
Abstract
Practical relevance:
Pancreatitis is a frequent finding in cats, the chronic form being more common than the acute form. Despite the large number of diseases or conditions that may be associated with feline pancreatitis, in most cases no cause is diagnosed and the pancreatitis is said to be idiopathic. The chronic form can be mild and asymptomatic, and has a high prevalence in apparently healthy cats. This has generated debate concerning the clinical significance of chronic feline pancreatitis. However, several reports have demonstrated the severity of clinical signs in certain forms of acute feline pancreatitis, while other studies have reported a strong association between chronic pancreatitis and the development of comorbidities such as hepatic lipidosis, diabetes mellitus, inflammatory bowel disease or exocrine pancreatic insufficiency. This suggests that feline pancreatitis should not be overlooked.
Clinical challenges:
Diagnosis of feline pancreatitis is complicated by the non-specific clinical signs and poor diagnostic value of basic biochemistry and haematology or imaging techniques. Development of a feline-specific pancreatic lipase immunoassay has improved our diagnostic ability in the past decade, but may have more limited application for mild and chronic forms of pancreatitis. Moreover, histopathology (the ‘gold standard’ diagnostic test) can be associated with false-negative results due to multifocal distribution of lesions or mild forms of the disease. With respect to treatment, it is important to take into account the idiosyncrasies of the feline species when considering medical therapies.
Evidence base:
This article reviews the literature on feline pancreatitis, focusing on the different forms and their relative clinical significance, while explaining difficulties inherent in the diagnosis of this disease. An overview of current recommendations for the management of cats with pancreatitis is also provided.
Feline pancreatitis has been recognised for more than 40 years.1,2 Despite marked improvement in our understanding of the disease, and development of more sensitive and specific diagnostic tools, many questions on the pathophysiology of feline pancreatitis remain unanswered. This article sets out to review current knowledge on the aetiology, diagnosis and treatment of feline pancreatitis, and to determine the clinical significance of this particularly challenging disease.
What are the different forms of pancreatitis in cats?
Pancreatitis is an inflammatory disease of the exocrine pancreatic tissue and can be divided into acute and chronic types based on histological findings.3,4 Until recently, pathological classification of feline pancreatitis was based on the human classification system. 5 In 2007, the histopathological characteristics of feline pancreatitis, were reviewed and a scoring system was designed to grade the severity of pancreatitis. 6 Two main forms of feline pancreatitis have been described. Acute pancreatitis (AP) is characterised by neutrophilic inflammation and varying amounts of pancreatic acinar cell and peripancreatic fat necrosis (Figure 1). 6 Chronic non-suppurative pancreatitis. (CP) is characterised by lymphocytic inflammation, fibrosis and acinar atrophy (Figure 2). 6
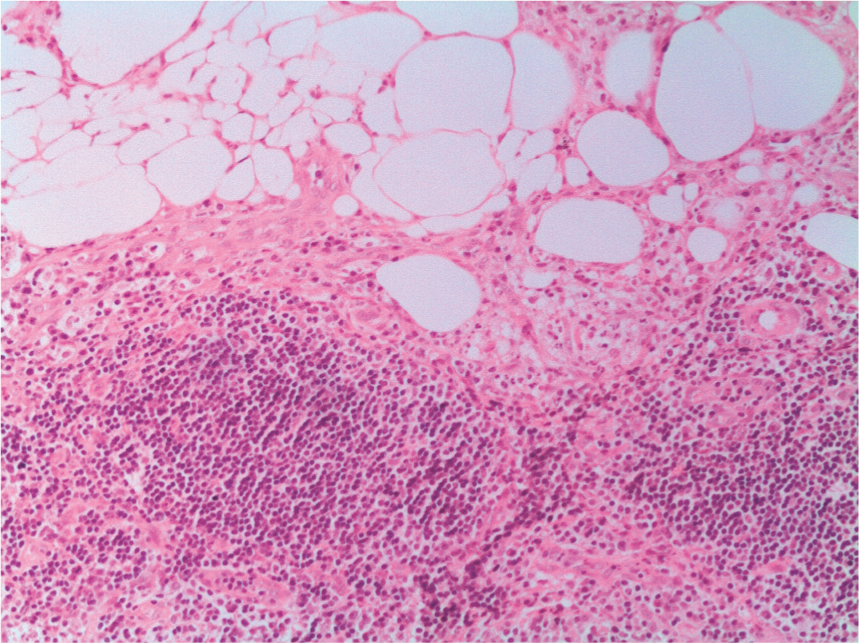
Histological section of the pancreas of a cat with acute pancreatitis. Note the intense peripheral fat necrosis and infiltration by mononuclear cells. Haematoxylin and eosin (H&E) x 40
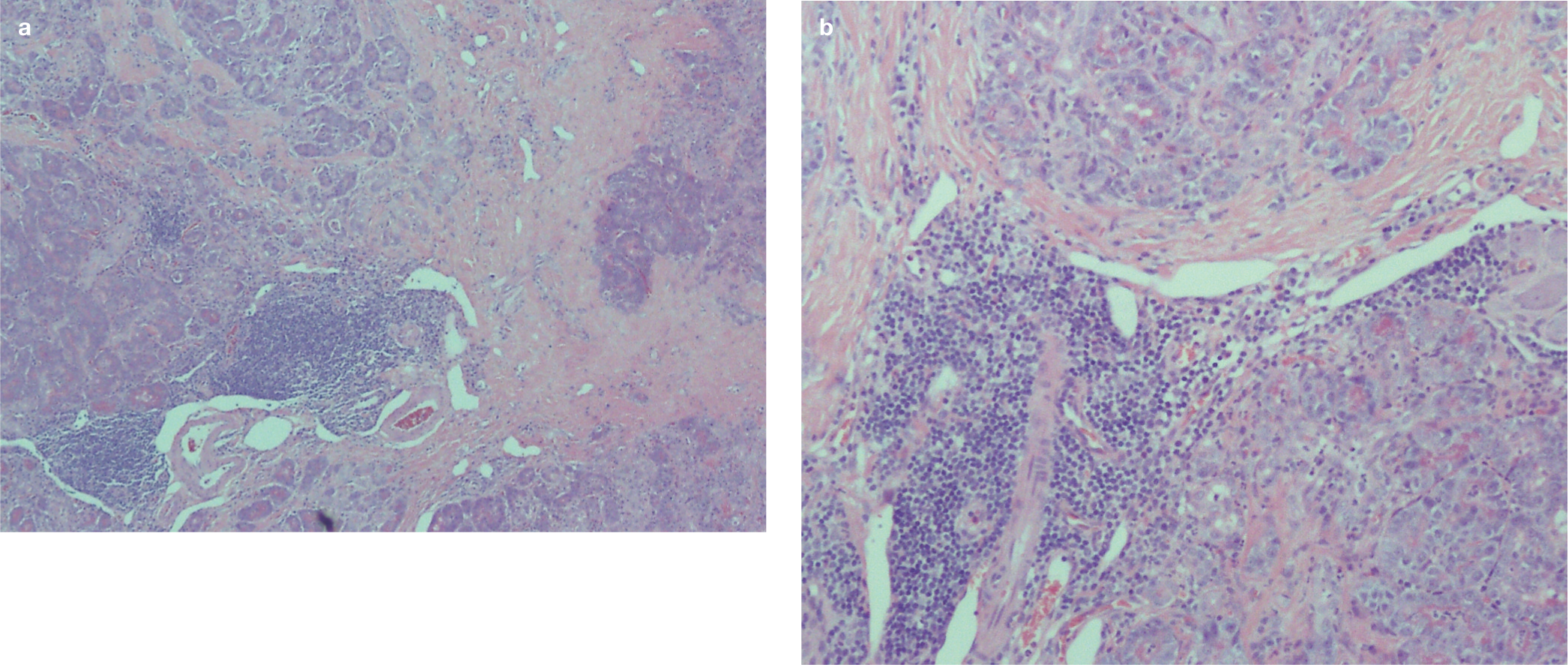
Histological sections of the pancreas of a cat with chronic pancreatitis, at x 10 (a) and x 40 (b) magnification. Note the extensive fibrous tissue (pale pink) surrounding and disrupting darker pink acinar tissue and clumps of lymphoplasmacytic inflammation (dark purple) at the top and bottom of section (a). H&E

Frequently nausea is not obvious in cats, but can be associated with hypersalivation or anorexia
An earlier study divided AP into two forms: ‘acute necrotising’, where there was significant fat necrosis, and ‘acute suppurative’, where fat necrosis was not a significant feature. 7 The authors of that study also included some cases with concurrent interstitial fibrosis and lymphocytes and plasma cells (findings that are consistent with more chronic changes) in the acute necrotising group. 7 This demonstrates that, unfortunately, there is some overlap between AP and CP histologically and it has been suggested that these represent different points on a disease continuum. 8
Why is feline pancreatitis so overlooked?
Diagnosing feline pancreatitis ante mortem remains a challenge for the clinician.9,13 This difficulty has multiple origins which include the undefined aetiology, often mild and nonspecific clinical signs, poor sensitivity and specificity of most of the imaging or clinicopathological findings, frequent concomitant disorders and difficulty in obtaining or interpreting biopsy samples.
Aetiology- what do we know?
Little is known about the aetiology of pancreatitis in cats. Experimental studies, when cats were used as a model for human disease, revealed that total or partial obstruction of the pancreatic duct was associated with development of chronic changes in the pancreas.14,15 Though naturally occurring AP associated with obstruction of the pancreatic duct, either by an intraluminal mass, pancreatolith or cholelith blocking the common duct near the sphincter of Oddi or by extraluminal compression, has occasionally been described in clinical cases,16–18 this does not appear to be a common cause of pancreatic inflammation in cats.3,7
Several studies have shown a strong association between pancreatitis, inflammatory bowel disease (IBD) and cholangitis in cats, and the association of concomitant inflammatory diseases in the liver, pancreas and intestine has given rise to the term ‘triaditis’.7,19,20 The pathogenesis underlying this association is not clear but may be explained partially by the common insertion of the common bile duct and the major pancreatic duct into the duodenal papilla. 4 It is theorised that this close anatomical proximity may favour reflux of bile or luminal contents, including bacteria, into the pancreatic ducts. When feline pancreases affected by acute or chronic pancreatitis were evaluated by fluorescence in situ hybridisation, bacteria were detected in 35% of the organs, mainly in periductal areas or glandular parenchyma. 21 Streptococcus species and Escherichia coli were most frequently found, which supports the suspicion of enteric bacterial translocation. Vomiting, a clinical sign commonly observed in cats with IBD or cholangitis, may raise the intraluminal pressure and further increase the risk of pancreaticobiliary reflux. 4 It is also possible that all three organs may be affected by a similar immune-mediated disease process, such as occurs in some human diseases.22,23
This concept of triaditis, and particularly the association between cholangitis and pancreatitis, has recently been challenged. 24 While accepting that triaditis was probably common in a subset of cats with severe liver disease, particularly those with neutrophilic cholangitis, it has been suggested that cholangitis is otherwise rarely associated with pancreatitis and IBD. 24 The strong association between chronic pancreatitis and IBD was not contested, however. 24
Ischaemia is another recognised cause of acute pancreatitis in cats. 25 This is particularly significant during surgery when inadvertent compression or ligature of the pancreatic vessels can compromise pancreatic blood flow. 1 Similarly, hypotensive episodes during anaesthesia can induce ischaemic insults to the pancreas. This seems to be an uncommon postoperative complication when the principles of appropriate surgical technique and careful anaesthetic monitoring are respected.26,27

Pancreatic ischaemia is also a consequence of pancreatitis itself. Inflammation, oedema or fibrosis can increase pancreatic interstitial and ductal pressure and lead to compromised pancreatic blood flow and further pancreatic inflammation.28,29 This vicious cycle helps to explain how CP can become progressive.
Other rare proposed aetiologies for feline pancreatitis include specific infectious agents (Toxoplasma gondii, feline herpesvirus 1, feline infectious peritonitis virus, calicivirus, pancreatic and liver flukes), organophosphate poisoning, lipodystrophy, acute hypercalcaemia, idiosyncratic drug reactions and nutritional causes.3,4,6,30
In the majority of feline patients, despite thorough investigations, no obvious cause of pancreatitis is diagnosed and the disease is considered to be idiopathic.3,7,9 This may partly explain the relatively low degree of clinical suspicion that exists for feline pancreatitis in many cases.
Laboratory findings – are there any specific clinicopathological markers?
Normocytic, normochromic, regenerative or non-regenerative anaemia is a frequent observation in cats with AP, occurring in 26–55% of cases, although it may only become apparent after correction of dehydration.4,7,8 Leukocytosis is less commonly noted than in dogs, seen in around 46% of cases.4,7,8 Leukopenia can be observed and may be associated with a poorer prognosis. 4 Haematological findings were not significantly different between CP and AP and between AP and acute suppurative pancreatitis in two studies in cats, and remain non-specific.7,8
Biochemistry changes are frequently observed but may reflect the presence of concurrent disease and, again, are not specific for pancreatitis. High activities of alanine aminotransferase (24–68%) and alkaline phosphatase (50%) have been described.4,7,8 Elevation of liver enzyme activity was more pronounced in cats with CP than AP in one study, suggesting this may represent the effect of concomitant hepatobiliary inflammatory disease. 8 Hyperglycaemia is a common abnormality (10–64%) and is observed in both AP and CP; hypoglycaemia is more frequently found in cats with AP.4,7,8 Ionised hypocalcaemia has been reported particularly frequently in cats with AP (32–61% of cases), and was associated with a poorer outcome in several studies.4,7,8,31 Hypokalaemia was also commonly found in one study, affecting 56% of patients. 7 As with haematology, biochemistry results do not appear to be significantly different between patients with CP and AP.
The clinical value of specific pancreatic function tests is more variable in cats than in other species, including humans and dogs. Lipase and amylase activities have classically been considered to be of limited value in cats, being extremely insensitive and showing non-specific increases associated with liver, renal or other gastrointestinal diseases.2,3,7,12,13 However, moderate to good sensitivity and specificity of lipase has been reported for the diagnosis of feline pancreatitis using the 1,2- o-dilauryl-rac-glycero-3- glutaric acid-(6’-methylresorufin) ester (or DGGR-lipase) catalytic assay, when compared with histology as the gold standard. 31 A cut-off value of 26 IU/l had a sensitivity of 100% for diagnosing AP but only 48% for CP, and a specificity of 63%. This test had a high agreement with the value of Spec fPL, and sensitivity and specificity of Spec fPL were not significantly different from the sensitivity and specificity of DGGR-lipase. 32
Serum feline trypsin-like immunoreactivity (fTLI) is a species-specific immunoassay that has been developed to assess pancreatic function in cats. However, a range of studies have reported a relatively low sensitivity of the assay for the diagnosis of feline pancreatitis.13,33–35 In one study, the sensitivity of fTLI was increased to 86% when the cut-off was decreased from 100 µg/l to 49 µg/l, although this probably also reduced the specificity, which was not calculated in the study. 34
A species-specific immunoassay to detect pancreatic lipase (feline pancreatic lipase immunoreactivity or fPLI) has been developed in the hope that this will be more useful than lipase, amylase or fTLI. 36 There are currently two different tests commercially available for the measurement of fPLI, both from the same laboratory: Spec fPL and Snap fPL (Idexx). Both tests are a monoclonal sandwich enzyme-linked immunosorbent assay (ELISA). Spec fPL is a quantitative test, for which concentrations >5.3 µg/l are consistent with pancreatitis and concentrations between 3.5 and 5.3 µg/l are in a grey zone. Snap fPL, now available in veterinary practices, is a semi-quantitative test. A positive Snap fPL test result indicates a fPLI value >3.5 µg/l and does not differentiate patients in the grey zone from patients with values of fPLI considered consistent with pancreatitis. A positive Snap fPL result must, therefore, be further confirmed by a Spec fPL assay.
There is still a paucity of studies evaluating the value of Spec fPL in the diagnosis of feline pancreatitis.32,35,37 In the only clinical study in which the diagnosis of pancreatitis was based on histopathology, fPLI appears to be the most sensitive test, compared with fTLI or computed tomography (CT), with a sensitivity of 100% for moderate or severe pancreatitis. 35 The sensitivity was much lower for mild pancreatitis, at 54%, with an overall sensitivity for all cases (mild, moderate and severe) of 67%, which was still higher than other tests. 35 However, histopathology was only performed when deemed possible by the clinician, introducing some bias in the recruitment of patients. In the same study, specificity when evaluating eight healthy cats was 100%. 35 The number of healthy cats was low in this study and when three cats with a normal pancreas but signs consistent with pancreatitis were evaluated the specificity dropped to 67%. 35
Obviously, more studies with higher numbers of healthy cats, or cats with other gastrointestinal diseases, are needed to properly evaluate the sensitivity and specificity of fPLI, but it does appear to be one of the most sensitive and specific blood tests for feline pancreatitis currently available. All these diagnostic values relate to Spec fPL. To date, Snap fPL has not been validated by independent studies, although validation studies have been performed by the manufacturer. Moreover, lesions such as fibrosis or atrophy are not expected to induce increases in fPLI levels. 37 This would suggest that the sensitivity of fPLI in diagnosing CP without an active component is low, and may explain the lower sensitivity for mild pancreatitis.35,37
Despite, therefore, being the most powerful non-invasive test for the diagnosis of feline pancreatitis that is currently available, it is important to remember that fPLI is not 100% sensitive and specific, especially for mild and/or chronic forms of pancreatitis, and that more studies are needed to strengthen the evaluation of its efficacy. 38
Imaging-is it any help?
Abdominal radiographs may reveal a cranial loss of serosal detail and/or a mass effect. However, radiography is both insensitive and non-specific for the diagnosis of feline pancreatitis and is mainly recommended to rule out concomitant diseases such as intestinal obstruction.7,8,13,34
Ultrasonographic findings that suggest AP in dogs, such as a hypoechoic pancreas, hyperechoic mesentery and abdominal effusion, are also relatively specific for pancreatitis in cats (Figure 4), although other pancreatic lesions (eg, neoplasia, hyperplastic nodules) may share a similar appearance with pancreatitis.35,39 Ultrasound findings are relatively specific in differentiating pancreatitis from other gastrointestinal diseases, but ultrasound lacks specificity to differentiate between AP and CP; indeed, there is considerable overlap in ultrasound findings between the two forms of the disease. 8 It is important to recognise that some changes detected during abdominal ultrasonography may be age related, like pancreatic duct dilation, previously thought to be a specific sign for pancreatitis (Figure 5). 39

Ultrasonographic findings in a cat with acute pancreatitis. Note the heterogeneous pancreatic parenchyma and surrounding hyperechoic mesentery (arrows). Courtesy of diagnostic imaging department, Queen’s Veterinary School Hospital, University of Cambridge, UK

In cats, abdominal ultrasound carries a low sensitivity (11–35%) for pancreatitis,8,33,34,40 although one study reported a 67% sensitivity in moderate to severe pancreatitis, with a lower sensitivity in the mildest forms of disease. 35 The sensitivity of abdominal ultrasound is further influenced by difficulties in detecting the pancreas in some patients, and is dependent on operator experience.33,40 The use of endosonography (endoscopic ultrasound) may improve general visualisation of the feline pancreas, but in one study did not alter the diagnosis of pancreatitis when compared with transcutaneous abdominal ultrasound despite improving general visualisation. 41
Despite the above-mentioned limitations, abdominal ultrasonography is recommended in any suspected case of feline pancreatitis, as it may be useful to diagnose associated pancreatic masses (eg, pseudocysts, tumours or abscesses), and pancreatic or biliary stones, and will allow fine-needle aspiration of lesions.12,40
The use of CT in the diagnosis of feline pancreatitis has been evaluated in two clinical studies,34,35 which revealed a similarly low sensitivity of 20%. CT is thus not recommended as a diagnostic aid for feline pancreatitis.34,35 Magnetic resonance cholangiopancreatography (MRCP) is becoming the imaging modality of choice in humans for the pancreatic and biliary tract, and a recent study in cats suggested that magnetic resonance imaging and MRCP may also be helpful in cats with pancreatitis. 42
History–an ideal gold standard?
The gold standard for ante-mortem diagnosis of pancreatitis in cats remains histopathological analysis of pancreatic biopsies,3,6,8,35 despite most authors agreeing that histopathology is not perfect for evaluating the presence of feline pancreatitis. Pancreatic biopsy is often complicated by the sensitivity of the pancreas to hypoxaemia, whether induced by hypotension during anaesthesia or by pancreatic blood flow impairment following manipulations of other organs during surgery. Moreover, most cats with severe pancreatitis are poor candidates for anaesthesia.4,38 Even for patients stable enough to undergo anaesthesia and pancreatic biopsy, or improving on supportive treatment, pancreatic biopsy may not be recommended as the results rarely alter patient management in these cases.
Pancreatic biopsy should be considered if laparotomy or laparoscopy are being performed for other reasons. 38 The trauma induced by performing pancreatic biopsy is not, in itself, considered to increase the risk of pancreatitis, so clinicians should not be reluctant to collect pancreatic biopsies at laparotomy provided they are careful and do not disrupt the blood supply. Gross lesions associated with AP include oedema, hyperaemic or haemorrhagic parenchyma (Figure 6) and signs of focal peritonitis. CP is usually associated with fewer changes, although severe areas of fibrotic tissue and adhesions to the small intestine may be observed.

Intraoperative view of a cat with severe acute pancreatitis. Note the areas of haemorrhagic parenchyma, and overall swollen and oedematous appearance of the pancreas. Courtesy of Jane Ladlow, Queen’s Veterinary School Hospital, University of Cambridge, UK
Histological accuracy is limited by frequent multifocal distribution of lesions in cats with AP or CP.6,7,40 In a study comparing the presence of pancreatitis lesions in the left limb, the right limb and the body of the pancreas, only half of the cats diagnosed with pancreatitis had lesions identified in every section. 6
Multiple biopsies are, therefore, recommended to reach a definitive diagnosis and pancreatitis cannot be completely excluded on the basis of a negative biopsy result.4,38
Lesions observed during CP are frequently mild in severity and it is suspected that histopathology may be relatively insensitive for diagnosing mild lesions. 6 Conversely, mild forms of CP were frequently found in asymptomatic patients in one study. 6 The finding of mild signs of inflammation on pan-creatic biopsy can be a diagnostic challenge, therefore, as these lesions may represent ongoing pancreatitis but may not necessarily explain the patient’s clinical signs.
Until recently there was no detailed description of the histological assessment of feline pancreatitis. The above-mentioned study has proposed criteria for diagnosing AP and CP histologically and for scoring the severity of lesions. 6 This represents the first histological classification of natural feline clinical pancreatitis. However, previous studies have been characterised by a marked variation in the description of the lesions and the severity of AP and CP, making histology less than ideal as a gold standard.

What is the clinical significance of feline pancreatitis?
The significance of the clinical signs in acutely and severely ill feline patients diagnosed with pancreatitis cannot be denied.3,4,7,8,12,38 Some of these cats will present with severe clinical syndromes like cardiovascular shock, disseminated intravascular coagulation, pulmonary thromboembolism and multi-organ failure.3,38 But these severe presentations are rare and the most frequent type of feline pancreatitis diagnosed in practice is a mild form of CP. Given the high numbers of asymptomatic cats with histological evidence of mild pancreatitis, 6 the clinical significance of finding mild pancreatitis on histological sections has to be questioned. It is possible that mild pancreatitis is not pathological in some patients, or may represent a response of the pancreas to concurrent disease.
However, there is now growing evidence that pancreatitis can be associated with other concurrent diseases, such as cholangitis and IBD, as discussed earlier. Hepatic lipidosis has also frequently been associated with feline pancreatitis.8,43,44 This is not surprising considering that anorexia and weight loss are a typical feature of feline pancreatitis. The reported prevalence of pancreatitis lesions in cats with hepatic lipidosis varies from study to study from 5–38%.43,44 In one study comparing AP and CP, concomitant hepatic lipidosis was found to be more frequent in association with CP (30% prevalence) than AP (9%). 8 These values, based on retrospective studies, likely underestimate the true prevalence of the association between feline pancreatitis and hepatic lipidosis. It is worth noting, too, that the presence of AP is considered a poor prognostic factor in a patient with hepatic lipidosis. 43
The high frequency of pancreatitis in feline patients with diabetes mellitus (DM) has been emphasised in several studies.8,12,45,46 There is likely to be a complex cause-and-effect relationship between DM and pancreatitis in cats, as there is in dogs and humans. DM can predispose to pancreatitis; conversely end-stage CP can lead to the development of DM by loss of islet cells, and these cases may additionally develop concurrent exocrine deficiency. 45 A study investigating the prevalence of pancreatitis in cats with DM found that fPLI was commonly elevated, suggesting that acute episodes of pancreatic inflammation were relatively frequent in diabetic cats. 46 Feline pancreatitis is also commonly found in cats with diabetic ketoacidosis, and some authors have suggested that pancreatitis may play a role in the development of ketoacidosis by decreasing sensitivity to insulin,45,47 although fPLI was not associated with response to insulin in one study. 46 It is recommended that clinicians look for pancreatitis when investigating insulin resistance in a diabetic cat.
End-stage CP with loss of acinar tissue is believed to be the main cause of exocrine pancreatic insufficiency (EPI) in cats.3,4,9,48 At the time of diagnosis of EPI, pancreatic histology predominantly shows fibrosis with loss of pancreatic acinar tissue and minimal inflammation (the pancreatic equivalent of a cirrhotic liver). 48 In one case series of 16 cats with EPI, no cat was clinically suspected of pancreatitis prior to diagnosis of EPI. Pancreatic histopathology was performed in two cats, with findings reported as ‘pancreatic atrophy’, although the authors did not clarify whether this was associated with extensive fibrosis typical of end-stage CP. 49 In this case series, EPI was diagnosed on the basis of low serum fTLI in all the cats in which it was measured, together with compatible clinical signs (weight loss and diarrhoea). Serum cobalamin was low in all the cats tested, 49 which is to be expected in EPI in this species because cats make all of their intrinsic factor required for ileal absorption of cobalamin in their pancreas. It is, therefore, important to consider a possible diagnosis of EPI in a cat with unexplained weight loss, with or without concurrent DM, and consider measuring both fTLI and cobalamin in these cases.
Treatment recommendations
Most of the recommendations for the treatment of feline pancreatitis are based on extrapolations from human studies or experimentally induced feline pancreatitis. Evidence is, therefore, lacking and prospective studies evaluating the effect of different aspects of treatmenton on spontaneous disease are needed.
The general recommendations are centred on three main aspects of management: nutrition and antiemetic treatment, correction of fluid and electrolyte imbalances, and analgesia.3,4,9,37
Nutrition and antiemesis
It haslong been recommended that food is withheld for 24–48 h in patients with pancreatitis, but this dogma has recently been challenged in both human and canine patients.50–52 Vomiting is not a common feature in cats, which are often presented with a history of anorexia of several days’ duration and commonly show evidence of concomitant hepatic lipidosis. Starvation can, therefore, be detrimental in feline patients, and it is now accepted that feeding should be instigated as soon as possible.4,53
There is currently no evidence that a low fat diet is beneficial in cats with pancreatitis. Due to the peculiarities of feline metabolism, it is generally suggested that affected cats are fed a diet that is low in carbohydrate, high in protein and contains a moderate amount of fat in order to avoid the development of malnutrition and hepatic lipidosis.9,53 Nutrition should be re introduced gradually over a few days to avoid refeeding syndrome. 53
It is extremely important to recognise and treat nausea in cats, as it can severely reduce food intake.4,54 Signs of nausea in cats include vomiting or hypersalivation (see Figure 3), but can also be poorly specific; anorexia, for example, may be the only reported sign. Antinausea medications (Table 1) are therefore indicated in all cats with suspected pancreatitis, whether or not vomiting is present. Metoclopramide is considered to be poorly effective in the feline species but may be more effective when given as a constant rate infusion, and may be more useful in cases that have functional ileus due to its prokinetic effects. 54 It may interfere with splanchnic perfusion via its dopamine antagonist action and with sphincter of Oddi activity via its cholinergic effect, although the significance of these effects has not been investigated clinically.55,56
Drugs used to treat pancreatitis in cats

IV = intravenously, SC = subcutaneously, IM = intramuscularly, PO = orally, CRI = constant rate infusion
Nausea is more reliably controlled in cats with pancreatitis by NK1 receptor antagonist (maropitant) or 5HT3 antagonist (ondansetron, 3 dolasetron) agents. 54 There is also evidence that maropitant has a beneficial effect in reducing visceral pain in cats, which further supports its use in feline pancreatitis. 57
If voluntary food intake is not restored rapidly, it may be necessary to place a feeding tube to allow energy requirements to be met. Naso-oesophageal, oesophagostomy and gastrostomy tubes (Figure 7) are used most frequently in patients with AP. 53 Use of a gastrojejunostomy tube, placed either surgically or endoscopically, has also been described. 58 It is unclear if bypassing the pancreas is beneficial in cats. Pre-pyloric feeding has been shown to be safe in humans and dogs, and may also be in cats. In the acute stages of pancreatitis, the cat may be too unstable to have a general anaesthetic for placement of a feeding tube, particularly if there is concurrent hepatic lipidosis. In these circumstances, placement of a naso-oesophageal feeding tube for a few days will allow stabilisation prior to placement of a more secure tube.

Gastrostomy feeding tubes allow administration of appropriate volumes of food and can be used for medication administration
Convalescence liquid veterinary diets can be used with naso-oesophageal tubes, while a semi-solid diet should be reserved for larger tubes (oesophagostomy and gastrostomy tubes) (Table 2). Convalescence diets are energy-dense and have a high protein content, which makes them appropriate for hospitalised feline pancreatitis patients, despite their high fat content. In the case of severe malnutrition and persistent anorexia, total or partial parenteral nutrition may be considered, although studies in humans support combining this with at least some enteral nutrition, where possible, to maintain gut wall barrier function. 53 , 59
Examples of commercially available convalescence veterinary diets that can be used with a feeding tube

DM = dry matter

Correction of eletiolyte imbalances
Vomiting, anorexia and diarrhoea canlead to severe dehydration and electrolyte imbalances in cats with pancreatitis.3,4 Aggressive intravenous fluid therapy is required to avoid the further deleterious effects of decreased pancreatic perfusion. Hypokalaemia and hypocalcaemia are not uncommon and must be treated, as their presence is associated with a poorer prognosis.4,31
Analgesia
Pain is a common feature of feline pancreatitis but is classically difficult to evaluate in this species. 60 Opioids are the recommended first-line drugs for treating abdominal pain associated with pancreatitis.3,60 Morphine has been associated with increased sphincter of Oddi activity and its use in AP has previously been questioned. However, recent human metaanalysis failed to show increased adverse effects when treating human pancreatitis patients with opioids, while the need for supplementary analgesia was decreased, supporting their use for the management of pancreatitis. 61 Buprenorphine, butorphanol and methadone are the drugs most often used (see Table 1).
In cases of intractable pain, fentanyl injection or patches, or ketamine and lidocaine constant rate infusions can be considered. 60 For management of chronic pain, sublingual buprenorphine or tramadol can be safe, although potentially less potent, alternatives.60,62
Other treatments
Other treatments that may be considered for cats with pancreatitis, in addition to the above mainstay treatments, are discussed on page 403.
Key Points
Pancreatitis in cats is increasingly recognized by veterinarians, but remains frequently overlooked.
In cats, AP is less prevalent than CP but the two presentations share similar clinical signs and diagnostic findings.
Despite increased awareness of the disease, suspecting and confirming feline pancreatitis is a challenge in the clinical setting. Lack of sensitivity or specificity of the available diagnostic tools, especially for CP, and the frequency of asymptomatic disease have led to the false idea that pancreatitis may not be clinically relevant.
In the light of its association with other diseases, including hepatic lipidosis, cholangitis, IBD, diabetes mellitus and EPI, it is important that clinicians maintain a high index of suspicion for pancreatitis, and investigate accordingly.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.