
Abstract
Practical relevance:
Respiratory endoscopy is a useful diagnostic tool to evaluate the airways for the presence of mass lesions or foreign material while allowing for sample collection for cytologic and microbiologic assessment. While bronchial disease (eosinophilic or neutrophilic) is the most common lower respiratory disease identified in cats, infectious, anomalous and neoplastic conditions can clinically mimic inflammatory bronchial disease. Diagnostic imaging is unable to define the etiology for clinical signs of cough, tachypnea or respiratory difficulty, necessitating visual evaluation and collection of airway samples. Endoscopy allows intervention that can be life-saving and also confirmation of disease, which is important given that life-long medication is likely to be required for management of inflammatory airway disease.
Patient group:
Cats with either airway or pulmonary disease benefit from laryngoscopy, tracheoscopy and bronchoscopy to determine an etiologic diagnosis. In the best situation, animals that require these procedures present early in the course of disease before clinical decompensation precludes anesthetic intervention. However, in some instances, these tests must be performed in unstable cats, which heightens the risk of the procedure. Cats that do not respond to empiric medical therapy can also benefit from bronchoscopic evaluation.
Clinical challenges:
Due to the small size of feline airways and the tendency for cats to develop laryngospasm, passage of endoscopic equipment can be difficult. Bronchoconstriction can lead to hemoglobin desaturation with oxygen and respiratory compromise.
Evidence base:
This article reviews published studies and case reports pertaining to the diagnostic approach to feline respiratory disease, focusing specifically on endoscopic examination of the lower airways in cats. It also discusses appropriate case selection, equipment, endoscopic techniques and visual findings based primarily on the authors’ experiences.
Why consider bronchoscopy over blind sampling?
Endoscopy of the respiratory tract is invaluable in the diagnostic work-up of animals with respiratory disease. Laryngeal examination is indicated for cats with upper airway complaints such as voice change or inspiratory difficulty and can easily be performed as a sole procedure or immediately prior to lower airway evaluation. The cat with a cough, respiratory difficulty or tachypnea is likely to have lower airway or parenchymal disease and is best examined by bronchoscopy.
Bronchoscopic evaluation of the respiratory tract allows visualization of airway abnormalities as well as collection of bronchoalveolar lavage (BAL) samples to investigate respiratory tract disease in cats.1,2 Due to the small airway diameter in cats, necessitating specialized endoscopic equipment, and the potential for life-threatening bronchoconstriction in feline patients, bronchoscopy is often reserved for severe, refractory or tertiary referral cases. Despite the potential risk associated with the procedure, bronchoscopy can be performed safely in the vast majority of cases when the animal is examined by an experienced individual. 3
Clinicians sometimes elect to perform blind endotracheal BAL due to concerns about anesthesia or the lack of appropriate equipment. 4 While this technique might provide an appropriate cytology sample, bronchoscopy offers many advantages over blind sampling techniques through the ability to visualize the airway and to obtain samples from specific lung lobes. 5 Airway lesions tend to be less dramatic in cats than in dogs; nonetheless, there is more to learn by performing a complete examination of the airways.

Indications
Endoscopic examination of the respiratory tract undoubtedly contributes to diagnostic assessment and also allows therapeutic intervention in cats with obstructive large airway disease. As mentioned above, laryngoscopy is indicated for cats with clinical signs related to upper airway obstruction such as stertor or stridor. Gagging, voice change and inspiratory noise or effort are also indications for laryngoscopy. Some of these signs can be seen with cervical tracheal lesions and will require tracheoscopy. Radiographs of the region are helpful in localizing the lesion and determining whether laryngoscopy, tracheoscopy or bronchoscopy might be required. Importantly, a thorough laryngeal examination should be performed in any cat anesthetized for a respiratory procedure because hyperemia, accumulation of secretions and edema are often found in conjunction with lower airway disease and can contribute to clinical signs.
A common indication for bronchoscopy is to document a specific cause for acute or chronic coughing. Coughing is usually associated with an infectious or inflammatory etiology. However, other causes include airway collapse, bronchiectasis or foreign body aspiration. Bronchoscopy can also be helpful in determining the etiology for respiratory difficulty or tachypnea associated with lung disease. However, caution is particularly warranted in these cases because of the risks associated with anesthetizing a cat in respiratory distress.

Bronchoscopy with BAL is useful primarily in airway-oriented processes; its utility is limited in cases of interstitial lung disease and respiratory neoplasia due to the lack of cellular infiltration into the airways. While an endoscopic biopsy or brushing can detect neoplasia that is endobronchial, these lesions are rare and typically require a lung biopsy to obtain a histologic diagnosis.7,8
Another advantage of performing bronchoscopy rather than blind BAL is the unique ability to undertake therapeutic interventions. For example, bronchoscopy can be used to visualize and remove foreign material. 9 It can also assist in debulking or removing airway-associated masses. 10 Finally, airway samples can be collected from specific sites for cytologic or histopathologic evaluation using endoscopic brushes, transbronchial aspiration needles and endoscopy biopsy forceps.
In instances where surgical disease might be encountered (ie, significant laryngeal disease, obstructive tracheal or bronchial masses, or when there is the potential for pneumothorax to develop because of bullous disease), it is essential that appropriate surgical facilities are available following the diagnostic procedure. This will decrease patient morbidity as well as potential mortality and will facilitate transfer of care. While bronchoscopy can be safely performed in many animals, the procedure should be avoided in cats that are not suitable for anesthesia. This includes cats with severe obstructive upper or lower airway disease that cannot be stabilized, cats with severe parenchymal disease or those with unidentified compromise of ventilation or perfusion.

The outer diameter of scopes used for feline bronchoscopy and laryngoscopy ranges from 2.5–4.0 mm. This image shows flexible endoscopes with an outer diameter ranging from 2.5–5.0 mm

A variety of instruments are available for bronchoscopic procedures. Generally the outer diameter of the instrument must be 0.2 mm less than the instrument channel of the scope to safely pass the length. Pictured here are 1.8 mm instruments: (a) loop snare, (b) retrieval forceps without spike (spiked forceps are useful for biopsy), (c) three-pronged grabber, (d) Wang needle and (e) guarded microbiology brush (unguarded cytology brushes are also available). Many of these instruments are also available in 1.0 mm diameter for smaller scopes with a 1.2 mm channel

Suction trap used for collecting BAL samples

Patient assessment and preparation
It is important to gauge the severity of respiratory compromise and to localize disease prior to performing respiratory investigations because clinical signs can worsen during recovery from anesthesia. Respiratory rate and effort are easy clinical parameters to assess. In addition to thoracic and cervical radiographs, pulse oximetry is recommended prior to anesthesia. If SpO2 readings do not exceed 95%, hypoxemia is likely and arterial blood gas measurement is recommended when possible. While hypoxemia is not necessarily a contraindication to bronchoscopy, pulse oximetry is valuable as a baseline assessment prior to the procedure and useful for comparison with post-procedural values. Similarly, pulse oximetry is useful as a baseline for ongoing patient monitoring following bronchoscopy and into treatment.
Bronchoscopy is typically performed with the patient in sternal recumbency with the head elevated near the edge of the table, although some clinicians prefer lateral recumbency. Terbutaline (0.01 mg/kg SC) administered before the procedure and immediately before BAL reduces the risk of life-threatening bronchoconstriction and enhances the safety of the procedure.3,6 While inhaled albuterol might be equally effective, bronchoconstriction could limit deposition of the drug at the site where it is needed. It is also unclear whether inhaled products could alter airway samples, thus parenteral drugs are used more commonly.
Intravenous access is required for anesthetic induction and to allow for resuscitation in the event of an untoward anesthetic reaction. Pre-oxygenation is performed for 5 mins prior to the procedure to delay desaturation with oxygen. For respiratory endoscopy, a combination of propofol and a benzodiazepine provides a smooth and balanced anesthetic induction; however, it is most important that the anesthetic regimen is tailored to the patient. Propofol often causes apnea during induction and at times it is necessary to administer doxapram to stimulate the respiratory cycle for proper assessment of laryngeal movement. A summary of intravenous protocols is provided in Table 1.
Drugs used for respiratory endoscopy

In cases of upper airway obstruction (laryngeal paralysis or airway-associated masses), preparations should be made to provide for temporary tracheostomy if needed to allow appropriate recovery. In the case of absent ventilation following extubation, the animal should be re-intubated and mechanical ventilation provided.
Laryngoscopy procedure
Immediately on induction, a careful laryngeal examination should be performed, especially when there is clinical evidence of upper airway disease or obstruction. It is important that laryngeal function is evaluated under a light plane of anesthesia. Rigid telescopes are easier to maneuver within the caudal oropharynx and provide excellent illumination and magnification. It is essential to have an assistant announce the respiratory cycle to the clinician to allow monitoring for appropriate laryngeal movement (abduction of the arytenoid cartilages during inspiration). Paradoxical laryngeal motion can be mistaken for normal movement; therefore, it is critical to ensure that the abduction (outward movement of the arytenoid cartilages) corresponds to inspiration.
The assistant also monitors anesthesia throughout the procedure and assists with collection of airway samples. Rigid cup biopsy forceps or long (laparoscopic) Metzenbaum scissors can be used to obtain diagnostic samples of laryngeal tissue, which is fibrous and elastic in nature. Several samples from the lesion should be collected because concurrent inflammation can mask neoplastic infiltrates. Feline laryngeal neoplasia is not commonly reported in the veterinary literature; however, lymphoma and carcinoma of laryngeal tissue can be diagnosed via cytology or histopathology (Figure 4).

Laryngoscopy images showing a normal feline larynx (a) with a jet ventilator catheter traversing the laryngeal opening and (b) an obstructive carcinoma
Tracheoscopy and bronchoscopy procedures
Before an endoscope is placed into the airways, adequate depth of anesthesia is confirmed and the patient’s mouth is held open with a mouth gag to avoid inadvertent damage to the bronchoscope. Spring-loaded mouth gags should be used with caution due to the potential for extensive jaw opening to compress blood supply and cause cortical blindness in cats. 11
Several methods can be used to maintain oxygenation throughout the procedure. A long 16 gauge catheter can be placed down the trachea and attached to a jet ventilator. A sterile open-ended red rubber catheter can be passed to the mid-thoracic trachea and attached to low flow oxygen (<1 l/min). Finally, an endotracheal tube can be inserted for stabilization then removed for endoscopic evaluation. Pre-oxygenation, using either an endotracheal tube or anesthesia mask, can be used to increase the blood oxygen saturation prior to beginning or between procedures. The animal is prepared for appropriate cardiovascular monitoring, including pulse oximetry, direct or indirect blood pressure monitoring and electrocardiography.
Following anesthetic induction and laryngeal examination, topical anesthesia (one drop of 2% lidocaine or aerosolized 10% lidocaine) is administered to reduce the risk of laryngospasm associated with passage of equipment through the larynx. 12 Topical preparations containing tetracaine or benzocaine should be avoided in cats due to the risk of oxidative injury and subsequent methemoglobinemia. Care should be taken to direct the scope through the laryngeal aditus without causing excessive irritation to the arytenoid cartilages, laryngeal saccules or vocal folds. By raising and extending the neck, the trachea is straightened, allowing easier access to the lower airways.
The endoscope is advanced down the trachea while maintaining a mid-luminal view to facilitate evaluation of all mucosal surfaces. Normal mucosa appears pale pink to slightly yellow and blood vessels are generally apparent beneath the surface. The trachea can usually be quickly examined because tracheal collapse is a rare finding in cats compared with dogs.13,14 This allows the majority of the procedure time to be spent exploring the lower airways. A systematic approach to evaluation of the lower airways ensures that all are thoroughly examined, remembering that with a cat in sternal recumbency the anatomy will be reversed in relation to the operator’s orientation facing the animal (ie, the right hemithorax appears on the left side of the screen and vice versa). 15
The endoscopist must have a firm understanding of the airway branching pattern to perform a comprehensive examination (Figure 5). If location within the lower airways is unknown, the endoscope is retracted back into the trachea until the carina is reached to provide a landmark to regain perspective. Any lesions induced by the scope should be noted in the report to prevent misinterpretation as a sign of pathology.

Illustration of the feline bronchial tree. Courtesy of Dr Roberta Caccamo

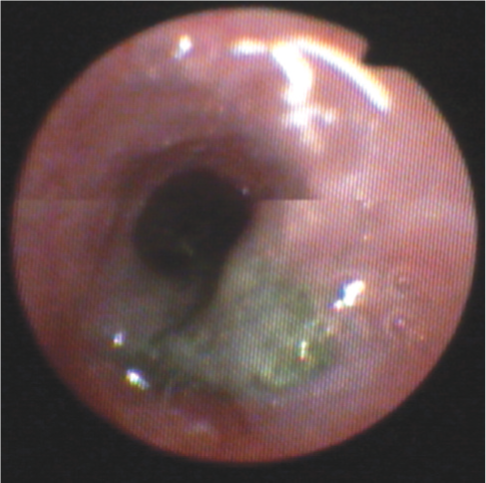
Bronchoscopic images showing a combination of gross findings including (a) airway collapse, (b) stenosis, (c) hyperemia and (d) mucus plugging. Unfortunately, gross findings correlate poorly with cytologic or histopathologic diagnoses

Endobronchial neoplasia is rarely identified in the cat. This is an image of a tracheal adenocarcinoma prior to debulking using an endoscopic snare. A catheter used for jet ventilation is in the foreground
Piece of gravel found within the trachea of a cat, which was removed using a three-prong grabber and basket retrieval forceps

Bronchoalveolar lavage
Prior to performing BAL, the endoscope should be withdrawn orally, the external surface wiped with saline-soaked sponges and the biopsy channel flushed with sterile saline to remove any airway material. The endoscope can then be reintroduced and advanced into the lower airways, taking care to avoid oropharyngeal contamination while maintaining a luminal view. This will minimize contamination of the endoscope tip and iatrogenic contamination of lavage samples.
BAL is performed by gently advancing the distal tip of the flexible endoscope deep into the terminal airways. Aliquot volume depends on the size of the endoscope and the size of the airway being occluded. In general, 3–5 ml aliquots of warm sterile saline are instilled at each lavage site up to a total of 10–20 ml per cat (total volume 2.5–5 ml/kg). 3 During BAL fluid collection, the tip of the endoscope should be agitated slightly to prevent adherence of the channel to the mucosal wall. If negative pressure is found during aspiration, pressure should be relieved temporarily and the tip of the endoscope should be withdrawn and repositioned before subsequent suction attempts.

BAL samples are collected via the endoscopic biopsy channel into a 20 ml syringe using hand suction. Alternatively, a suction trap can be employed to collect the sample for submission. Approximately 50–75% return of fluid should be anticipated.

Suppurative inflammation is characterized by either degenerate or non-degenerate neutrophils and is consistent with infectious or inflammatory airway disease. Such samples should be carefully scrutinized for the presence of organisms, although Mycoplasma species are rarely identified cytologically due to lack of a cell wall

Eosinophils can make up to 20% of normal BAL cytology in the cat. Excessive eosinophils (>20%) are suggestive of asthma or inflammatory airway disease

Foreign body removal
Though uncommon, foreign bodies have been reported in the lower airways of a small number of cats. Focal, persistent alveolar infiltrates increase the degree of suspicion for this differential, although radiographic changes are absent in up to one-third of cases. 9 If a foreign body is found or suspected, the endoscopist should evaluate each branch of the lower airways systematically for additional foreign bodies, paying close attention to areas of thick mucoid, purulent inflammation or bifurcations with proliferative lesions, although most foreign bodies in cats lodge at the trachea or carina. 9 Three-pronged grabbers, snares, and biopsy or alligator forceps can all be used to isolate material and withdraw it orally with the endoscope. After removing one foreign body, the site of implantation should be inspected for residual or additional material.
Postoperative care and potential complications
Following completion of bronchoscopy and BAL procedures, the cat should be re-intubated with an endotracheal tube and maintained on oxygen and gaseous anesthetic for 10 mins to restore oxygen saturation prior to recovery. Anesthetic recovery should take place in a quiet location to minimize stimulation and patient anxiety. Following extubation, flow-by oxygen can be useful if the patient tolerates the proximity of a mask or tube. General anesthetic monitoring and post-procedural monitoring are continued until the animal is fully recovered from the procedure. It is not uncommon for crackles to be ausculted at the site of lavage for 4–12 h after the procedure; however, respiratory distress is generally not encountered.
The most significant complication encountered post-procedure is airway obstruction. This may be caused by inflammation and obstruction of the upper airway (resulting from biopsy or a pre-existing lesion), accumulation of pharyngeal secretions, or severe bronchoconstriction exacerbated by the procedure. In cases where obstruction due to upper airway inflammation is anticipated, dexamethasone (0.05–0.2 mg/kg IV) can be administered prior to extubation. Additional doses of terbutaline (IM or SC) can be considered when significant bronchoconstriction is encountered, as evidenced by reduced hemoglobin saturation with oxygen after BAL.
Key points
Airway endoscopy with bronchoalveolar lavage (BAL) can provide crucial diagnostic information and, when combined with clinical history, physical examination and thoracic radiographs, offers a complementary assessment of the upper and lower airways of cats.
Bronchoscopic evaluation provides several advantages over blind BAL sampling techniques including the ability to visually obtain directed lavage samples and to perform other diagnostic and therapeutic procedures.
With appropriate case selection, anesthetic monitoring and training, laryngoscopy, tracheoscopy and bronchoscopy are rewarding additions to a clinician’s diagnostic armamentarium.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.