
Abstract
Practical relevance:
Definitive diagnosis of disease involving the parenchymal abdominal viscera often requires a representative specimen of affected tissue. Methods used to obtain tissue samples range from those that are minimally invasive, such as fine-needle aspiration (FNA), to more invasive techniques such as surgical biopsy.
Clinical challenges:
FNA and cytological examination can be a useful diagnostic tool and is commonly used for hepatic, splenic and lymph node specimens. FNA is an easy and cheap procedure that is best suited to diffuse disease and can be performed at low risk to the patient. However, its accuracy and agreement with the histopathological findings vary depending on the underlying disease and it often fails to provide information on parenchymal architecture. Importantly, FNA for cytological examination of the liver has serious limitations when used to identify the primary disease process due to the small sample size obtained.
Audience:
This review is aimed at clinicians undertaking more detailed and specialist investigation of diseases of feline parenchymal abdominal organs and provides practical guidance on the different methods used to obtain hepatic, renal, pancreatic and splenic specimens in cats.
Evidence base:
The information presented is based on peer-reviewed publications and the clinical experience of the author.
Why biopsy?
The accuracy of cytological examination as a diagnostic tool has been evaluated in the veterinary literature and disagreement between cytological findings and histopathological examination has been reported on many occasions. In a study of cats and dogs presented with hepatic disease, Wang et al showed that overall agreement between the histopathological and cytological diagnosis was found in only 51.2% of the 41 feline cases. 1 Another study of cats with infiltrative liver disease highlighted the risk of a misdiagnosis of hepatic lipidosis, based on the presence of concurrent vacuolar changes. 2
Definitive diagnosis of disease involving an organ often requires a representative specimen of the affected tissue. Tissue sampling of feline abdominal organs can be carried out using core needle biopsy instruments through a percutaneous ultrasound-guided, laparoscopic or open surgical approach.
General considerations before biopsy

In order to verify patient suitability and that there are no contraindications to biopsy, a thorough physical examination, blood pressure assessment, complete blood count and biochemical profile, urinalysis, coagulation profile, and thoracic and abdominal imaging are always recommended (see box on page 216).
Biopsy of the liver
Liver biopsy is an important step in the evaluation of cats with hepatic disease. It permits formulation of a diagnosis and treatment plan, and an accurate prognosis. However, a single liver specimen evaluates only a small portion of hepatic tissue and may not represent the entire liver. Therefore, when possible, samples from multiple lobes are preferred, even when the parenchyma appears uniform.
In preparation for biopsy it is important to evaluate the liver, biliary tract and portal vein with ultrasonography, and to assess the patient’s coagulation status (see box below). 6 In a large retrospective study involving 124 cats, Bigge et al demonstrated that those with moderate to severe thrombocytopenia (<80,000 platelets/µl) and prolonged APTT (>1.5 x normal) had a greater risk of haemorrhage from ultrasound-guided biopsy procedures. 6
Hepatic biopsies are performed percutaneously under ultrasound guidance, by laparoscopy or directly at coeliotomy. The biopsy technique selected is determined by the likelihood of the sample being accurate, the appearance of the liver on imaging, the presumptive diagnosis, the results of coagulation tests, the risks of anaesthesia and surgery, and the likelihood of postoperative complications. Technique selection should also consider liver size, the presence of ascites, whether the disease is diffuse or focal, the need for possible surgical resection and the experience of the clinician in performing the procedure.
Where there is diffuse hepatic disease, any part of the liver can be sampled. Focal lesions require selective sampling under ultrasound guidance or direct visualisation via a laparoscopic or surgical approach. Large lesions should always be sampled in the periphery because the centre may be necrotic.

Ultrasound-guided percutaneous liver biopsy
The ultrasound guidance technique has risen in popularity in companion animal medicine because it is relatively easy, minimally invasive, widely available and has been associated with a low incidence of complications. However, it has been reported that needle biopsy specimens produce findings that are very different from those produced by wedge biopsy specimens; 7 therefore, hepatic core needle biopsy must be interpreted with caution. Furthermore, the technique is contraindicated in cats with microhepatica, coagulation defects, large-volume ascites, hepatic cysts or abscesses, vascular tumours or lesions adjacent to large bile ducts or hepatic vessels. 5
The major limitation of the core biopsy technique is the small size and limited number of samples retrieved, which may erroneously be assumed to represent the entire liver. One study in humans confirmed that diagnostic accuracy of hepatic needle biopsy depended on specimen size and the number of specimens acquired: needle biopsy specimens ≥15 mm long are necessary to include the 15 portal triads required for accurate morphological characterisation of diffuse and multifocal disorders. 8 Median needle biopsy specimen length in cats is generally shorter than this minimum length recommended for diagnostic accuracy (15 mm).7,8 We can speculate that the short biopsy length in cats reflects the small size and depth of the liver lobe from which specimens are collected. Furthermore, it has been determined that a 16 gauge biopsy core needle sample typically contains only four or five portal triads without complete hepatic lobules, and that histological interpretation can be very difficult. 7 The same study reported that the difference between diagnoses derived from wedge and needle biopsy specimens most likely reflects a common inability to achieve more than four to six portal triads and, in turn, the small number of acinar units sampled and poor representation of zonal lesions. 7

These findings encourage reconsideration of the method of tissue acquisition and the overall amount of liver needed to achieve a definitive diagnosis of hepatobiliary disease in both cats and dogs.
Open surgical liver biopsy
If cats are having surgical procedures performed on the hepatobiliary tract, open surgical biopsies are obtained. It is recommended that a surgical liver biopsy is taken early during the laparotomy because hepatocellular damage can result from prolonged anaesthesia, vascular changes and manipulation of the bowel. 3 The advantages of surgery are the exposure, direct visualisation, and ability to manipulate and palpate the tissues and monitor the biopsy site for bleeding. The disadvantages are the abdominal incision and the postoperative recovery. The sample size of a surgical biopsy is the largest of any of the methods described, providing adequate tissue for histopathology and culture. 3
There are several techniques for obtaining open surgical liver tissue (see box on page 218), including suture fracture and punch biopsy.
Vasanjee et al compared the volume of haemorrhage, number of lobules and portal triads available for histological evaluation and resultant collateral damage between five hepatic biopsy methods in dogs: needle biopsy, punch biopsy, guillotine method, laparoscopic biopsy (forceps) and ultrasonic scalpel (Harmonic scalpel; Ethicon). 9 All biopsy methods produced minimal haemorrhage and, with the exception of needle biopsy, yielded adequate tissue samples for histological evaluation. A similar study has not been carried out in cats.

Laparoscopic liver biopsy
Laparoscopic liver biopsy is technically easy to perform, provides adequately sized and lesion-specific tissue samples for histopathological analysis and permits visual inspection of small lesions. 10 After the liver is explored with a palpation probe, a cup biopsy forceps is used to take samples from the edge of the liver. The forceps is opened and closed over the liver edge, holding the liver for up to 30 s; the forceps is then rotated to tear the parenchyma (preferable to linear traction) and withdrawn from the body. The biopsy site is monitored for bleeding, which in most cases is minimal. If haemorrhage is a concern, the palpation probe can be used to apply pressure, or haemostatic agents can be placed into the biopsy site. 10
For a fuller discussion of laparoscopic liver biopsy, the reader is referred to a recent two-part review article in this journal.11,12
Biopsy of the kidney
Although the general guidelines for renal biopsy are the same as for hepatic biopsy, the specific indications are fewer and renal biopsy is performed much less commonly.
Renal biopsy is typically required to refine a diagnosis, determine the severity and formulate an optimal treatment plan for cats (and dogs) with renal disease. However, there is often reluctance to pursue renal biopsy because of practitioners’ concerns over associated complications. Studies have shown that the frequency of severe complications from renal biopsy is relatively low (see later) and that renal biopsy minimally affects renal function when correct patient selection and a proper technique are employed. 4

Renal biopsy is indicated only when the results are likely to alter patient management by providing a precise histological diagnosis. Obtaining an accurate histological diagnosis may indeed be one of the more important factors in successful management of cats with: neoplasia; renal cortical (glomerular) disease, such as protein-losing nephropathy; or acute renal failure in which the underlying cause cannot be determined by less invasive methods and that is either persistently severe (ie, persistent oliguria or uraemia) or has deteriorated despite appropriate medical management. 4 By contrast, renal biopsy is unlikely to alter the prognosis, treatment and outcome in cats with chronic renal failure and, for patients with end-stage renal disease, renal biopsy is unlikely to determine the underlying cause. Moreover, an increased risk of complications in human patients with chronic renal failure has been reported. For these reasons, renal biopsy is generally not indicated in patients with chronic renal failure. 4
Abdominal ultrasound is usually performed as part of the initial evaluation of cats with renal neoplasia, acute renal failure or protein-losing nephropathy. In addition to the assessment of size, shape, contour and internal architecture of the kidneys, ultrasonography permits the identification of conditions that may make renal biopsy contraindicated (see box above). 4 Other patient factors may be associated with an increased risk of haemorrhage and include severe azotaemia, uncontrolled systemic hypertension, or administration of non-steroidal anti-inflammatory drugs within the previous 5 days. 4 In the presence of severe hydronephrosis, renal biopsy is contraindicated because of the risk of penetrating the distended renal pelvis, which is likely to be under increased pressure. Concern over inducing renal pain or perirenal tissue infection via biopsy of renal cysts and the limited diagnostic yield of a biopsy specimen that contains cysts has led to the recommendation that renal biopsy should not be performed in kidneys containing large or multiple cavities. Perirenal abscessation and pyelonephritis are additional contraindications to renal biopsy because of the risk of secondary peritonitis. Ideally, urinary tract infections should be addressed before renal biopsy. 4
Because renal vessels progressively increase in size from the surface of the kidney towards the pelvis, samples should be taken from the renal cortex, regardless of the biopsy method. To reduce haemorrhage, the large arcuate vessels in the medulla should be avoided. The renal pelvis should also be avoided, to minimise urine extravasation.13–15 Whenever possible the biopsy is taken from either the cranial or caudal kidney pole, as it is easier to stay within the cortical tissue. Both feline kidneys can be easily localised and immobilised, making both equally suitable for biopsy. 4
In general, at least five or six glomeruli are needed for adequate evaluation of the kidney. In cats, renal tissue samples can be obtained with needle biopsy instruments through a percutaneous ultrasound-guided, laparoscopic or surgical approach or by parenchymal incision during an open approach. 13
Immobilisation of the patient is very important for renal sampling, and general anaesthesia has been shown to be associated with procurement of a quality biopsy specimen. 14 Failure to immobilise the cat may increase the risk of development of serious complications after biopsy. Some extremely ill cats may be immobilised by sedatives alone, though there remains the risk of sudden abdominal movement during the procedure because of incomplete peritoneal anaesthesia.

Ultrasound-guided percutaneous renal biopsy
Blind biopsy was frequently performed in the past, but is no longer recommended, and ultrasound-guided percutaneous renal biopsy has become the modality of choice for those cats without contraindications for renal biopsy. 4 Ultrasonography identifies cortical tissue, large renal vessels and focal lesions, and guides correct placement of the needle. Moreover, it allows monitoring for post-biopsy haemorrhage. 4
Cats are placed in left lateral recumbency for biopsy of the right kidney or in right lateral recumbency for biopsy of the left kidney. The skin over the biopsy site is clipped and aseptically prepared. Sterile coupling gel is applied and a sterile sleeve is placed over the ultrasound probe. Once the site of entry is determined, a stab incision is made through the skin and the tip of the needle is guided to the renal capsule with one hand while the probe is held with the other. The biopsy needle should be aligned parallel with the external surface of the kidney, generally on the lateral aspect or across the caudal pole. The needle should be placed through the renal capsule and fired, making sure that it remains within the renal cortex (Figure 1).

Mock-up image showing renal sampling using a core biopsy needle. The biopsy is taken from either the cranial or caudal kidney pole. The needle should remain in the renal cortex and not cross the corticomedullary junction
In cats with glomerular disease, at least two quality samples should be obtained, whereas one cortical biopsy may be sufficient for a patient with acute renal failure. Digital pressure should be applied to the kidney transabdominally for approximately 5 mins after biopsy, to minimise haemorrhage. Although needle guides are available for the ultrasound probe, these are probe-specific and are not available for all probes. Moreover, a specific computer software requirement makes use of the guides rather expensive.
Unilateral ultrasound-guided renal biopsy has minimal effect on renal function in healthy cats (and dogs). The effect on renal function in diseased kidneys has not, however, been thoroughly studied. 14
Open surgical renal biopsy
Surgical biopsy is the preferred method in cats that have either isolated areas in the kidney (eg, cysts) that need to be avoided during the biopsy procedure or are undergoing exploratory surgery for other reasons (Figure 2). 4 A surgical needle biopsy can be performed (see box below) but generally a surgical wedge biopsy is preferred (see box on page 223). The wedge biopsy method allows more control over the depth of biopsy and volume of tissue collected, and is more likely to produce a good quality sample. 4

Right kidney of a cat with multifocal histiocytic nephritis visualised during exploratory open surgery
As with all surgical biopsies, the approach to wedge biopsy is via a ventral midline coeliotomy. Peritoneal and paralumbar attachments are bluntly disrupted and the kidney is elevated from the paralumbar fossa. The renal artery is identified by its pulse and digitally occluded between the thumb and forefinger if an assistant is available. Otherwise, the kidney is reflected ventromedially and the renal artery is gently occluded (for 20 mins maximum) with a vascular clamp or Rumel tourniquet. The kidney is then immobilised between the thumb and forefinger, and a wedge-shaped incision is made through the capsule and cortex with a number 11 scalpel blade. The biopsy sample is gently lifted with fine tissue forceps and the remaining tissue attachments are severed with the scalpel blade (see box above). The capsule is then closed with 4–0 monofilament absorbable suture material and pressure is applied to oppose the edges with the fingers. Including a piece of collagen sponge in the defect before closure and maintaining digital pressure for about 5 mins may help to limit haemorrhage post-biopsy. Alternatively, in the author’s experience, an ultrasonic scalpel can be used to limit parenchymal haemorrhage (Figure 3).
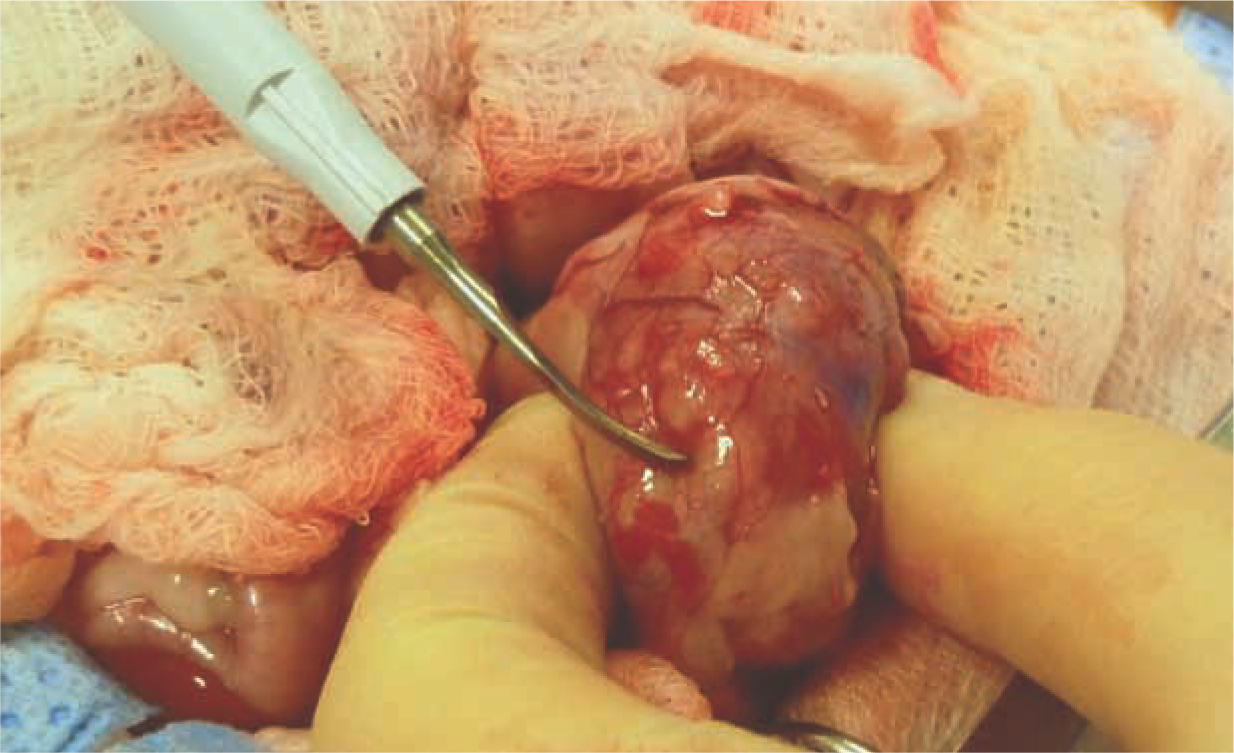
An ultrasonic scalpel (Harmonic scalpel) can be used to collect renal and hepatic biopsies and to limit haemorrhage


Laparoscopic renal biopsy
Laparoscopy enables excellent visual control over positioning of the biopsy needle and allows monitoring for post-biopsy haemorrhage. A manipulating instrument is used to position and secure the kidney, while a spring-fired core biopsy needle is placed against the renal capsule and directed tangentially prior to discharge. After biopsy, the needle is withdrawn and pressure is applied with the manipulating instrument. 15

Post-renal biopsy patient care
The cat should be kept hospitalised for at least 24 h after biopsy to enable fluid therapy and monitoring for serious haemorrhage. Intravenous isotonic fluids are recommended in the first 24 h to produce diuresis and reduce the formation of obstructing clots in the renal pelvis or ureter. The packed cell volume should be evaluated 24 h after biopsy, or earlier if concerns over ongoing bleeding arise. 4
Complications of renal biopsy
Potential complications of renal biopsy include microscopic and macroscopic haematuria, severe perirenal haemorrhage that may necessitate blood transfusion, hydronephrosis secondary to obstruction of the renal pelvis or ureter by blood clots, renal infarction and thrombosis, damage to renal vasculature, intrarenal arteriovenous fistula formation and death (see box above).4,14 In one retrospective study on renal biopsy methods and complications in dogs and cats, complications were reported in 18.5% of feline cases. 14 Severe haemorrhage was the most common complication, developing in 16.9% of all cats. Hydronephrosis and death were uncommon. Death is generally attributed to excessive haemorrhage.
Microscopic haematuria is an expected finding after renal biopsy and is generally self-limiting, resolving within 48–72 h. Gross haematuria usually resolves within 24 h. Persistence should prompt further imaging of the urinary system and evaluation of the patient’s renal function. Scar formation, linear infarcts representing needle tracts, parenchymal fibrosis and atrophy in renal tissue have been well documented and seem to be common after renal biopsy. 4 Retention cysts may also develop along needle tracts.
Biopsy of the pancreas
In contrast to pancreatitis in dogs, feline pancreatitis can be a very difficult disease to diagnose. In general, a definitive diagnosis of feline pancreatic disease requires a combination of clinical suspicion, changes on abdominal ultrasonography and histological examination of biopsies. The most reliable method for making an accurate diagnosis of pancreatic disease remains direct visualisation and histopathology. However, this method can be invasive, expensive and, in some cases, potentially dangerous if the cat is haemodynamically unstable. 16
Cases of acute feline pancreatitis are often successfully managed medically but a small number of cats may deteriorate despite conservative treatment and may require surgical intervention. Cases that have been proposed to benefit from surgery include those with bile duct obstruction, pancreatic abscesses or pancreatic masses. 17
Biopsy of the pancreas can be performed laparoscopically or through exploratory laparotomy.
Open surgical pancreatic biopsy
Diffuse pancreatic disease
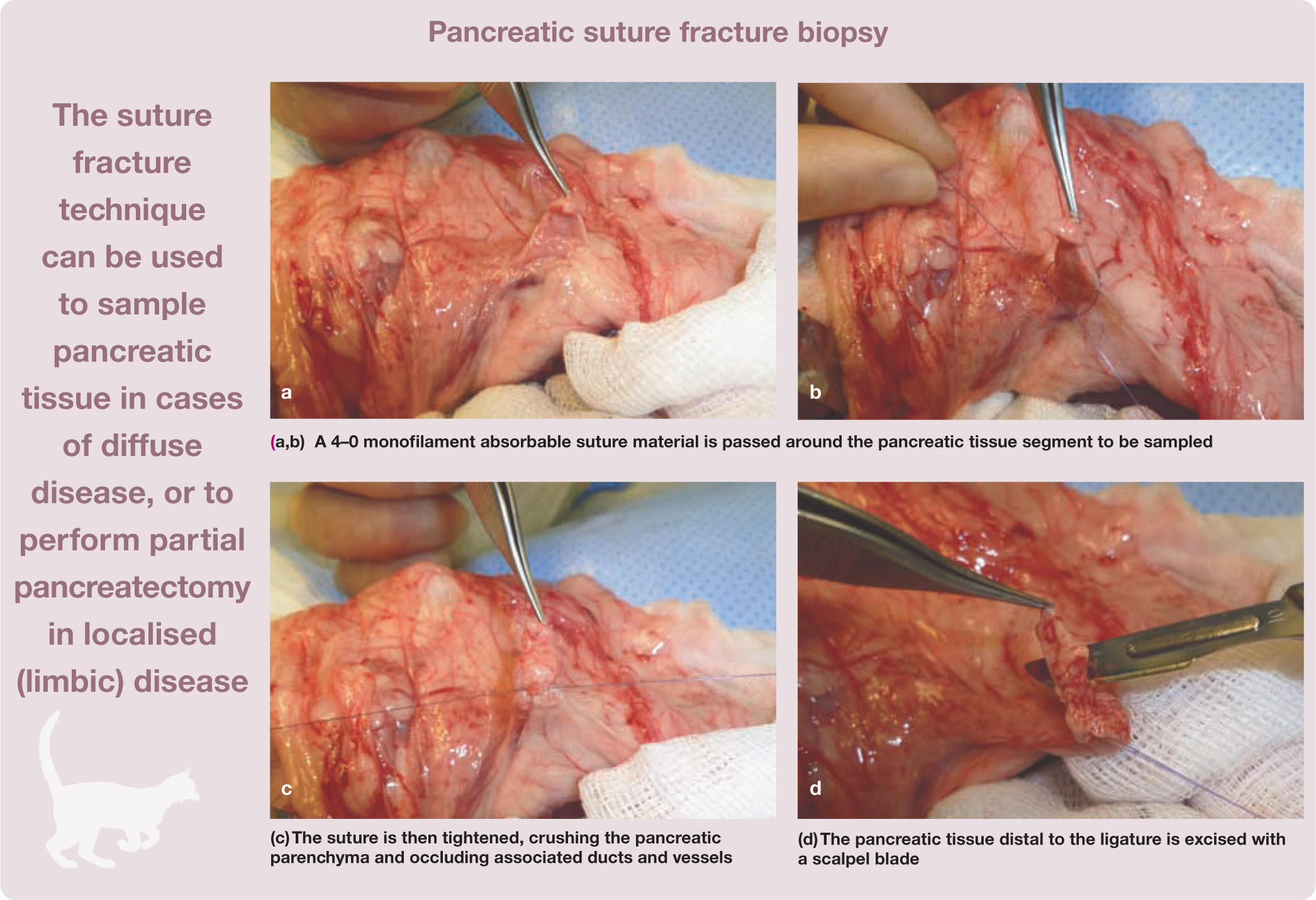
In cats with diffuse pancreatic disease, biopsy is generally performed at the distal aspect of the right limb of the pancreas due to its distance from the pancreatic duct system and major blood vessels. In cats undergoing an open surgical approach, pancreatic biopsy may be performed using a scalpel blade to obtain a wedge biopsy specimen or via a suture fracture technique.

Localised pancreatic disease
Biopsy of single or multiple localised pancreatic lesions can be excisional (partial pancreatectomy) using the suture fracture technique or wedge biopsy if positioned in the left or right pancreatic limb.
In cases in which the lesion is localised within the body of the pancreas, partial pancreatectomy cannot be performed and the biopsy may need to be collected with a core biopsy needle or a punch biopsy instrument. However, occlusion of associated ducts and vessels cannot be achieved and there may be some postoperative pancreatic enzyme leakage. A blunt dissection and ligature technique could alternatively be used. Using this method, pancreatic tissue to be removed is isolated from the remaining pancreas by blunt dissection with a Halsted mosquito hemostat or sterile cotton swabs. Associated vessels and ducts are ligated or cauterised, the pancreatic tissue is excised and the mesoduodenum is closed. Care must be taken to avoid damage to the duct system and to the major vascular supply to the area. In particular, it is very important to avoid injury to the pancreaticoduodenal vessels to prevent duodenal necrosis.
Recently a partial pancreatectomy using a bipolar vessel-sealing device (Ligasure; Covidien) has been performed in a cat, with no surgery-related complications. 18 This may demonstrate that pancreatectomy, and therefore pancreatic biopsy, can be performed using the Ligasure sealing device as a safe and fast alternative to standard surgical techniques. 18 However, it is the author’s opinion that diffusion to the pancreatic parenchyma of heat developed during sealing could lead to secondary thermic injury to the pancreas and secondary pancreatitis.
Effects of open surgical pancreatic biopsy
The clinical effects of open surgical pancreatic (wedge) biopsy have been evaluated in a study involving 15 healthy cats. 19 Mild, non-specific clinical signs after surgery included swelling of the abdominal incision, pyrexia, mild pain upon abdominal palpation and one episode of vomiting. Follow-up evaluation revealed small adhesions of the omentum to the biopsy site in 13 cats and more extensive adhesions in two cats; these may have been induced by the presence of ligature material. 19
Laparoscopic pancreatic biopsy
Exploratory surgery for obtaining pancreatic specimens is considered fairly invasive and laparoscopy represents a safe and less invasive procedure. Webb and Trott reported laparoscopic pancreatic biopsy in nine cats examined for anorexia and vomiting. 20 Cosford et al performed a laparoscopic punch biopsy of the pancreas in 11 healthy cats.21,22 Re-evaluation of the pancreatic biopsy site 1 month later documented a normal tissue response to biopsy. The punch biopsy provided high quality samples and the technique was considered useful and safe in healthy cats.
On the basis of these reports laparoscopy can be considered a minimally invasive, useful diagnostic tool by which pancreatic biopsies can be obtained in cats.20–22
Biopsy of the spleen
There is limited information in the veterinary literature regarding biopsy of the spleen. Splenic biopsy alone is rarely an indication for laparotomy. This may be due to the nature of splenic disease in companion animals, which often necessitates splenectomy rather than biopsy, as well as a perceived fear of complications associated with biopsy of such a highly vascular organ. 23 Needle aspiration is often the preferred method for minimally invasive diagnostic evaluation of the spleen. However, cytology has proven to be less accurate compared with histology. 24
Open surgical splenic biopsy
For diffuse splenic disease, the easiest procedure to perform is the open surgical suture fracture technique on the periphery of the splenic tail (see box below). The tip of the tail is easily accessible and haemorrhage is rare after tissue specimen collection. For single or multiple lesions located away from the periphery of the spleen, partial or complete splenectomy may be the technique of choice.


Laparoscopic splenic biopsy
Laparoscopic splenic biopsy has been described in human patients and found to be safe and effective. Radhakrishnan and Mayhew recently described laparoscopic splenic biopsy in 10 dogs and five cats. 23 A pair of 5 mm cup biopsy forceps clamped the splenic parenchyma after splenic capsule opening. Haemorrhage was subjectively assessed to be minimal and was comparable to that typically observed following laparoscopic hepatic biopsy. 23 The use of an absorbable gelatin sponge was reported to be helpful in slowing haemorrhage from biopsy sites. 23
Key points
FNA and cytological examination of parenchymal abdominal organs has limitations as a diagnostic tool and its accuracy and agreement with histopathological findings vary depending on the underlying disease.
An ideal biopsy sample should be of adequate size and taken from a location that represents the primary organ pathology.
Where there is diffuse disease, multiple samples of the same organ are preferred.
Focal lesions require identification before sampling.
Small sample sizes obtained from core needle biopsies may not represent the entire organ and have a tendency to become distorted.
Laparoscopic and surgical biopsies generally provide large and diagnostic samples. These should be at least 0.5–1 cm in diameter.
Appropriate tissue handling and histological interpretation are critical for a correct diagnosis.
Thorough physical examination and appropriate investigations are required for correct patient selection and to reduce the risk of post-biopsy complications.
The risks/benefits of performing a biopsy must be weighed for each case as there is always the potential for complications.

Footnotes
Funding
The author received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The author declares that there is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.