. Inflammatory joint fluid should always be cultured, because some organisms (eg, Mycoplasma species) do not induce these cytologic abnormalities.6,15,16
Synovial fluid should always be submitted for aerobic and anaerobic culture, and swabs submitted for specific Mycoplasma species culture. Direct bacterial culture of synovial fluid is positive in only about half of all cases of septic arthritis.6,20 The use of broth-enrichment media (eg, thioglycolate blood culture bottles) and incubation for 24 h prior to culture greatly increases the rate of positive culture (85–100% positive). 6 Culture of blood, urine and synovial membrane biopsy samples can also improve the chance of recovering a clinically relevant pathogen.
Additional tests
All cats with inflammatory joint disease should be tested for feline immunodeficiency virus (FIV) and feline leukemia virus (FeLV) since immunosuppression may be an important predisposition for infectious arthritis and FeLV has been implicated in the development of periosteal proliferative polyarthritis. Immunologic and serologic testing for Borrelia, rickettsiae and other infectious agents may be warranted in endemic regions. When reactive polyarthritis is a possibility, a complete blood count, biochemical panel, urinalysis, thoracic and abdominal radiographs, abdominal ultrasound, culture of urine and blood, and lymph node aspirates should be recommended in order to identify underlying chronic infections or neoplasia.6,8,9
Radiographs are an important part of the initial evaluation of cats with mono- or polyarthritis in order to determine whether their disease is erosive or non-erosive. When interpreting radiographs, it is important to appreciate that incidental radiographic abnormalities due to OA are common in cats. 1 Feline OA causes osteophytes and periarticular and meniscal mineralization – not the synovial effusion, destructive ‘punched out’ subchondral and periarticular lesions, and joint subluxation associated with erosive disease.1,3,4,9,18,23
Infectious inflammatory joint disorders
Septic (bacterial) arthritis
A cat bite wound penetrating the joint is the most common cause of feline septic arthritis. Pasteurella species and coliform organisms are most often incriminated.6,17 Septic arthritis due to inoculation during a cat fight usually involves only one joint, and the carpus, hock and interphalangeal joints are at highest risk. Bacterial infection of multiple joints (suggesting hematogenous spread of bacteria) is rare, but can be seen in neonatal kittens with omphalophlebitis. Cats with septic arthritis are often systemically ill, febrile and depressed. Affected joints are painful, with palpable joint and periarticular swelling.
To confirm a diagnosis of septic arthritis, bacteria must be identified in cytologic preparations of synovial fluid or cultured in synovial fluid, blood or urine from a cat with appropriate clinical signs.6,9 Synovial fluid is often yellow, cloudy or bloody, and less viscous than normal. There is a marked increase in TNCC, with neutrophils predominating (usually >90%). Bacteria may be evident within the cells and neutrophils may be toxic, ruptured or degranulated. Organisms that do not cause rapid destruction of articular cartilage (ie, streptococci, Mycoplasma species) will not typically cause degenerative cellular changes.6,15,16 Synovial fluid should always be cultured for aerobic and anaerobic bacteria, and for Mycoplasma species.6,9
Antibiotics should be administered as soon as possible after all samples are collected. A broad-spectrum, β-lactamase-resistant antibiotic such as amoxicillin–clavulanic acid is indicated (Table 2).6,9 The quinolones enrofloxacin and pradofloxacin are also effective against Pasteurella species and should be used if coliform organisms are suspected based on cytology or culture. Although retinal toxicity is a potential concern in cats receiving quinolones, pradofloxacin has an improved safety profile (Table 2). 24 Most cats with acute monoarticular septic arthritis can be treated conservatively with systemic antibiotics, but if dramatic improvement is not seen within 2–3 days, surgery should be performed to flush enzymes and fibrin debris from the joint and debride infected tissue.6,9 A minimum of 4–6 weeks of antibiotic therapy is administered, and cage rest is recommended to facilitate healing of articular cartilage. Analgesic medications are also administered, as needed (Table 3).3,25
Antibiotics used to treat infectious arthritis in cats

Suggested doses of analgesics for use in cats

Mycoplasma arthritis
Mycoplasma species are normal inhabitants of the conjunctival membranes, pharynx, and upper respiratory and urogenital tracts, and are generally considered non-pathogenic. Mycoplasma gateae and Mycoplasma felis have, however, been associated with erosive and non-erosive polyarthritis and tenosynovitis in cats.10,15,16,26,27 Mycoplasma polyarthritis occurs primarily in debilitated or immunosuppressed animals, but has also been described in apparently immunocompetent cats.16,27 Cats with polyarthritis associated with Mycoplasma species should be tested for FIV and FeLV, lymphoma and other immunosuppressive disorders.
Mycoplasma polyarthritis typically results from hematogenous spread of the bacteria to the joints. In one study, healthy cats and immunosuppressed cats injected intravenously with M gateae isolated from a naturally infected cat all developed polyarthritis. 10 The naturally infected case and the immunosuppressed cats were severely affected, whereas the immunocompetent experimentally infected cats only exhibited mild transient lameness and recovered without treatment. 10 Naturally occurring M felis was identified as the cause of monoarthritis in two cats in another report. 27 Direct inoculation of the elbow was suspected in one cat and bacteremia with hematogenous spread to the hock after trauma was suspected in the other. 27
Cytology of synovial fluid shows an increase in normal neutrophils with no visible organisms, similar to the expected findings in non-infectious immune-mediated arthritis.9,15 Mycoplasma species can be difficult to culture, requiring specialized media. In one case report, isolation of M gateae, a facultative anaerobe, was only successful under strict anaerobic conditions. 15 Inflammatory joint fluid from cats should always be specifically cultured for Mycoplasma species and empirical treatment with oral doxycycline for 3 weeks is recommended before treating culture-negative polyarthritis with immunosuppressant drugs.
Mycoplasma polyarthritis has been described in the literature as being primarily non-erosive based on radiographs, but erosions can occur.9,10,16,26 –28 The first reported case of M gateae polyarthritis had no radiographic lesions but subchondral bone and cartilage erosions were evident at necropsy. 10 One more recently reported cat with convincing M gateae polyarthritis had a generalized decrease in radiodensity, a unique very coarse trabecular pattern in the bones of the hocks, and focal subchondral bone lysis in multiple bones of the distal limbs (Figure 2). 15

Radiographs of the left hock of a cat with Mycoplasma gateae erosive polyarthritis. There is periarticular soft tissue swelling, a coarse trabecular pattern in the bones adjacent to the hock and radiolucent foci of subchondral bone lysis (arrows). Reproduced, with permission, from Zeugswetter et al 15
Treatment of Mycoplasma arthritis with doxycycline, enrofloxacin or pradofloxacin should result in rapid clinical improvement (Table 2).15,16,27 Treatment for 6–8 weeks may be required, as relapse is common with shorter courses of treatment.15,16,27 Based on data from the few cases reported in the literature and experimental studies of antibiotic treatment of hemotropic Mycoplasma species, the quinolone antibiotics may be more effective than doxycycline at actually eliminating the organism.15,16,29
Bacterial L-form-associated arthritis
L-forms of bacteria are cell wall-deficient forms morphologically similar to Mycoplasma. These organisms have been isolated from cats with a syndrome of fever, cellulitis and polyarthritis. 11 Cats are infected by direct inoculation, usually through bite wounds, and the infection spreads locally and hematogenously to cause cellulitis, draining tracts, polyarthritis and subcutaneous abscesses (Figure 3). An epizootic outbreak was described in three cats living in one household. 30 Cytology of aspirates from joints and subcutaneous abscesses showed mixed inflammation containing macrophages, neutrophils and few lymphocytes but no organisms; and fungal and bacterial cultures, including for Mycoplasma species, were negative. The infection was resistant to treatment with many antibiotics but susceptible to tetracycline, and the infection was transmitted experimentally to specific pathogen-free cats by subcutaneous injection of cell-free material, leading to the suspicion of L-form bacteria. 30 Electron microscopic evaluation revealed the characteristically pleomorphic, cell wall-deficient organisms within phagocytes.11,30

Distal pelvic limb of a cat with bacterial L-form infection, showing multiple fistulas draining purulent exudate. Reproduced, with permission, from Greene CE and Chalker VJ. Nonhemotropic mycoplasmal, ureaplasmal and L-form infections. In: Greene CE (ed). Infectious diseases of the dog and cat. Elsevier, 2012
Radiographic abnormalities in cats with L-form arthritis include periarticular soft tissue swelling and periosteal proliferation progressing to damaged articular cartilage and subchondral bone. 11
This disorder should be suspected when cellulitis, subcutaneous abscesses and draining tracts occur in a cat with culture-negative arthritis. Treatment with doxycycline or quinolone antibiotics should result in clinical improvement within a few days (Table 2). Therapy should continue for 4–6 weeks or at least 1 week after draining lesions have healed.
Group G streptococcal arthritis
Beta-hemolytic streptococci are normal microflora in the skin, and upper respiratory and genital tracts of cats but occasionally cause severe infections. Most clinically important infections are caused by Lancefield group G streptococci and are Streptococcus canis. 31 Neonatal kittens may develop omphalophlebitis and bacteremia after being infected with streptococci from the vagina of the queen. 31 Juvenile kittens (3–7 months old) with untreated S canis pharyngitis, tonsillitis and cervical lymphadenitis may occasionally progress to septicemia and embolic pneumonia, myocarditis, pyothorax or arthritis.31,32
S canis was suspected to be the cause of purulent mono- and polyarthritis in six kittens aged 2–23 weeks old from different litters in a closed breeding colony during a 6 month period. 32 Five kittens recovered after 5 days of treatment with penicillin and streptomycin, and necropsy of the one untreated kitten revealed synovitis, destruction of articular cartilage and a pure culture of group G S canis. 32 Group G streptococci are very sensitive to penicillin and its derivatives amoxicillin and ampicillin (Table 2).
Feline calicivirus arthritis
Feline calicivirus (FCV) is a common pathogen of cats, causing fever, sneezing, nasal discharge, conjunctivitis, and oral and nasal ulceration. Occasionally, infected cats develop acute synovitis and lameness, either alone or together with the typical signs of FCV infection. Experimental inoculation with field strains of FCV isolated from cats exhibiting lameness is more likely to induce polyarthritis than inoculation with most vaccine strains of FCV, but polyarthritis can definitely occur following vaccination. 12 In one study of apparent reactions occurring within 21 days of vaccination with three different systemic modified-live FCV vaccines, 80% of 123 vaccine reactions were associated with lameness and fever alone or in association with acute oral/respiratory disease. 33 Virus isolated from oropharyngeal swabs from symptomatic cats was rarely identical to the vaccinated virus, suggesting that either the lameness was caused by a field strain of FCV that was being incubated at the time of vaccination or the vaccine virus had been slightly altered by passage through the cat. 33
Polyarthritis associated with FCV seems to occur primarily in kittens 5–7 days following their first vaccination (Figure 4).6,12,33 In addition to lameness, many affected kittens are febrile, and some have concurrent acute oral or respiratory signs. Synovial fluid analysis reveals a mildly to greatly increased TNCC, with small mononuclear cells and macrophages predominating, as well as increased neutrophils. Bacterial and Mycoplasma species cultures are negative. FCV can be isolated from the oropharynx of some infected cats or from synovial tissues. Lameness and fever usually resolve spontaneously after 2–5 days, so diagnostic evaluation may not be necessary in kittens presenting with a classical history and clinical examination findings.

Presumed calicivirus polyarthritis in a 10-week-old kitten exhibiting swollen joints, lameness and fever 6 days after modified-live virus vaccination. Reproduced, with permission, from Taylor SM and Scott-Moncrieff CR. Disorders of the joints. In: Nelson RW and Couto CG (eds). Small animal internal medicine. 5th ed. Elsevier, 2013
Short-term administration of an analgesic medication such as buprenorphine by oral mucosal application (Table 3) may be recommended.3,25
Coronavirus polyarthritis
Fever and lameness due to generalized synovitis are occasionally recognized in cats with the dry or wet form of feline infectious peritonitis. This is due to immune complex deposition (reactive polyarthritis) in some cats, but in others coronavirus-infected macrophages can be identified within the synovium. 13
Rickettsial polyarthritis
Non-erosive polyarthritis is a common manifestation of many tick-borne rickettsial diseases in dogs, but has been only rarely described in cats.
Anaplasma phagocytophilum
Susceptibility of cats to Anaplasma phagocytophilum was first demonstrated experimentally, with inoculated cats developing morulae in circulating neutrophils either in the absence of clinical signs of disease or with only mild pyrexia.34,35 More recently, confirmed naturally occurring feline granulocytotropic anaplasmosis has been reported in cats from several countries, including the United States, Poland, Finland, Sweden, Denmark, Ireland, Italy and the UK.14,35 –38 The most common clinical signs described are fever, lethargy and anorexia. Other reported signs are lymphadenomegaly, epistaxis, weight loss, conjunctivitis, neurologic abnormalities, tachypnea and ocular discharge. 35 Thrombocytopenia sufficient to cause bleeding may occur. Although a few infected cats have exhibited fever, swollen painful joints and lameness, synovial fluid analysis was not performed so polyarthritis has not been confirmed.14,36,38 A phagocytophilum is transmitted by Ixodes species ticks in other species, and all confirmed feline cases have lived in a region where the tick is endemic, making this vector likely in cats.35,39
Microscopic detection of inclusion bodies within neutrophils (Figure 5) in a clinically ill cat is highly suggestive of the diagnosis, but morulae can be scarce and difficult to find, so serologic or nucleic acid detection methods are generally needed to confirm the diagnosis. Antibodies detected by indirect immunofluorescence assay can be measured, but results are often negative during acute infection, cross-reactivity with Ehrlichia species occasionally occurs, and a single positive titer cannot differentiate active disease from previous infection.35,39 In addition to serologic testing, cats with suspected anaplasmosis should ideally be evaluated with a genus-inclusive PCR assay to detect co-infection with other tick-borne pathogens.35,39

(a,b) Morulae (arrows) in neutrophils from two cats with Anaplasma phagocytophilum infection. Reproduced, with permission, from Adaszek et al 36
Recommended treatment of cats with suspected anaplasmosis includes supportive care, fluid therapy when necessary, and administration of doxycycline for 3–4 weeks (Table 2).
Ehrlichia species
The species of Ehrlichia that infect cats after natural exposure have not been fully determined. 40 Numerous cases have been reported in which feline monotropic ehrlichiosis was suspected in sick cats based on finding morulae in mononuclear cells and documenting positive Ehrlichia canis serology or a positive response to anti-ehrlichial drugs, but only a few cats have had E canis-like DNA isolated from their blood.40 –42 Fever, inappetence and weight loss are reported in most of the confirmed and suspected cases. Hyperesthesia and joint pain have also been commonly described, suggesting polyarthritis.41,42 One infected cat did have synovial fluid examined, revealing neutrophilic, culture-negative inflammation. 41 Neutropenia and thrombocytopenia occur in some cats, while others exhibit neutrophilia. Not all infected cats are seropositive. Confirmation of Ehrlichia species infection using PCR is recommended, but only possible through a research laboratory at this time.
Cats with suspected clinical ehrlichiosis should be treated with doxycycline for a minimum of 28 days (Table 2). 40 It is unknown if this treatment protocol will eliminate the organism.
Lyme disease
Despite evidence of seropositivity to Borellia burgdorferi in endemic regions at a rate similar to that seen in dogs, naturally occurring Lyme disease has not been described in cats.43,44 Experimentally inoculated cats seroconvert but do not develop clinically apparent disease, suggesting some resistance to progression of infection.43 –45 Cats inoculated with organisms harvested directly from arthropods did, however, develop polyarticular lameness, synovitis, meningitis and evidence of systemic inflammation.46,47
Cats with polyarthritis or meningitis from endemic regions should be serologically evaluated for Lyme borreliosis. Although marketed for use in dogs, point-of-care assays developed to detect antibodies against the C6 peptide of B burgdorferi (3Dx/4Dx SNAP, IDEXX Laboratories) are also reliable in cats. 48 Organism numbers are very low, so detection by PCR is difficult in body fluids such as blood, cerebrospinal fluid and synovial fluid, but may be rewarding when performed on infected tissues like synovium. 44
Suspected Lyme borreliosis should be treated with antibiotics. Doxycycline is generally the drug of choice, because it is effective, has good tissue distribution and will also address potentially unidentified co-infecting tick-borne pathogens such as Anaplasma, Ehrlichia and Bartonella species (Table 2). When young kittens are infected, treatment with amoxicillin may be preferred to prevent staining of tooth enamel. An immediate response is expected, but continued treatment for 4–6 weeks is recommended. 44
Fungal arthritis
Fungal arthritis is rare in all species and nearly always occurs in association with systemic fungal disease. 49 Arthritis can develop from local extension into the joint of an adjacent fungal osteomyelitis lesion or by hematogenous spread from a severe systemic fungal infection. Cryptococcus species, Histoplasma capsulatum, Coccidioides immitis and Blastomyces dermatitidis have all been implicated.49,50 In addition to true fungal arthritis, cats can develop immune complex mediated (reactive) polyarthritis secondarily to a systemic fungal infection.
Neutrophilic inflammation of synovial fluid with normal-appearing neutrophils is the most likely finding in cats with fungal arthritis and also in cats with reactive polyarthritis secondary to systemic infection. Diagnosis of fungal arthritis is straightforward when fungal organisms are identified cytologically in synovial fluid, but organisms can be scarce. 50 Thoracic radiographs, sinonasal radiographs or computed tomography, lymph node aspirates, bone palpation, thorough dermatologic and ocular examination, and abdominal palpation should all be considered when systemic fungal infection is suspected. The urine antigen test for blastomycosis cross-reacts with histoplasmosis antigen, so it is possible to use one test to screen for both diseases. 49 Serology for coccidiodomycosis is fairly reliable, as is the latex cryptococcal antigen agglutination titer (LCAT). 49 Primary immune-mediated polyarthritis is rare enough in cats that screening for an underlying cause of reactive arthritis such as systemic fungal infection should always be considered in endemic areas before proceeding with immunosuppressive therapy.
Fungal arthritis is treated with antifungal drugs. The prognosis for affected cats is related to the severity and location of the systemic fungal infection.49,50
Non-infectious inflammatory joint disorders
Non-infectious inflammatory (immune-mediated) joint disorders are very common in dogs but rare in cats.6 –9 All cats with polyarthritis should be vigorously evaluated for an infectious cause and also for a systemic infectious or neoplastic reason for reactive polyarthritis. Even when all tests are negative it is prudent to treat empirically for 14 days with doxycycline (Table 2) to gauge response before making a diagnosis of primary immune-mediated disease.
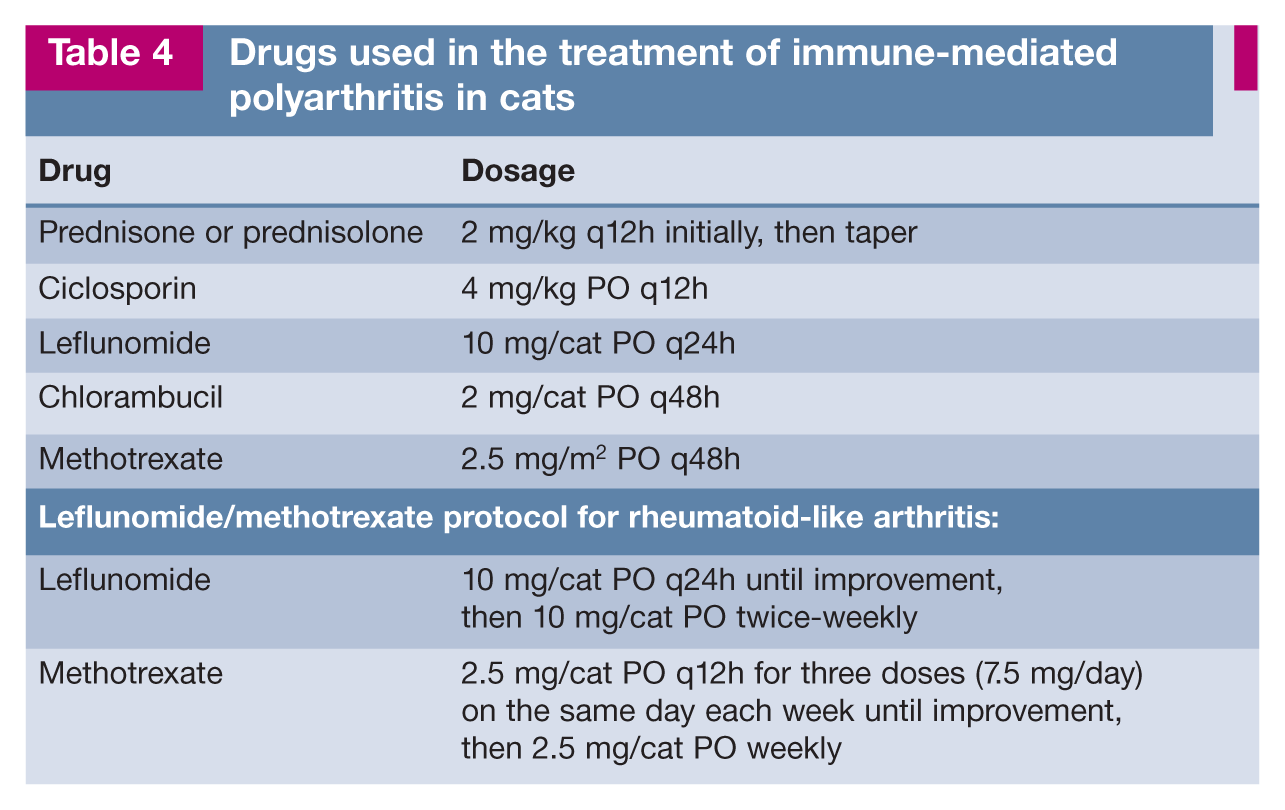
Immune-mediated joint disorders are treated with glucocorticoids and occasionally other immunosuppressive drugs (see box below and Table 4). Although most reports of treatment have involved prednisone used at immunosuppressive doses, there is growing evidence that prednisolone (dehydrocortisol) is more bioavailable than prednisone in cats; administration of identical doses of the two drugs will result in significantly higher concentrations of the active moiety, prednisolone, when prednisolone is administered. 51 A differential clinical response to the two drugs has not yet been assessed in feline patients with polyarthritis.
Drugs used in the treatment of immune-mediated polyarthritis in cats
Non-infectious immune-mediated joint disorders are classified as non-erosive or erosive based on the absence or presence, respectively, of radiographically evident joint destruction.
Non-erosive immune-mediated polyarthritis
Non-erosive immune-mediated polyarthritis is caused by deposition of immune complexes in the synovial membrane and the ensuing inflammatory response.6,9,17,18,52 This can occur as a primary or idiopathic disorder, secondarily to antigenic stimulation (reactive polyarthritis) or as a feature of systemic lupus erythematosus (SLE). Radiographic changes, even after many months of joint disease, are minimal to non-existent and are limited to soft tissue swelling.17,18,52
Idiopathic or primary immune-mediated polyarthritis
Primary idiopathic immune-mediated polyarthritis (IMPA) can be diagnosed in a cat with non-erosive polyarthritis when infectious etiologies have been eliminated and there is no evidence to support SLE or reactive polyarthritis. IMPA is the most common form of polyarthritis diagnosed in dogs, but it is very rare in cats.18,53 One study described six cats with IMPA but diagnostic evaluation was limited. 18 Four cats responded completely to a tapering dose of prednisone started at 2 mg/kg per day, but two were non-responders, and were euthanized. On necropsy, one of the non-responders had mild pyelonephritis, and Corynebacterium species were isolated from the liver and synovial membrane of the other. Also, two of the four cats that did respond to therapy were FeLV positive, suggesting that some of these cats may actually have had reactive polyarthritis rather than IMPA. 18
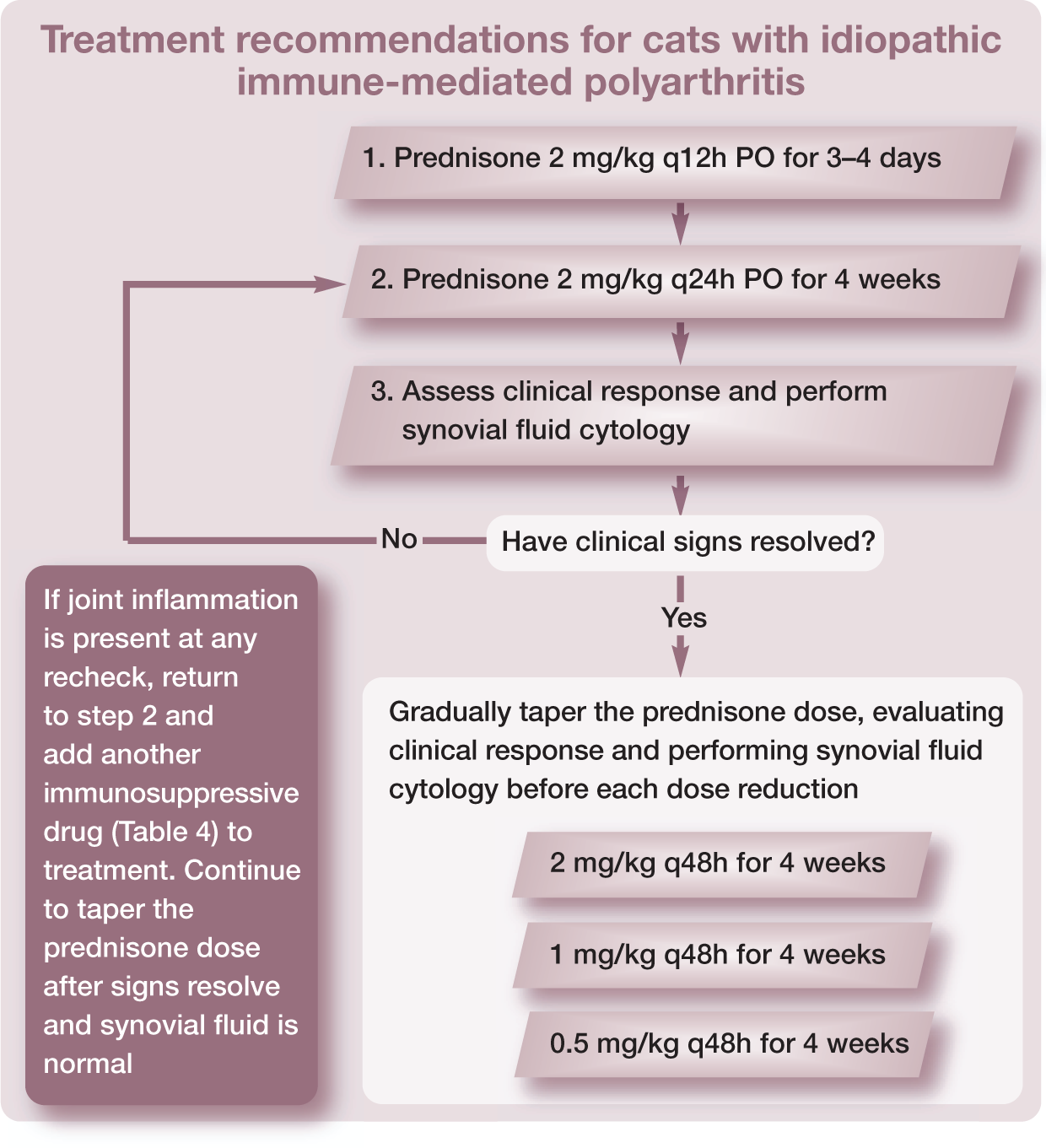
When thorough diagnostic evaluation suggests IMPA and a cat does not respond to empirical doxycycline, treatment with glucocorticoids is warranted. Immunosuppressive doses are administered initially, with monthly tapering based on clinical response and synovial fluid cytology (Table 4).6,9
Reactive polyarthritis
Reactive polyarthritis occurs secondarily to antigenic stimulation from chronic infection, neoplasia or drug administration. This disorder accounts for approximately 25% of all non-erosive immune-mediated polyarthritis cases in dogs but is much less commonly documented in cats.6,9,18,52 Infections that have been identified in cats with presumed reactive polyarthritis include pneumonia, pyelonephritis, intestinal toxoplasmosis with severe hemorrhagic enteritis, FeLV, FIP and cat bite abscess.13,18 Reactive polyarthritis has also been documented in cats with myeloproliferative disease. 18 It is likely that most cases of feline reactive polyarthritis are undiagnosed, as veterinarians suspect that a cat’s fever and unwillingness to walk are related to their primary disease, and joint taps are rarely performed.
Drugs that have been shown to occasionally cause reactive polyarthritis in dogs include sulfadiazine–trimethoprim, phenobarbital, erythropoietin, penicillin, cephalexin and routine vaccinations. 6 Reports of drugs causing polyarthritis in cats are rare, but sulfadiazine–trimethoprim has been implicated and one of the authors (ST) had polyarthritis develop in one cat on long-term erythropoietin therapy. 5
Treatment of reactive polyarthritis should be directed at eliminating the underlying disease or antigenic stimulus whenever possible. If not contraindicated by the primary disease, inflammation and pain can be controlled by short-term administration of immunosuppressive doses of glucocorticoids. Alternatively, non-steroidal drugs and analgesics can be administered (Table 3).3,6,25
Systemic lupus erythematosus
SLE is a disorder in which autoantibodies against tissue proteins and DNA result in circulating immune complexes that, when deposited in tissues, cause inflammation and organ damage.6,54 Diagnosis requires evidence of multisystemic immune-mediated disease as well as circulating antinuclear antibodies. Antinuclear antibodies can, however, occur in many inflammatory disorders other than SLE – and have been identified in cats with Ehrlichia species, FeLV and FIV infections, as well as cats being treated with propylthiouracil and methimazole.
There are very few reports in the literature of cats with convincing SLE according to criteria applied in dogs.18,54 Polyarthritis is the most commonly reported clinical manifestation of canine SLE (78%), but occurs less frequently in cats (36%). Dermatitis, fever and glomerulonephritis are more frequently reported in cats with SLE. 54 Cats with non-erosive polyarthritis as a component of multisystemic immune-mediated SLE-like disease should have testing performed to eliminate an infectious or secondary (reactive polyarthritis) cause, but thereafter treatment is identical to IMPA protocols. The prognosis for resolution of SLE polyarthritis should be good, but other systemic manifestations may be more problematic.
Erosive immune-mediated polyarthritis
Two uncommon immune-mediated disorders cause joint damage and destruction in cats. One is a periosteal proliferative polyarthritis characterized by marked periarticular periosteal new bone formation.18,19,55 The second is a deforming arthritis resembling rheumatoid arthritis in humans and dogs.18,19,55,56
Early reports referred to both of these disorders as chronic progressive polyarthritis (CPP), describing a periosteal proliferative form and a deforming variant. All of the initial cases were in male cats, and all were positive for antibodies against feline syncytium forming virus (FeSFV), also called feline foamy virus. There was speculation that CPP could result from chronic immune stimulation secondary to FeSFV infection in genetically predisposed cats immunosuppressed by FeLV or FIV infection or other factors.17,19,57 FeSFV is, however, a widespread retrovirus of cats, so the association between this virus and CPP is uncertain. Experimental infection with FeSFV does not cause clinical illness or joint pathology in cats.19,58
Feline periosteal proliferative polyarthritis
Periosteal proliferative polyarthritis occurs most often in male cats (intact and castrated), but female cats can also be affected.9,17 –19,59 Cats of any age can develop this polyarthritis, but it is most common in young adults.9,17 –19,59 Affected cats experience fever, lethargy, a stiff gait, and joint pain and swelling, particularly of the carpus and hock.7,17 –19,55 There is sometimes concurrent edema of the skin and soft tissues overlying the joints.18,19,55 Lymph node hyperplasia may cause severe regional lymph-adenopathy.7,18,19 Synovial fluid analysis reveals a moderate-to-severe neutrophilic pleocytosis and culture is negative.
Radiographic changes may not be evident for the first 10–12 weeks of illness and then early findings include periarticular soft tissue swelling and mild periosteal proliferation.17 –19 An abnormally coarse trabecular pattern of the bones of affected joints, similar to that reported in one cat with Mycoplasma polyarthritis, 15 has also been described. 19 Over time, the periosteal proliferation worsens and extends beyond the confines of the joint, which may lead to ankylosis.17 –19 Periarticular osteophytes, subchondral cyst-like lesions and periarticular erosions are evident (Figure 6).18,19,55 Calcification and erosion of bone may occur at the attachment of ligaments and tendons, causing painful lesions (enthesopathies).9,18 Synovial biopsies initially reveal neutrophilic synovitis and tenosynovitis; but, with chronicity, the proportion of lymphocytes and plasma cells increases.17 –19,55 No inflammation is evident in the periosteal new bone.17 –19

Mediolateral radiograph of the hock of a cat with periosteal proliferative polyarthritis. New bone deposits are seen on the bones of the hock and on the distal tibia and proximal metatarsus, extending beyond the confines of the joint. Lytic foci are seen in most of the tarsal bones and within the os calcis. Reproduced, with permission, from Bennett D. Immune mediated and infective arthritis. In: Ettinger SJ and Feldman EC (eds). Textbook of veterinary internal medicine. 7th ed. Elsevier, 2010
Treatment with glucocorticoids (prednisone or prednisolone) lessens the severity of signs and may slow progression of disease, but is not curative. About half of treated cats improve and have a reasonable quality of life when treated lifelong with glucocorticoids and analgesics. 18 Administration of more potent immunosuppressive drugs has been rarely reported in cases of feline periosteal proliferative polyarthritis, but should be considered based on recently reported results in cats with rheumatoid-like arthritis.18,56,59,60
Feline rheumatoid-like arthritis
Feline rheumatoid-like arthritis has an insidious onset, with lameness and joint deformity developing slowly over weeks to months. Middle-aged and older cats are most often affected, and Siamese cats may be overrepresented. 57 This disorder is generally considered to be rare, but may simply be underrecognized.7,18,56 Lameness is often noticed by the owner in only one limb but careful examination reveals swelling and pain affecting multiple distal joints in all affected cats.18,19,56 Systemic illness and fever do not occur, so these cats are rarely evaluated before severe joint deformities are evident.18,19,56 Feline rheumatoid-like arthritis is most likely the same as the deforming variant of CPP described by Pederson et al in 1980.18,19 Synovial fluid analysis reveals an increased TNCC with mixed inflammation (neutrophils, lymphocytes and macrophages). Neutrophils are usually the predominant cell type (86%), but the inflammation may be less marked than in cats with periosteal proliferative polyarthritis.18,19,56 Synovial biopsy reveals chronic synovitis and villous hypertrophy of the synovial membrane, with dense lymphoid and plasma cell infiltrates destroying articular cartilage.
Radiographically, rheumatoid-like arthritis is characterized by severe subchondral central and marginal erosions, and periarticular soft tissue swelling.7,9,17 –19 Advanced cases may show extensive bone destruction with gross joint deformities (Figure 7).18,19 Periosteal new bone formation is minimal. Calcification of the soft tissues around the joint may be seen.18,19 Rheumatoid-like arthritis should be suspected in any cat with erosive, deforming polyarthritis once infectious causes have been eliminated and a treatment trial with doxycycline has been ineffective.

Radiographs of both carpal and hock joints of a cat with rheumatoid-like arthritis. (a) Craniocaudal view of the right carpus. There is extensive destruction of the carpal and proximal metacarpal bones. (b) Craniocaudal view of the left carpus. There is extensive destruction of the carpal and proximal metacarpal bones; in addition discrete ‘punched out’ erosions can be seen within some of the bones. (c) Mediolateral view of the right hock. There is extensive destruction of the distal tibia and tibial tarsal bone. (d) Mediolateral view of the left hock. There is destruction of bone, soft tissue mineralization and subluxation of the joint. Reproduced, with permission, from Bennett D. Immune mediated and infective arthritis. In: Ettinger SJ and Feldman EC (eds). Textbook of veterinary internal medicine. 7th ed. Elsevier, 2010
Rheumatoid-like arthritis is commonly associated with the presence of circulating autoantibodies directed against immunoglobulin G, known as rheumatoid factor (RF). Tests for RF in cats are not commercially available but modifications of the canine Rose-Waaler or ELISA tests have been used to measure RF in cats.18,19,56 A positive RF test is not essential or sufficient for diagnosis, but results have been positive in most reports in the literature of cats with rheumatoid-like arthritis.18,56
Rheumatoid-like arthritis is an aggressive, destructive and irreversible disease if early disease-modifying therapy is not administered. Most cats have only a minimal response to treatment with non-steroidal anti-inflammatory drugs or glucocorticoids. One report of treatment with methotrexate in combination with leflunomide resulted in marked clinical improvement in 58% of cats, with no serious toxicity. 56 Treatment with other potent immunosuppressive agents known to be safe in cats could also be considered (Table 4). Most cats with rheumatoid-like arthritis also require analgesic medications (Table 3), but keep in mind that NSAIDs and glucocorticoids should never been administered concurrently.
Key Points
With the exception of osteoarthritis, which is common in cats, other causes of feline joint disease are rare to very rare.
Polyarthritis is more likely to be infectious than immune mediated in cats.
Polyarthritis secondary to calicivirus infection should be suspected in a cat with lameness and concurrent oral or respiratory symptoms. Calicivirus polyarthritis is most often seen in kittens following their first vaccination with a modified-live virus vaccine.
Synovial fluid culture for Mycoplasma species should always be requested in a cat with erosive or non-erosive monoarthritis or polyarthritis.
Lameness and fever responsive to doxycycline have been reported in cats with Ehrlichia-like infection and anaplasmosis.
Idiopathic or primary immune-mediated non-erosive polyarthritis is very rare in cats – an infectious cause or a reason for secondary reactive polyarthritis should always be sought before initiating immunosuppressive treatment.
An unusual immune-mediated polyarthritis causing periosteal proliferation is recognized in cats.
Rheumatoid-like polyarthritis causing subchondral erosions and joint deformities has been reported in cats. Recent information suggests that aggressive immunosuppressive treatment may be effective.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors declare that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.