
Abstract
Practical relevance:
Thoracoscopy provides a minimally invasive means of diagnosis and offers many important benefits when compared with open thoracotomy.
Clinical challenges:
The expense of the equipment, the steep learning curve required to gain proficiency in thoracoscopic surgery, and the limitations imposed by the feline thoracic cavity, in terms of working and viewing space, are some of the challenges that have limited its uptake to date. However, it is envisaged that it will increase as a technique in feline medicine, in much the same way as laparoscopy has.
Audience:
This article is directed at veterinarians currently performing open thoracic surgery and the associated aftercare who concurrently are adept at endoscopic surgery.
Evidence base:
The article draws on the small body of literature that is available on thoracoscopy in cats, which includes reports of its use for evaluation and management of undiagnosed pleural effusion, lung lobe torsion, persistent right aortic arch and chylothorax.
Thoracoscopy – how may cats benefit?
Thoracoscopy provides a minimally invasive means of diagnosis and therapeutics for thoracic disease and offers the benefits of greatly improved lighting and magnification when compared with open thoracotomy. Thoracoscopy also minimizes patient morbidity (pain) and is associated with more rapid recovery and decreased hospitalization times compared with open surgery. 1
While thoracoscopy is a rapidly expanding technique for diagnosis and treatment in dogs, it is less commonly reported in cats.2–5 Reasons may include the presenting population consisting of more dogs than cats, and the smaller body size and apparent decreased working space in cats. 5 Laparoscopy, however, has become popular in both species and, with time, increased effort and development of equipment better suited to the smaller stature of cats, thoracoscopy should also grow as a technique in cats.
Patient selection and evaluation
Patient selection for thoracoscopy is generally the same as that for open thoracotomy. Each cat should undergo a thorough physical exam, complete blood count, biochemistry profile, urinalysis, thoracic radiography, and any tests as determined by the differential diagnosis list. Many concurrently undergo echocardiography if a heart murmur is present or if the heart is suspected to be the cause of pleural effusion. Effusion should be sampled for protein analysis, cell count, cytologic examination, and culture and susceptibility testing. Abdominal imaging with radiographs and ultrasound may be important for staging of disease such as neoplasia. Advanced imaging of the thorax should be considered in every case, as complete thoracic exploration from one approach is often difficult.


Biopsy of abnormal lung in a cat. The tip of the lung lobe has been encircled with a pre-tied loop ligature and is pale compared with the adjacent lung, which has a nodular appearance. (below) Normal lung viewed endoscopically

Collapsed lung in a cat with spontaneous pneumothorax. This patient was treated with an assisted partial lobectomy

Indications and drawbacks
Thoracoscopy and assisted procedures have been used for a variety of purposes in canine and, to a lesser extent, feline patients (see box above). The mainstay of thoracoscopy and assisted procedures is reduced morbidity and hospitalization times; avoiding rib retraction seems important.
The main drawbacks of endoscopic surgery are the expense of the equipment required and the steep learning curve associated with minimally invasive surgery. The learning curve requires the acquisition of skills translated via a two-dimensional monitor, and use of long instruments that lack the exquisite feel of the gloved hand. The surgeon must also become familiar with the need for conversion to open surgery and should be proficient with the open procedure. Endoscopic surgery should not be considered for conditions in which the clinician is not currently doing open surgery.
Equipment
For thoracoscopy (and laparoscopy) most clinicians use 5 mm instrumentation, which may be slightly large for small cats and the length may make operation more difficult. Smaller equipment is available and is commonly used in exotic species including reptiles and birds.6,7 Endoscope sizes as small as 1.9 mm are available (Karl Storz, Goleta, CA, USA); however, a 5 mm or 2.7 mm 30° rigid endoscope provides a better image and is not too large for the intercostal space in cats. Small, lightweight, threaded graphite ports and 1.7, 2 or 3 mm instrumentation are also available (Figures 3 and 4), making endoscopy possible in very small animals. 7

Small instruments available for thoracoscopy in cats. Instruments (a–e) are size 3.0 mm and ports (f) are 3.5 mm. (a) Curved dissectors, similar to mosquito hemostatic forceps; (b) fine scissors, similar to Metzenbaum scissors; (c and d) grasping forceps; (e) hooked scissors for cutting suture; (f) lightweight graphite, threaded port
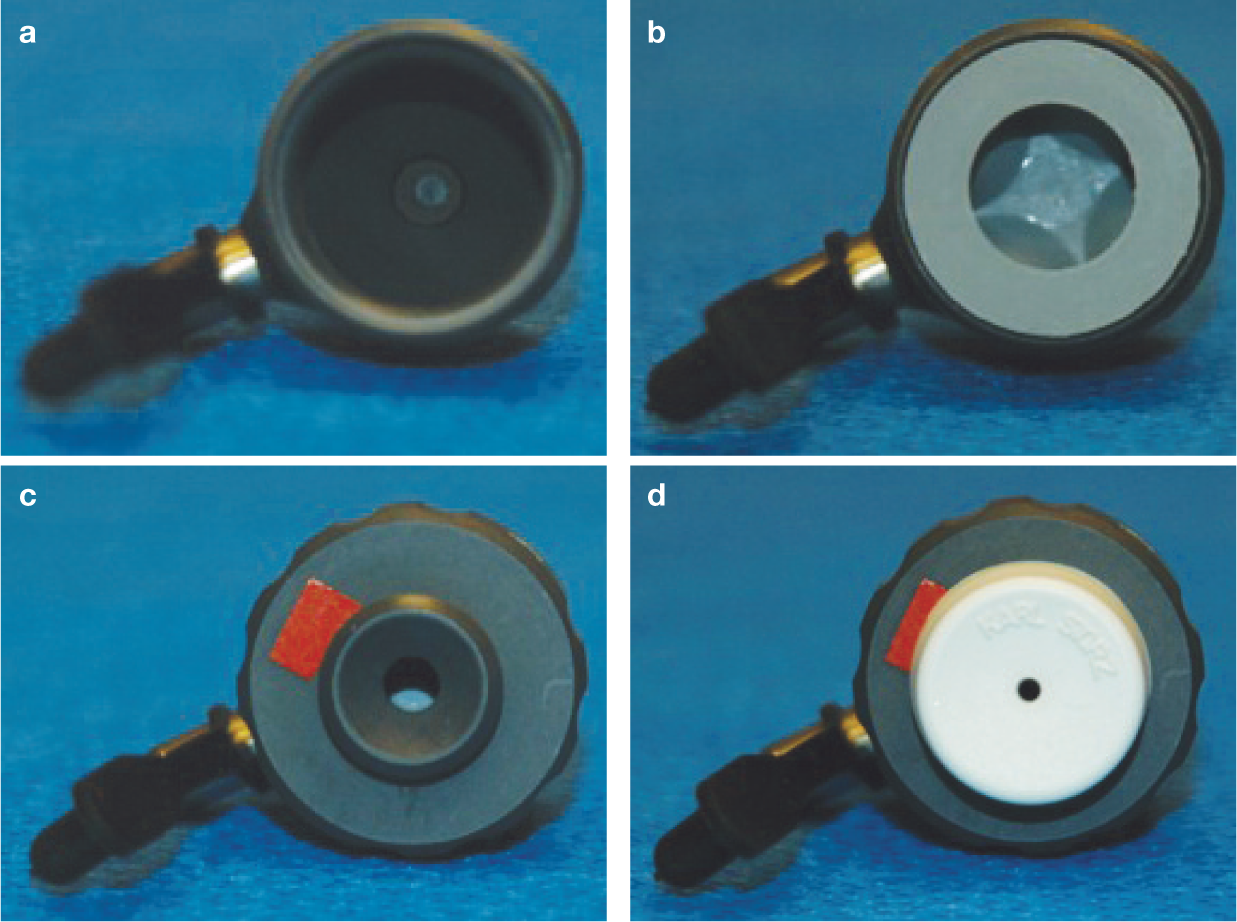
Standard threaded port altered to allow insufflation of the abdomen or chest. (a) Open end of the port for typical thoracoscopy; (b) insert within the port that allows instrument passage during insufflation; (c) screw cap in place to guide instrument passage during insufflation; (d) grommet in place to ensure no loss of insufflation during instrument passage
Thoracostomy tubes should be placed as they would for open surgery. The tube is used to monitor for air or blood accumulation in the pleural space as an indication for further medical or surgical therapy, and for instillation of local anesthetics for analgesia. Thoracoscopy does not obviate the need for critical care and 24 h monitoring before and after surgery.


Clips have been applied to all tissue dorsal to the aorta (arrowhead) and ventral to the sympathetic trunk (arrow)
Limitations of working within the thoracic cavity
The normal thoracic cavity is supported by a rigid costal arch system, making viewing simple. However, in cats there is a challenge in that the working space seems small despite the rigid support structures. Thoracoscopy is usually performed with the assistance of mechanical ventilation because of the creation of an open thorax. Decreasing the lung volume allows the operator to view the majority of the thorax and is typically done by decreasing the tidal volume by 50%. Open ports are used without valves since insufflation is not required – again, because of the rigid thoracic wall.
In one study, thoracoscopy resulted in significantly decreased PaO2, CaO2, end-tidal CO2 and increased dead space ventilation, PA-aO2 (alveolar to arterial oxygen pressure gradient) and heart rate. 8 Oxygen delivery, PaCO2 and cardiac index were not affected. The changes are likely to be related to pulmonary atelectasis and reduced functional residual capacity. It is important to note that these findings occurred in normal dogs. Changes in clinically affected cats would likely depend on the disease process present, and cats with pulmonary disease may be more significantly affected by thoracoscopy.
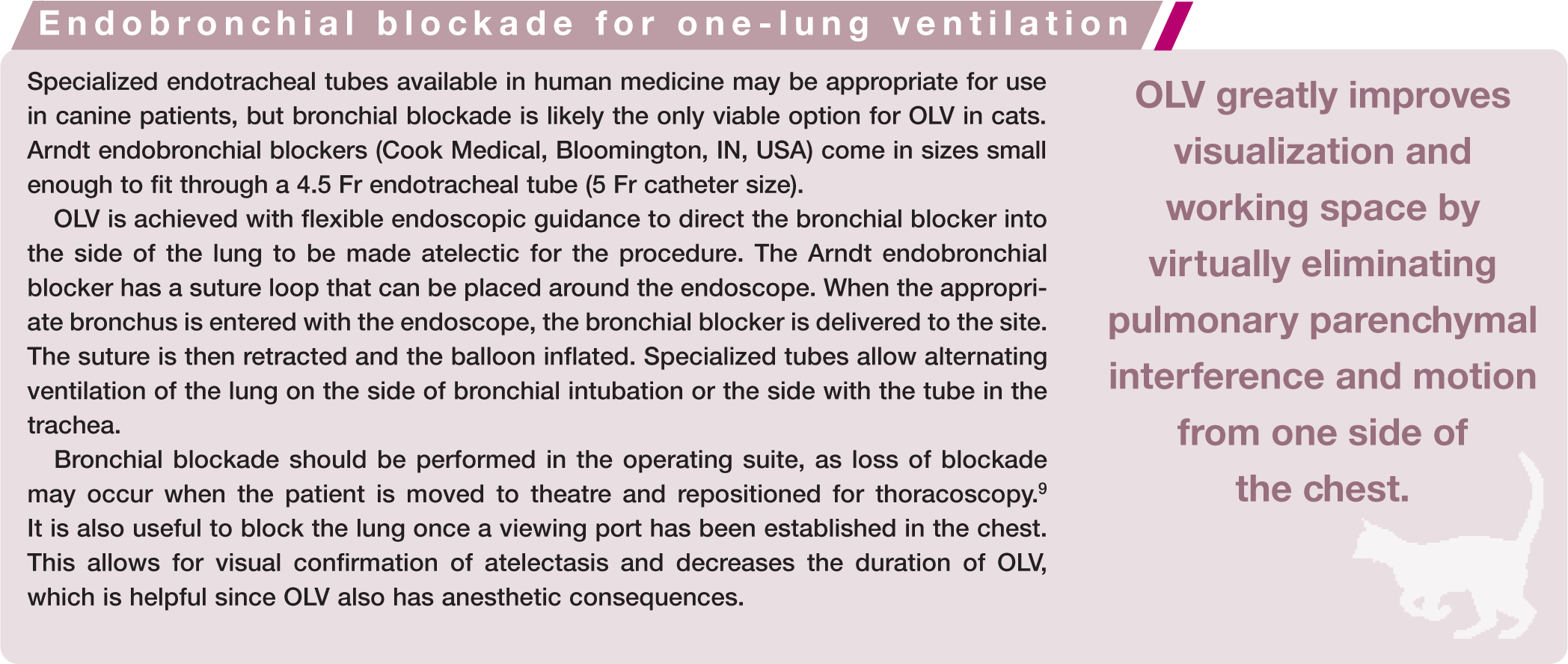
One-lung ventilation
Further improvement in viewing and working space for certain procedures has been achieved by one-lung ventilation (OLV). OLV greatly improves visualization and working space because one entire side of the chest is nearly free of pulmonary parenchymal interference and motion. In cats, OLV can be achieved with the use of bronchial blockers (see box).

OLV has been reported to result in increased shunt fraction, PaCO2, cardiac index, heart rate and arterial blood pressure, and decreased PaO2 and systemic vascular resistance. 10 The changes were not severe in normal dogs. The use of positive end-expiratory pressure (PEEP) at 5 cm H2O improved PaO2 in dogs undergoing OLV during thoracoscopy and did not have adverse effects on hemodynamics in normal dogs. 11 Changes that might occur in patients with abnormal thoracic conditions are not widely reported and there have been no studies published on changes in cats.
Regardless of whether OLV is used, intensive monitoring should be carried out in cats undergoing thoracoscopy or open thoracotomy.
Low pressure thoracic insufflation
Insufflation is required for laparoscopy to gain a working space due to the lack of a rigid abdominal wall. Insufflation of the thoracic cavity has been reported in dogs. 12 Cardiac output, and systolic and diastolic blood pressures decreased significantly at 3 mmHg of insufflation pressure; at 6 mmHg, there was a significant increase in central venous pressure and a decrease in heart rate. 12 The results of the study cautioned against the use of thoracic insufflation, even at low pressures. However, some surgeons have used very low insufflation pressures of 1–2 mmHg in cats to increase the working space (G Dupré, personal communication, July 2012).
Since OLV is difficult to achieve in dogs, and may be even more challenging in cats due to their small size, investigation of low pressure thoracic insufflation in cats may be warranted. Perhaps insufflation can be used during bilateral lung ventilation to slightly (but just sufficiently) improve the viewing and working space in these small patients.
Placement of ports
Access to the chest is limited to small incisions for introducing the endoscope and instruments. Ports protect the tissues of the intercostal space and may be rigid or flexible. The author prefers flexible ports, where possible, to avoid compression of the intercostal vessels and nerves against the ribs. Compression of the nerves is likely to result in some pain, and compression of vessels may prevent visible hemorrhage, which can be fatal if undiagnosed.
Ports are placed via a mini-thoracotomy. The skin is incised with a scalpel and the surgeon bluntly dissects through the musculature until the thorax is entered. The port is placed using a blunt obturator to avoid trauma to the lung. Small, threaded ports are useful, but require care to avoid trauma. Endoscopic visualization should be used for any port placed after the first, to minimize the risk of vascular or pulmonary trauma.
Port sites have been described for many procedures and are beyond the scope of this article.
Approaches to the chest
There are two main approaches to the chest for thoracoscopic (and open) surgery: lateral (Figure 6) and sternal (Figure 7). The ability to view the contents is limited by each approach. The lateral approach allows complete evaluation of one hemithorax; the sternal approach allows bilateral evaluation of the chest, except for the dorsal aspect. A third approach has been described for thoracoscopy and consists of lateral approaches with the patient in sternal recumbency; this allows for examination of both hemithoraces minus the ventral aspects.

Intercostal thoracoscopy in a cat. This illustration shows the typical placement of an endoscope in the central port, with instrument ports cranial and caudal, all triangulated towards the operative target
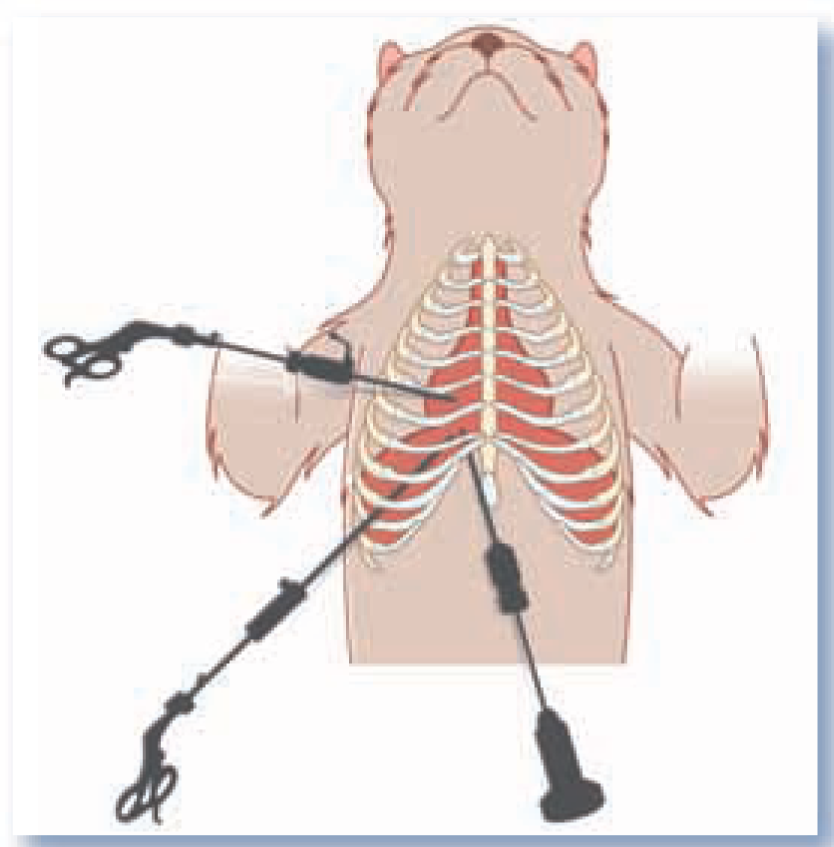
Thoracoscopyin a dorsally recumbent cat mimics the approach gained by median sternotomy. The first port is placed in a paraxiphoid position. Instrument ports are placed as desired in the intercostal spaces ventral to the pulmonary excursions and may be placed on one side of the thorax, as depicted here, or on the left and right sides of the chest
The lateral approach is undertaken simply by placing intercostal ports via mini-thoracotomies. The sternal approach mimics the access gained via a median sternotomy. The first port is usually placed adjacent to the base of the xiphoid cartilage, or paraxiphoid. A threaded port is best for this site, and its insertion can be viewed with a 0° endoscope placed in the lumen of the port. The port is directed in a dorsal direction relative to the patient and into the ipsilateral hemithorax. Viewing during placement allows the surgeon to visualize passage through the subcutis, diaphragm and caudal mediastinum, and to stop the insertion as soon as the chest is entered, optimizing placement. Insertion too far into the chest will limit visualization and instrument operation, and too short an insertion will preclude viewing or operation. Once the paraxiphoid port is in place, the chest can be examined (Figure 8) and an intercostal port can be placed in the ipsilateral hemithorax for division of the ventral mediastinum, after which the contralateral hemithorax can be examined.

Appearance of the heart (arrowheads) within the chest of a cat with severe, fibrosing pleuritis. Pulmonary parenchyma is not visible
Specialized instrumentation can greatly improve the ease and speed of thoracoscopy (see page 29).


Thoracic duct identification in a cat. Cranial is to the right of the image, dorsal is at the top of the image. The thoracic duct (arrow) is a grey, linear structure dorsal to the aorta (arrowheads)
Complications of thoracoscopy
Thoracoscopy does not eliminate any of the complications associated with the disease process and its associated surgery. Thus, the complications of thoracoscopy are the same as those for open thoracotomy. Anesthesia should be carefully monitored, and conversion to open surgery may be necessary if adequate ventilation cannot be achieved with the decreased tidal volume necessary for visualization.
Key points
Feline thoracoscopy is not performed as commonly as canine thoracoscopy, but development of technology and procedural descriptions make it a viable option.
Thoracoscopic-assisted procedures that avoid rib retraction seem to be providing a bridge, until wholly endoscopic procedures are developed.
Open surgery is an option when immediate intervention is required during thoracoscopy. The complications for the two procedures are similar.
Aftercare for open surgery and thoracoscopy are similar, but hopefully thoracoscopic approaches will minimize morbidity and duration of hospitalization in feline patients.
Footnotes
Funding
The author received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The author does not have any potential conflicts of interest to declare.