
Abstract
Practical relevance:
Minimally invasive techniques are becoming increasingly available in both first opinion and referral veterinary surgeries. Clients may be reluctant to pursue open surgery for the collection of biopsy samples in a sick cat but may be more open to a laparoscopic approach. Furthermore, a laparoscopic approach provides excellent visualization of the abdominal organs and enables high quality biopsies to be taken that are invariably more diagnostic than percutaneous needle biopsies. Although the feline patient is small in size, its distensible abdomen allows more room for surgical manipulation than afforded by a similar sized canine patient.
Clinical challenges:
Clinical challenges for the most part relate to mastering laparoscopic technique. Familiarity with the use of long instrumentation viewed on a two-dimensional screen is essential. Hemostasis is an important consideration and suitable instrumentation for achieving hemostasis should be available at all times. Insufflation of the abdomen carries its own challenges with regard to anesthesia and this is covered in an accompanying article in this Special Issue series.
Aim:
This article introduces the feline practitioner to basic techniques required to effectively utilize diagnostic laparoscopy within feline medical investigations. It focuses on the common procedures of liver biopsy, cholecystocentesis, pancreatic biopsy, kidney biopsy and laparoscopic-assisted intestinal biopsy.
Evidence base:
Information provided in this article is drawn from the published literature and the authors’ own clinical experience.
Laparoscopy – favorable characteristics and common procedures
Laparoscopy provides minimally invasive access to the abdominal cavity, and is considered a safe alternative to conventional open surgery for exploration and biopsy collection. Rapid recovery in debilitated patients, as well as enhanced diagnostic accuracy courtesy of increased magnification, illumination and field of view in a small working space, are all favorable characteristics that have raised awareness and uptake of laparoscopy in feline patients. Laparoscopy has, to date, principally been used for diagnostic purposes in feline practice, the most common procedures being liver biopsy, cholecystocentesis, pancreatic biopsy, kidney biopsy and laparoscopic-assisted intestinal biopsy.
Patient evaluation and preparation
Patient evaluation prior to laparoscopy should be performed as it would for surgical laparotomy. A full clinical history, physical exam, complete blood count, platelet count, serum biochemistry and urinalysis serve as the ‘minimum database’. Patients that require biopsies of the liver due to severe liver pathology should ideally have prothrombin time and activated partial thromboplastin time measured as well. Buccal mucosal bleeding time should also be considered, although this is most relevant in canine breeds predisposed to von Willebrand’s disease. Although coagulopathies are a relative contraindication to liver biopsy, the patient’s coagulation status does not necessarily predict the risk of post-procedural hemorrhage. 1 If a biopsy is required for accurate diagnosis and treatment, a minimally invasive approach will lead to less hemorrhage compared with laparotomy, and any bleeding can usually be adequately controlled without resorting to open surgery.


Basic set-up for diagnostic laparoscopy

5 mm x 29 cm 0° rigid operating telescope
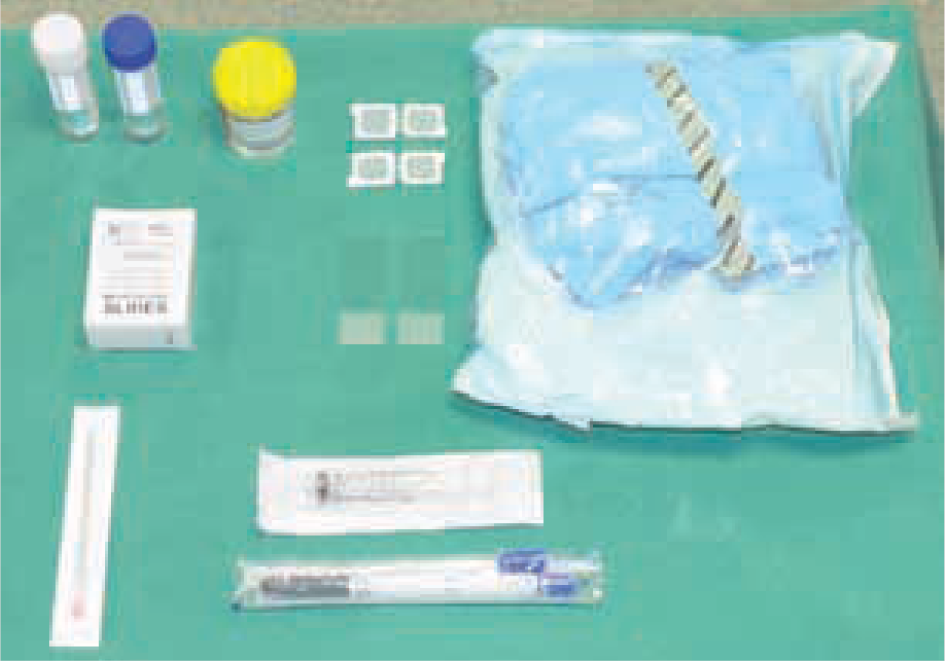
Set-up for sampling
Diagnostic imaging (eg, ultrasonography) is recommended as a complementary diagnostic technique prior to any exploratory surgery (laparotomy or laparoscopy), especially in the presence of suspected disease deep within the parenchyma of an organ.
Diagnostic laparoscopy is performed under general anesthesia and the patient should be fasted for at least 12 h prior to the procedure. The urinary bladder is evacuated to reduce the risk of inadvertent puncture during trocar placement.
The objectives of the laparoscopic procedure will influence both patient positioning and the selection of cannula placement sites. Most commonly, diagnostic laparoscopy is performed via a right lateral or a ventral midline approach (Figures 4 and 5). The right lateral approach (cat lying in left lateral recumbency) is recommended for diagnostic evaluation of the liver, gall bladder, right limb of the pancreas, duodenum, right kidney and right adrenal gland. A ventral approach is useful for many operative procedures, and offers good visualization of the liver, gall bladder, pancreas (left and right limb), stomach, intestines, reproductive system, urinary bladder and spleen. With the ventral approach, visualization is sometimes partially obscured by the falciform ligament; however, this is much less prominent in feline patients compared with their canine counterparts, and is rarely a problem in practice. A wide variety of different cannulae are available to facilitate entry of the endoscope into the abdominal cavity (see box, page 19).

Ventral midline approach: (a) two-port entry and (b) three-port entry. The latter would typically be used for laparoscopic-assisted intestinal biopsy

Right lateral approach

General exploration of the abdomen
The surgeon should be aware that the first priority in diagnostic laparoscopy is not the visualization of tissues and organs. Rather, it is always safe laparoscopic technique, which requires, first, visualizing the introduction of trocars/cannulae and, secondly, visualizing the introduction, movement and manipulation of instrumentation within the abdomen. 2
The palpation probe is the most useful piece of equipment for exploring the abdomen because it has a relatively atraumatic blunt end that can be used to lift liver lobes, manipulate intestines and move omentum. It is also used for ballottement of the gall bladder and to provide tactile feedback from soft tissue structures in the absence of direct digital palpation. Additionally, the palpation probe has 1 cm graduation marks, which can be used to measure various organs and lesions identified during exploration.
Rotating the camera port 180° will allow visualization of caudal abdominal organs such as the colon, urinary bladder, reproductive organs and internal inguinal rings.
After full exploration of the abdomen, the palpation probe can be replaced by an alternative instrument, depending on the specific requirements; typically this will be biopsy forceps. Electrocautery units are not usually necessary in diagnostic laparoscopy but should be available in case of intractable hemorrhage from a biopsy site. This is rare but can occur when taking biopsies from relatively vascular tumors.
Liver biopsy
The simplest way to collect a laparoscopic liver biopsy for diagnosis of diffuse liver disease is with the use of 5 mm cup (clam shell) biopsy forceps (Figure 6). In brief, the procedure (which is described in detail in the box) involves strategically placing closed forceps underneath the edge of a chosen liver lobe. The forceps are opened and slowly withdrawn, allowing the liver edge to fall into the open jaws. The biopsy cup is then closed over the sample and held in place for 30–45 s to encourage hemostasis. The forceps are then gently twisted and retracted towards the instrument port.

5 mm cup (clam shell) biopsy forceps
Care should be taken to avoid rough handling as this can lead to tearing and excessive hemorrhage. In cases of significant hepatic fibrosis, tearing is sometimes unavoidable, and the liver tissue may not cut completely until the forceps are actually retracted into the trocar, such that the sharp edge of the trocar provides an additional cutting surface.
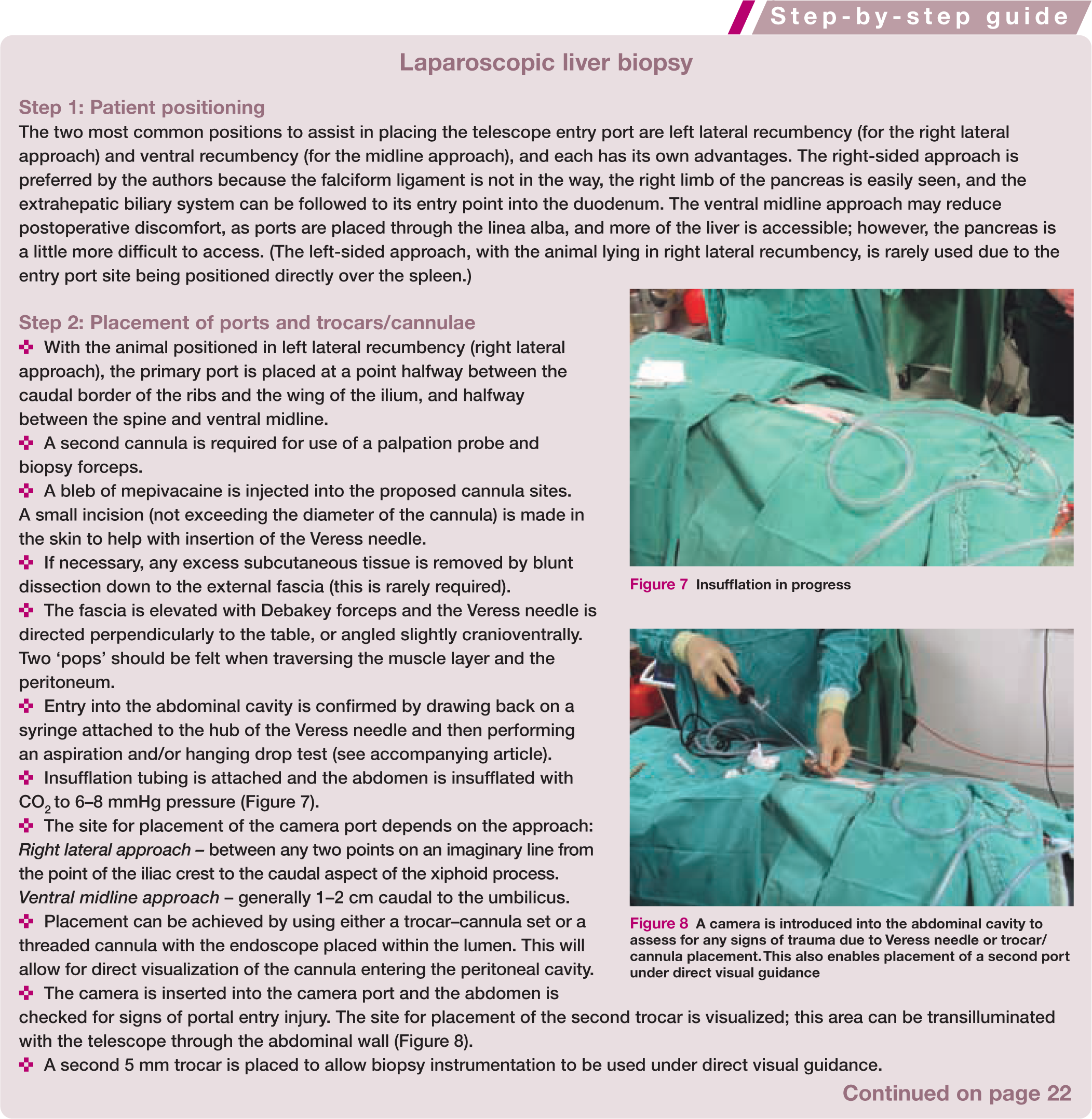

Insufflation in progress

A camera is introduced into the abdominal cavity to assess for any signs of trauma due to Veress needle or trocar/ cannula placement. This also enables placement of a second port under direct visual guidance
Provided it is performed correctly, this technique has been shown to cause minimal bleeding in healthy dogs, and produce adequate tissue volume and high quality samples.3,4 Several samples should be taken from different lobes. Where there are discrete lesions on the surface of the liver these should be biopsied at the edge of the lesion. The lower jaw of the open biopsy forceps is introduced into normal liver parenchyma at the edge of, and facing into, the lesion and the upper jaw is closed to obtain the sample. The forceps are held closed for 30–45 s before removing the biopsy sample, as detailed above. In all cases, the biopsy sites should be observed until the surgeon is satisfied that bleeding has ceased. The palpation probe can be used to apply direct pressure to assist clot formation, or a piece of hemostatic sponge (Gelfoam) can be placed into the lesion with grasping forceps, although the latter is rarely necessary.
Loop ligature technique
If coagulopathy or hemorrhage is a concern, or a larger focal lesion near the edge of a lobe is to be removed, it may be preferable to apply a pre-tied loop ligature (see page 23) and collect a liver sample using the ‘guillotine’ technique (Figure 13). This reduces the risk of severe hemorrhage; however, a second instrument port will be needed to place the ligature (Figure 4b). The loop is passed through the instrument port, under direct visual guidance, and placed around a tip of the liver lobe with the assistance of atraumatic grasping forceps inserted through the second instrument port. When the loop is in position, it is tied by advancing the plastic applicator; this slides the pre-tied slip knot down until it tightens securely into place, ligating the vasculature and bile ducts within the parenchyma. The liver tissue, as with the open guillotine biopsy method, is cut distal to the ligature with curved scissors and either withdrawn through the cannula or placed in an endoscopic sample retrieval bag and removed through an enlarged port site, as required.
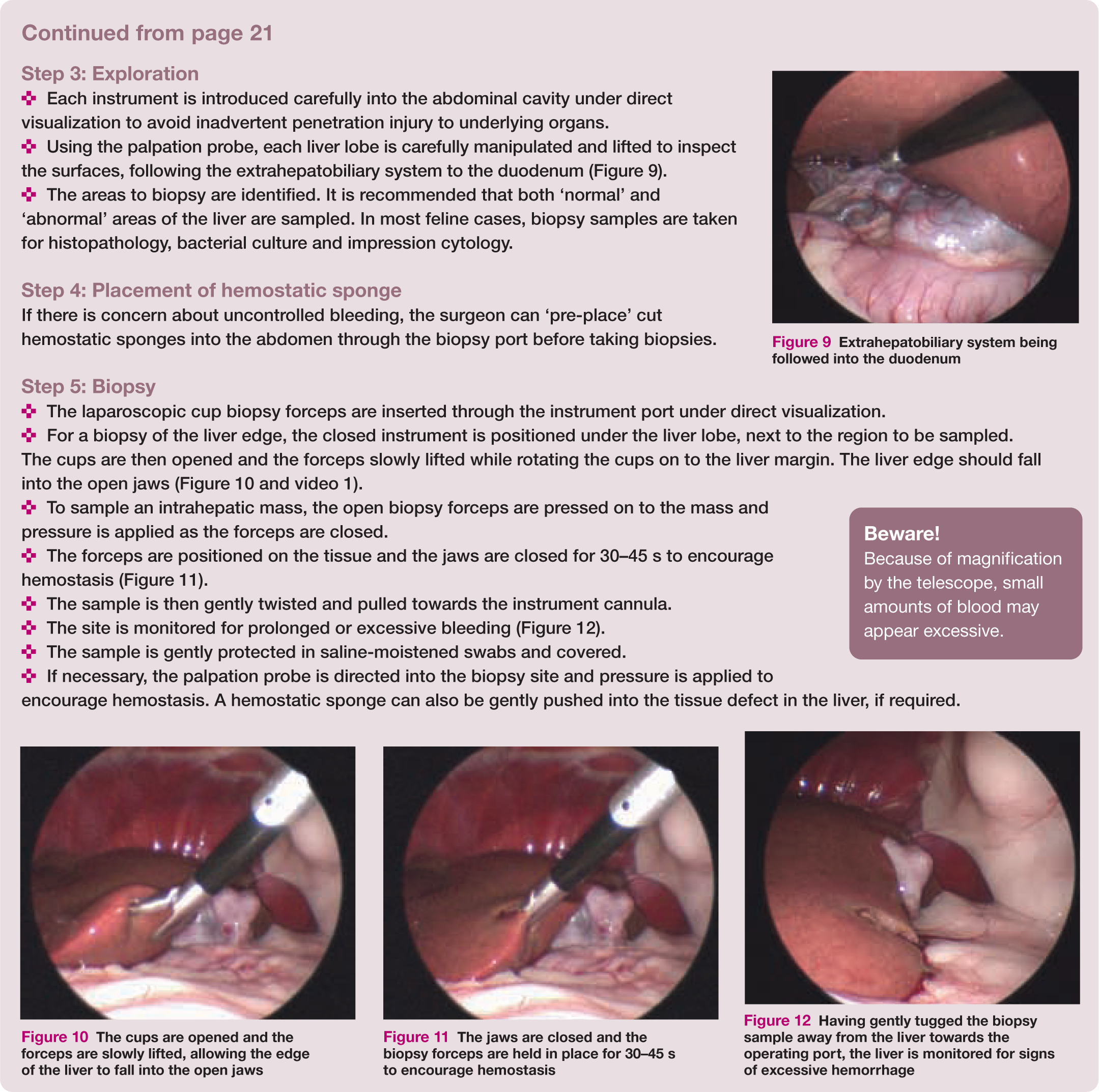

Extrahepatobiliary system being followed into the duodenum
The cups are opened and the forceps are slowly lifted, allowing the edge of the liver to fall into the open jaws
The jaws are closed and the biopsy forceps are held in place for 30–45 s to encourage hemostasis

Having gently tugged the biopsy sample away from the liver towards the operating port, the liver is monitored for signs of excessive hemorrhage

Liver sampling using the loop ligature technique. (a) Tip of loop applicator. (b) Pre-tied loop at the other end of the applicator encircling the tip of a liver lobe. (c) The tip of the applicator is snapped and the operator pulls on the toggle to slide the knot down and tighten on to the sample
Cholecystocentesis
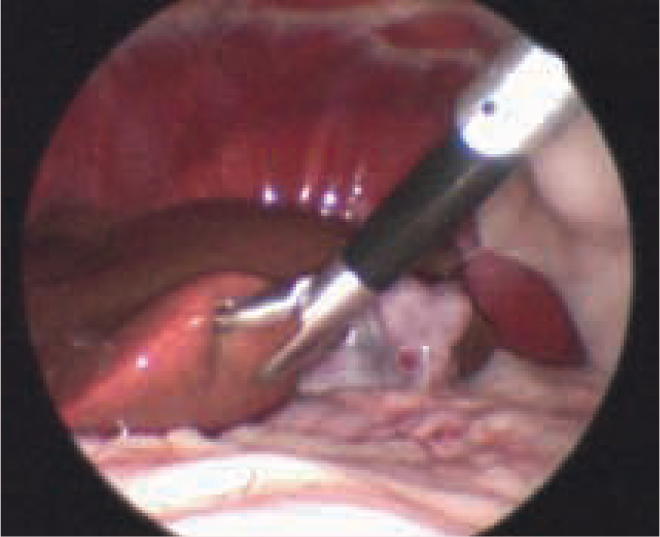
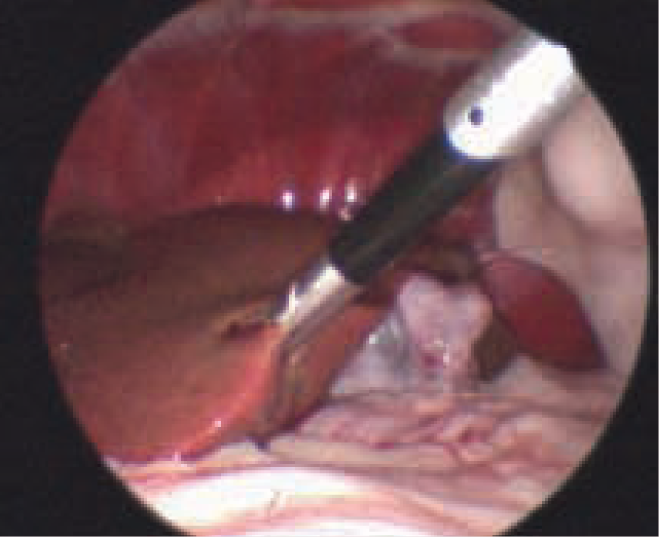
Bile aspirates for cytology and bacteriology are important when performing gastrointestinal (GI) investigations in cats, particularly those suspected of having triaditis. Laparoscopic cholecystocentesis (see below and video 2) is considered safe and easy to perform. The authors use spinal needles (18–20 G x 3–6", or 20–22 G if fluid is viscous) with an inner stylet that can be removed once the lumen of the gall bladder has been penetrated. The size, fullness and firmness of the gall bladder can be assessed both visually and with the palpation probe (Figure 14).

Assessment of the gall bladder with a palpation probe


Spinal needle penetrating the gall bladder

Aspiration of gall bladder contents
Pancreatic examination and biopsy
In cats, pancreatic biopsy is often performed at the same time as hepatic biopsy and cholecystocentesis, and requires a single instrument port. The right lateral approach (animal in left lateral recumbency) is preferred as this provides excellent visualization of most of the right limb and body of the pancreas, and allows adequate access for biopsy. Clinical judgement will help the clinician decide whether this area is sufficient to allow for a representative sample.
A 5 mm punch biopsy forceps (Figure 17) can be used to collect the sample from the periphery of the pancreas. Care should be exercised to avoid sampling the central portion of the pancreas and damaging the pancreatic ducts and pancreaticoduodenal vessels at the tip of the right pancreatic limb. It is sometimes helpful to flip the duodenum over and examine the pancreas from the other side, as the edge of the pancreas may be more accessible.

5 mm punch biopsy forceps
Studies have shown this technique to be safe in healthy dogs 5 and cats, 6 with no significant clinical abnormalities detected postoperatively despite histopathological evidence of inflammation around the biopsy sites. 5
Visualization of the left limb
It is difficult to examine the entire pancreas laparoscopically because the left limb lays within the greater omentum caudal to the greater curvature of the stomach, and so requires more skill to visualize. A mid-abdominal ventral approach is made, with the patient in a reverse Trendelenburg position (ie, tilted so that the lower extremities are below the level of the head and neck). The greater curvature of the stomach is retracted and elevated forwards, and a window is created in an avascular part of the greater omentum caudal to the gastroepiploic vessels in order to enter the omental bursa and examine the left lobe.
Alternatively, a limited view of the left lobe can be obtained relatively easily by tilting the patient to the right by 45° and retracting the spleen towards the midline. This allows the distal tip of the left limb to be visualized between the spleen and left kidney, caudal to the stomach.
Visualization of the right limb
In the right lateral approach, the palpation probe can be used to elevate the descending duodenum. This will reveal the right limb of the pancreas. The palpation probe may be needed to push the omentum and colon to the side in order to achieve adequate visualization. If there are adhesions due to active peritonitis, a third cannula will need to be placed so that the adhesions can be broken down.
Biopsy procedure
When taking pancreatic biopsies, it is best to select an area away from the entry point of the pancreatic duct to the duodenum. Usually the distal aspect of the right limb is sampled as this avoids the center of the pancreas where the main pancreatic duct lies. In a similar fashion to collecting a liver biopsy, the punch forceps are introduced under direct visualization beneath the edge of the pancreas, opened and slowly withdrawn, allowing the tissue to fall into the jaws of the instrument (see video 3). The forceps are closed and held in position for 30–45 s before being gently retracted towards the biopsy cannula (Figure 18). The authors recommend collecting two biopsy samples.

Forceps are held in position for 30–45 s before retrieving the pancreatic biopsy sample
Concerns regarding pancreatitis as a potential complication of pancreatic biopsy appear to be unfounded, with several studies evaluating laparoscopic pancreatic biopsies in normal dogs finding no evidence of secondary pancreatitis. 5
Kidney biopsy
A percutaneous Tru-Cut needle technique is usually used to obtain a kidney biopsy, with the patient in lateral or ventrolateral recumbency. This procedure can be achieved using a single port and a percutaneously placed needle that is guided to a location directly ventral and caudal to the kidney. However, it is advisable to place an additional port; this will enable a palpation probe to be used to help manipulate the kidney into position and to place direct pressure on the biopsy site to minimize hemorrhage.
The significant benefit of laparoscopic-guided kidney biopsies is the ability to accurately place the biopsy needle, especially where there is focal disease, and to visualize and control hemorrhage to ensure hemostasis has been achieved prior to closure. As hemorrhage is more easily controlled, a larger biopsy needle (14–16 G) can be used, providing a more diagnostic sample.
Laparoscopic-assisted intestinal biopsy
Biopsy of the small intestine is usually performed using a laparoscopic-assisted technique. In humans, in which the small intestinal lumen is significantly larger, endoscopic stapling devices can be used to resect small antimesenteric sections of intestine. In small animals, this would likely result in a significant reduction in luminal diameter and, therefore, is not considered a practical option. Instead, a ‘mini-laparotomy’ is performed by exteriorizing a small bowel segment through a port incision.


Intestine grasped within the jaws of Babcock forceps

Gelpi retractors in place
A technique for laparoscopic-assisted intestinal biopsy involving a left lateral approach is described on page 25.
Final inspection and closure
Following diagnostic laparoscopy, the abdominal cavity is inspected to ensure adequate hemostasis, the CO2 insufflation tubing is disconnected and all valves are opened to decompress the abdomen.
Each incision in the fascia, subcutaneous tissue and skin is closed with a small mattress suture using a monofilament absorbable material. Alternatively, tissue glue may be used instead of skin sutures.
Postoperative care
Many cats undergoing laparoscopic organ biopsy are ill and so should continue to receive appropriate intensive care following recovery. ‘Simple’ cases of medical investigation that do not require intensive care are sent home on the day of surgery. Postoperative care includes monitoring for signs of pain and bleeding, and provision of nutritional support. This should be continued until a definitive diagnosis is obtained and specific therapy can be instituted.
Key points
Although building confidence and competency in minimally invasive surgery requires a large investment of time and financial commitment, for both training and equipment purchase, it is rewarding professionally, financially and personally.
Diagnostic laparoscopy generally has an easier learning curve compared with flexible gastrointestinal endoscopy. A routine outpatient diagnostic laparoscopic procedure can often be performed in 20 mins.
Because of its minimal invasiveness, clients are often willing to accept laparoscopy as an option, especially in feline patients.
Footnotes
Acknowledgements
The authors are grateful to Philip Lhermette for providing the video clips that accompany this article.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.