
Abstract
Practical relevance:
Endoscopic examination of the feline gastrointestinal (GI) tract is a minimally invasive method for obtaining biopsy samples of the GI mucosa, which is often necessary for a diagnosis of chronic GI diseases. In addition endoscopy has several therapeutic indications including foreign body retrieval, oesophageal stricture dilation and placement of a percutaneous gastrostomy tube.
Clinical challenges:
Initially, practitioners must learn the subtle manipulations necessary to efficiently guide the endoscope through the GI tract to obtain biopsy samples of high diagnostic quality, and develop skills for implementing interventional procedures (eg, foreign body removal). Another challenge in mastering GI endoscopy is the ability to recognise normal from abnormal, which requires many years of practice and experience. Endoscopy is a diagnostic and interventional procedure that should be performed only in conjunction with a thorough history, physical examination, appropriate laboratory evaluation, and radiographic and/or ultrasonographic imaging.
Audience:
This review is intended to familiarize both the general and referral practitioner with GI endoscopy as a minimally invasive diagnostic and therapeutic intervention for the feline patient.
Evidence base:
The guidance contained within this article is based on a combination of the published literature, the authors’ personal experience and the experience of colleagues.
Role of endoscopy in GI disease
Nowadays, flexible endoscopy is a routine procedure in the diagnostic work-up of cats with gastrointestinal (GI) signs, such as retching, regurgitation, vomiting or diarrhoea, albeit one that should be used only after less invasive procedures have failed to yield a final diagnosis. The results of abdominal palpation, haematology, biochemistry (including plasma thyroxin levels, trypsin-like immunoreactivity and vitamin B12 levels), complete faecal analysis (including Giardia species and Tritrichomonas foetus) and, as in all sick cats, feline leukaemia virus and feline immunodeficiency virus testing should always be assessed. Appropriate diagnostic imaging such as plain or possibly contrast radiographs and, most importantly, abdominal ultrasound should also contribute to a full GI system evaluation.
It is important to be aware that endoscopy has some major limitations in the investigation of many GI problems. Motility abnormalities, functional diseases (dietary hypersensitivity, antibiotic-responsive disease, etc), lesions outside the GI tract (liver, pancreas, etc) or even submucosal disease cannot be visualised endoscopically; nor is it possible to investigate the entire GI tract with flexible endoscopes currently available.
If the indications are well chosen, however, the equipment is appropriate for the patient, and the clinician is experienced in the procedure, endoscopy can not only help to diagnose many diseases in the oesophagus, stomach and intestine, but may even help to treat some problems minimally invasively.
Flexible GI endoscopy has the major advantage over exploratory coeliotomy of allowing one to precisely access areas of pathology and take multiple biopsies from these areas in a minimally invasive manner. There are rarely complications associated with wound healing or dehiscence (particularly in cats with low serum protein concentration) and thus animals can be treated immediately with immunosuppressive drugs, especially steroids.

Oesophagoscopy
Overall, oesophageal diseases are uncommon in cats and represent about 0.05–1% of all admissions in a referral situation.1,2 Common clinical signs that might necessitate an oesophagoscopy are retching, dysphagia, regurgitation and possibly ptyalism; it should be remembered, however, that differentiating vomiting from regurgitating in cats can be difficult and is often not possible for owners.
Plain radiographs of the thorax should always be obtained in cats with these clinical signs and may diagnose a radiodense foreign body or gas/distension around a possible non-radiodense foreign body, megaoesophagus, gastro-oesophageal intussusception 3 or mediastinal mass. Contrast radiographs with liquid contrast (iodine-based or barium) or contrast agent mixed with food might be indicated in some cats and several abnormalities such as a stricture, radiolucent foreign body, vascular ring anomaly, gastro-oesophageal intussusception or tumour can be diagnosed with this modality. A swallow study (fluoroscopy) is needed to diagnose functional oesophageal motility problems, which can occur in cases of dysautonomia or dystrophic myopathy, or may be idiopathic. 2
If the problem cannot be diagnosed by these various means, endoscopy may be indicated and is the only modality that will diagnose oesophagitis.
Possible abnormalities found during oesophagoscopy are summarised below. The exact location of an oesophageal lesion is difficult to ascertain unless it is directly over the base of the heart where pulsation of the aorta can be seen. To record abnormal findings, the distance from the upper incisors should be ‘guesstimated’ based on the length markings on the endoscope.

Mucosal erythema, irregularity, erosion and ulceration indicate an oesophagitis (Figure 1).
A stricture is characterised by a circumferential narrowing, commonly in the exact centre of the lumen, which cannot be passed (Figure 2). It is important not to confuse this with difficulties in passing the cardia, which might be a problem in some cats.
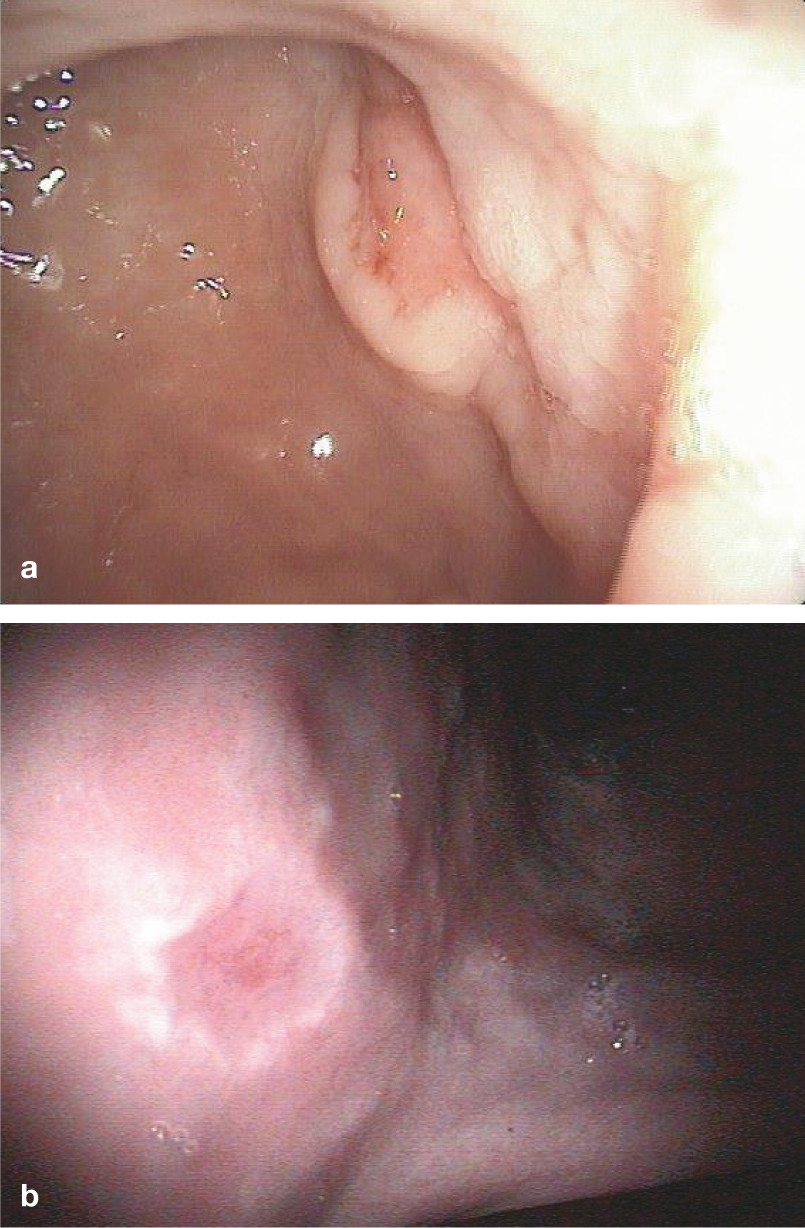
Tumours of the feline oesophagus are rare. They mostly present as masses protruding into the lumen (Figure 3), which tend to be ulcerated and friable. Sometimes oesophageal lymphoma may appear simply as a very irregular mucosa with a ‘cobble-stone’ appearance.
Foreign bodies (Figure 4) are readily diagnosed and can often be removed endoscopically (discussed later).
An extraluminal compression can be due either to a mass in the mediastinum (lymphoma, cyst, thymoma) or a vascular ring anomaly (eg, persistent right aortic arch). While, in the former, bulging of the mucosa with cranial dilation is visualised, the latter often has a typical band crossing the oesophagus with a cranial diverticula (Figure 5).
Protrusion of gastric rugal folds into the oesophagus is the hallmark of a gastro-oesophageal intussusception.
Generalised dilation of the entire oesophagus is the definition of a megaoesophagus and is a rare finding in cats. This problem, which might be secondary to dysautonomia or myasthenia gravis, is commonly diagnosed on plain or contrast radiographs. Oesophagoscopy is rarely indicated and may even be contraindicated due to the high risk of aspiration pneumonia during induction or recovery from anaesthesia. A dilated oesophagus during air insufflation is difficult to differentiate from a dilated oesophagus due to a megaoesophagus. Froth, fluid and fermenting food might be seen in megaoesophagus, together with signs of oesophagitis. Furthermore, it might be difficult to pass through the lower oesophageal sphincter as the endoscope might be diverted into some blind-ending folds, or a diverticulum.

Oesophagitis in an 11-year-old domestic shorthair cat with a history of 2 months of vomiting and pre-treatment with longacting dexamethasone

Oesophageal stricture in a 1-year-old cat 4 weeks after clindamycin tablet administration

Adenocarcinoma of the oesophagus in a 6-year-old domestic shorthair cat with a 3 week duration of regurgitation

Blood clot in the oesophagus of a cat with marked oral bleeding

Endoscopic view of the oesophagus of a 1-year-old cat with persistent right aortic arch. A band compressing the lumen from the outside can be seen from the 6 o’clock to 2 o’clock position in a clockwise rotation

Gastroscopy
The most common indication for gastroscopy is chronic vomiting for which a diagnosis cannot be achieved with laboratory or diagnostic imaging methods and therapeutic trials. Acute vomiting is rarely an indication unless a foreign body is suspected and requires immediate intervention, or there is severe haematemesis which is unresponsive to medical management. Other indications for gastroscopy in cats might include undiagnosed weight loss, anorexia, nausea/ptyalism or melaena.
In the normal stomach, rugal folds, which run in parallel towards the antrum, are easily distended with air. The endoscopist should be careful to avoid overdistension, which is not an uncommon problem.
The most common abnormalities seen during gastroscopy are foreign bodies (including trichobezoars, Figure 6), and irregular mucosa (petechial haemorrhage, erosions, friable, cobble-stone appearance) (Figure 7). Ulcers (Figure 8) are also seen, but are rare in cats. 4 Food in the stomach >12 h post-feeding indicates a motility problem. This might be a primary pathology, but is more commonly identified secondarily to gastritis or other inflammatory GI conditions.

Gastroscopic views of foreign bodies. (a) Ear plug in the stomach of a 2-year-old Maine Coon cat. (b) Trichobezoar in the antrum of a 15-year-old cat

Irregular mucosa with cobble-stone appearance in the greater curvature of a 10-year-old domestic shorthair cat. In the background, towards the 3 o’clock position, the entrance to the antrum can be seen. The cat had histologically marked lymphoplasmacytic gastritis
(a) Typical ulcer with rim can be seen (2 o’clock position) close to the entrance to the antrum (towards the 11 o’clock position). Lymphoma was diagnosed by histology. (b) Small ulcer in the incisura angularis (top towards fundus, bottom towards antrum), which proved histologically to be an adenocarcinoma
Acute gastritis in cats can be due to ingestion of plant material, drugs (eg, non-steroidal anti-inflammatory drugs [NSAIDs], steroids, antibiotics), dietary indiscretion, ‘stress’ or any severe disease and hypotension. Normally endoscopy of the stomach in these patients is not necessary and symptomatic therapy with a proton pump inhibitor, sucralfate, an antiemetic drug and dietary management is all that is required. 5 The endoscopic appearance in cases of acute gastritis might be completely normal, or might show petechial bleeding and erosions, especially in the antrum (Figure 9).

Acute gastritis with severe bleeding in a 12-year-old domestic shorthair cat with vomiting and an invasive cutaneous adenocarcinoma
Masses in the stomach can either be benign, such as polyps (Figure 10), or malignant, most commonly lymphoma. While the former generally are smooth and small, and the latter is often associated with irregular, potentially ulcerated mucosa, and can be of variable size, only a histological examination can differentiate benign from malignant masses.

Gastric polyp (arrow) in the antrum of a 6-year-old domestic shorthair cat with chronic vomiting
Duodenoscopy
Duodenoscopy is mostly performed as part of an upper GI endoscopy procedure – oesophagogastroduodenoscopy. Besides those indications already mentioned under gastroscopy, chronic diarrhoea, weight loss, abdominal pain and thickened bowel loops on physical examination are common presentations for which duodenoscopy is indicated in cats. Like all endoscopic procedures, duodenoscopy should only be performed if other procedures have not provided a diagnosis or improvement in clinical signs.
Potential abnormal findings are inflamed mucosa with increased friability, granularity/areas of focal bleeding (Figure 11a), mass, foreign body, ulcer (Figure 11b), intussusception and parasites. Unfortunately, there is often a marked discrepancy between the macroscopic appearance and final histological diagnosis – underlining the critical importance of collecting biopsies during all endoscopic examinations. Differentiation between lymphoplasmacytic IBD and small-cell lymphoma is difficult and should be confirmed by immunohistochemistry. 7

Bleeding (a) and ulcerations (b) in the duodenal mucosa. Note intestinal peristalsis and narrowing of the distal lumen in (b)
Intestinal parasites should not be seen in a patient treated with appropriate anthelmintics prior to undergoing endoscopic examination. Nevertheless, both roundworms and tapeworms can be encountered and typically try to move away from the endoscope tip.
Colonoscopy
Large intestinal disease in cats commonly results in large bowel diarrhoea or constipation. It must be remembered that vomiting is another frequent complaint in cats with large bowel disease. 8 Furthermore, haematochezia can be due to local problems in the large intestine or anorectal disease, and must be differentiated from generalised coagulopathies. Once again, a thorough investigation for systemic disease is warranted for all these problems, including haematology, biochemistry, coagulation testing, faecal analysis (sedimentation, ELISA, PCR, fungal culture) and diagnostic imaging.
In cats with constipation the most common aetiologies are idiopathic megacolon (62%), pelvic canal stenosis (23%) and neuropathies (6%) 9 – none of which require colonoscopy for a diagnosis. Nerve injury, Manx cat sacral nerve deformity, dysautonomia, perineal hernia, intestinal foreign bodies, dietary indiscretion/hypersensitivity, anal, rectal or colonic atresia and prostatic diseases are other, rare causes of constipation/obstipation in cats, which can generally be diagnosed without endoscopy.
The commonest large intestinal disease in cats is some form of colitis. This can be limited to the colon or may be part of IBD of the entire intestinal tract. As mentioned earlier, macroscopic appearance can range from fairly normal to markedly irregular, with friable thickened mucosa and lymphoid hyperplasia (Figure 12). This can undoubtedly be grossly mistaken as neoplasia; thus it is essential to collect an adequate number of biopsies and not to overinterpret the gross visual picture.

Bleeding colon in a 10-year-old domestic shorthaircat with signs of large bowel diarrhoea. Histologically, a moderate lymphoplasmacytic infiltration was seen
Colonic tumours, especially lymphoma, can look identical to inflammatory colitis and must be differentiated by histopathology, and often immunohistochemistry, for definitive diagnosis. Other large intestinal tumours in cats include adenocarcinoma and leiomyosarcoma, both of which are more focal and often invade the lumen, producing an irregular proliferative appearance (Figure 13). Obtaining diagnostic biopsies might be difficult in both as superficial samples will often only reveal inflammation.
Irregular mass in the colon of a 13-year-old Abyssinian cat with haematochezia, which proved to be an adenocarcinoma
Other rare findings in cats include ileocolic or ileocaecal intussusception (often diagnosed by ultrasound prior to endoscopy) and rectal stricture.

Foreign body removal
Due to their fastidious eating behaviour, GI foreign bodies are much less common in cats compared with dogs. Nevertheless, a variety of objects can be found in the oesophagus, stomach (Figure 6) and intestine. Endoscopy for foreign body removal from the oesophagus and stomach is approached in an identical manner to diagnostic endoscopy. Before the procedure is initiated, however, the endoscopist must evaluate if the procedure can be performed successfully by assessing the type (sharp ends, needle, ball) and size of the foreign object, the available retrieval instruments, as well as their own experience. Various foreign bodies can rarely be removed endoscopically (see box) and, certainly, it is clinically unwise to make a prolonged attempt to retrieve an object that could be removed via exploratory surgery (potentially without even opening the stomach) in a fraction of the time.

In general, however, endoscopic foreign body removal is much quicker than surgery in the hands of an experienced clinician, requiring normally less than 30 mins from the point of anaesthesia induction. Other advantages of endoscopy over surgery are minimal invasiveness and rapid discharge from the clinic. Owners must be made aware of potential complications (unsuccessful procedure, oesophageal perforation) and thus should provide consent for surgical intervention during the same anaesthesia in these cases. In cats with severe oesophagitis following foreign body removal, placement of a temporary gastrostomy feeding tube should be strongly considered (see later) and ideally should be discussed with the owner prior to performing the procedure.
Foreign body removal instruments can either pass through the working channel or are pushed alongside the endoscope. Rat tooth forceps, alligator forceps (Figure 14), multi-prong forceps, basket forceps and snares are available for 2.8 mm working channels and most of them for 2.0 mm working channels. While it is not necessary to have all of these instruments available, with one type of prong and one type of grasper many objects can be successfully removed.

Foreign body retrieval instruments that can be used through the working channel of a flexible endoscope: rat tooth forceps (a) and serrated-edge alligator forceps (b). ©2013 Courtesy of KARL STORZ GmbH & Co KG
The choice of instrument lies mainly in the hands of the endoscopist and sometimes different instruments will need to be tried to grasp the object satisfactorily. It is of paramount importance that no foreign object is ever pulled into the working channel of the endoscope and that the endoscope is not damaged by the prongs if they are used alongside the insertion tube. Foreign body prongs used in this way have a much better gripping strength, with the endoscope used solely to visualise the object. These must be small enough to pass alongside the endoscope without traumatising the cat’s oesophagus.
A very long and sturdy instrument has recently become commercially available and may help ease the removal of more complicated foreign bodies (Figure 15). Other instruments that can be used in a similar manner are laparoscopic grasping forceps. A plastic overtube (eg, old endotracheal tube cut to size) can help to protect the mucosa and endoscope during the removal of sharp and pointed objects (eg, needles, fish hooks). The endoscope is introduced through the tube and the object is pulled into the lumen of the tube. The endoscope, object and tube are then removed as one unit.

Foreign body grasping instrument (length 60 cm) that is used alongside the endoscope for retrieval of bones and other large objects. ©2013 Courtesy of KARL STORZ GmbH & Co KG
Oesophageal foreign body
Cat owners will often be aware of the possibility of an oesophageal foreign body causing clinical signs such as retching or gagging. Since needles and fish hooks may still have thread or line attached, careful sublingual inspection should be performed during the clinical examination. The thread or line should never be cut until the foreign body has been removed, irrespective of the technique used. Thoracic radiographs must be carefully inspected for pneumomediastinum and/or fluid accumulation indicating potential oesophageal perforation.
Foreign body removal is approached in a similar way to diagnostic oesophagoscopy. The cat is placed in left lateral recumbency so that the oesophagus is positioned above the aorta. A careful inspection of the mucosa for potential foreign body-related injury is undertaken during air insufflation. In the case of a perforated oesophagus, respiratory compromise may occur and should be anticipated. Once the foreign body has been visualised it should be gripped firmly with a foreign body grasper or forceps. Pointed objects are initially pushed aborally to dislodge them from the mucosa and then the pointed tips are grabbed and pulled towards the endoscope. While some traction is needed, force should never be used to remove a foreign object. Careful rotational torque may help to dislodge bony objects. If a foreign body grasper is used alongside the endoscope, the endoscope should first be withdrawn. Rarely, the foreign object is lost just before passing the upper oesophageal sphincter – in these cases it is best to remove the object with a long curved grasping forceps under laryngoscopic control.
After removal, the oesophagus should be inspected for mucosal damage caused by lodgement of the object and/or its removal. Moderate to marked oesophagitis is treated with oral liquid sucralfate; steroids are most likely not helpful. In severe cases a gastrotomy feeding tube should be considered.
Gastric foreign body
Foreign objects are uncommon in the stomach of cats. While not all such foreign bodies are the cause of clinical signs, and some may be incidental findings during diagnostic imaging, gastric foreign bodies normally require removal. Immediately after induction of anaesthesia, and just before endoscopy, a control abdominal radiograph should be taken to ascertain that the object has not moved into the small intestine.
While endoscopy for gastric foreign body removal is started in left lateral recumbency, it may be necessary to rotate the cat to dorsal or even right lateral recumbency should visualisation or grabbing of the object be difficult. This is commonly the case when the object lies in the fundus directly adjacent to the cardia; due to the small size of the feline stomach, the endoscope sometimes bypasses the object and grabbing is not possible when the animal is positioned on its left side.
The object dictates the type of removal instrument used. Sharp objects are removed as discussed above for oesophageal foreign bodies – a rubber tubing sleeve over the endoscope can assist with retrieval and protect the mucosa of the stomach and oesophagus from lacerations. Stones or rubber objects (both rare in cats) are grabbed with a basket or prong forceps. Pulling them through the cardia may be difficult – it is easiest to have the object as close to the endoscope as possible. Pulling both as a single unit slowly, with intermittent/simultaneous insufflation, will eventually assist in removal.
Duodenal foreign body
It is very uncommon to be able to grab and remove foreign bodies from the duodenum in cats. These objects need surgical removal as many complications are possible, such as perforation and intussusception. Duodenal foreign bodies may also be simply too large or too out of reach to properly grasp for safe removal.
Stricture dilation
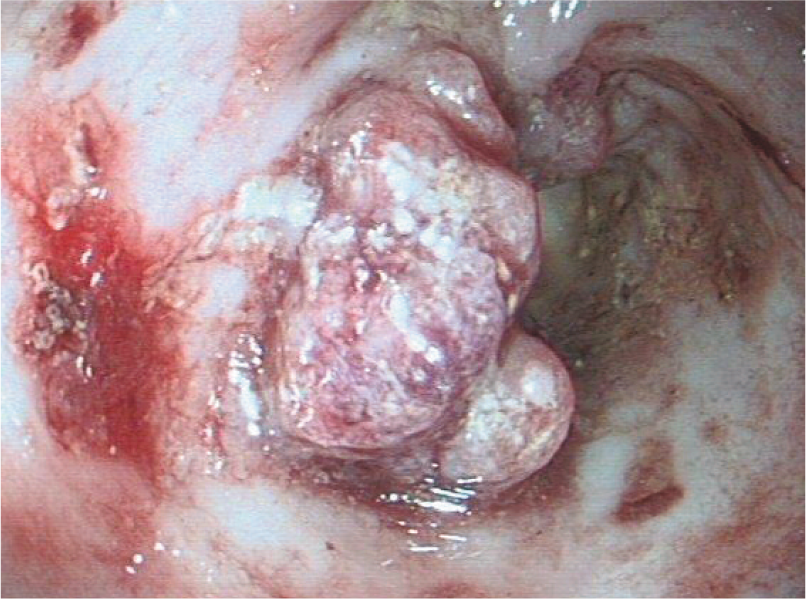
Once inflammation of the oesophagus extends deeply enough into the muscularis mucosa, healing may result in intramural fibrosis and subsequent stricture formation (Figure 2). In cats, the most common underlying causes are potentially ulcerogenic drug formulations (eg, doxycycline and clindamycin) and their retention within the oesophagus, and foreign body trauma (eg, trichobezoar). Reflux during anaesthesia or ingestion of caustic substances as a cause of oesophageal stricture is a very rare finding in cats. While bougienage has been described to dilate oesophageal strictures, this has largely been replaced by balloon catheter dilation. 14 This procedure, which involves dilating a balloon within the stricture to cause stretching and tearing, is quick and safe, resulting in few complications if performed carefully.
Used cardiac balloon catheters are cheap and very effective. In cats, the required length is commonly 6–10 cm, and diameter 1.0–1.2 cm (Figure 16a). Under endoscopic control, a guide wire is first placed through the stricture and the balloon catheter is then passed over the wire along the endoscope into the stricture. There are balloon catheters available that can be used through the working channel of the endoscope; however, these are expensive and for single-use only. Once within the stricture, the endoscope is withdrawn a few centimetres, and the balloon is inflated with water (better than air) via a syringe or pump connected to a pressure gauge. Once the pressure that is permitted for the particular balloon has been reached (Figure 16b), the balloon is kept in place for 1–2 mins and then deflated. Endoscopic visual inspection after the procedure should reveal some tears and bleeding (Figure 17). If these signs are not visible, either the dilation was not wide enough or the balloon slipped, and the procedure must be repeated.
(a) Balloon catheter (length 4 cm, inflated to width 10 mm). (b) Manometer for use during balloon dilation of oesophageal strictures. Images courtesy of Dr M Schneider, Small Animal Clinic, University of Giessen, Germany

Tear in the oesophageal mucosa after balloon catheter dilation
To prevent re-stricture formation, the procedure is repeated twice weekly until there is no significant stricture visible endoscopically. Re-dilation when regurgitation recurs is another approach, albeit often less successful in the long run.
After balloon dilation, the cat is treated for severe oesophagitis with oral liquid sucralfate, a proton pump inhibitor, an antiemetic drug and soft food. There are no studies showing that prednisolone will help to prevent stricture formation. In severe cases, endoscopically guided intralesional injection of triamcinolone (0.4 mg/kg) into the cranial edge of the stricture until a bleb is formed is probably more justified. In cats with moderate tears of the oesophagus, placement of a gastrostomy feeding tube might be considered. Major, life-threatening tears are a rare occurrence (4–9%) and will result in mediastinitis and potentially tension pneumothorax. Surgical repair is needed but carries a risk of further stricture formation.
In cases with recurrent stricture formation despite frequent re-ballooning (>10 times), placement of an expandable stent can be considered (Figure 18).10,11 Unfortunately, there are so far no biodegradable stents for cats available for the oesophagus and complications of permanent stents, such as aboral migration, pressure necrosis and occlusion by hair or food, are serious risk factors to consider and discuss with the owners.
Metallic stent in the oesophageal lumen of a cat in which balloon catheter dilation of a stricture was unsuccessful. Reproduced with permission from Glanemann et al (2008)10
PEG tube placement
Feeding is paramount in sick and debilitated patients and enteral feeding is preferred as it improves enterocyte health and decreases bacterial translocation from the GI tract. 15 While force-feeding and use of naso-oesophageal feeding tubes may be ideal in the short term, neither generally allow adequate caloric intake in severely sick patients and feeding may even be impossible in cats with anatomical or functional problems of the oral cavity or oesophagus. Percutaneous endoscopic gastrostomy (PEG) tubes have multiple advantages inasmuch as commercial food and special diets for specific diseases (eg, chronic kidney disease, liver problems) can be administered, the daily caloric requirement is easily met, most oral drugs can be given through the tube (avoid crushing tablets with coating to resist gastric acidity) and the time required for feeding is much reduced, not only in a hospital setting but also at home. The major drawback of PEG tubes is the cost of the tube (especially commercial kits) and of the endoscopic placement.

PEG tubes can be placed during laparotomy, when the cat undergoes this procedure for other causes, or blindly (eg, using an Eld applicator). The safest and probably quickest procedure (5–10 mins in experienced hands with commercial kits), however, is endoscopic placement.
Types of PEG tubes
There are two types of PEG tubes available: commercial kits (from human medicine), which contain all materials for quick placement, and ‘home-made’ kits, which are cheaper but more cumbersome and, therefore, time-consuming. A third type of tube, the so-called low-profile PEG tube (or ‘button’), is available as a replacement for the initial tube or to be placed from the outset – but there is hardly any experience with these in cats so far.
Commercial kits
Commercial PEG tubes are made of either silicone or polyurethane and can withstand gastric acidity for the animal’s lifetime. In cats 16–20 Fr size is used. The inner flange is different between different brands but all are suitable for cats. The commercial kits contain – besides the feeding tube with conical end – the following materials, which are also needed in ‘home-made’ kits: large over-the-needle catheter (16 G), double looped strong suture material (long enough to extend from mouth to side of abdomen, ie, 70–100 cm), scalpel, material to fix the feeding tube on the outside (clips or suture) and an adaptor for the feeding syringe (Figure 19).

Components of a commercial human PEG tube set (Freka), 15 Fr size, which can be easily used in the cat
Home-made kits
Home-made kits for PEG tubes include mushroom tip catheters, commonly Pezzer urinary catheters. With a pipette tip, a needle and a strong suture material as a guide wire a similar device as the commercial PEG tube is created (Figure 20). 13

(a) Materials used for a ‘home-made’ PEG tube using a Pezzer urethral catheter. (b) Part of the catheter is used as an inner flange. (c) A pipette tip is used as a conical dilator and threaded over the catheter. (d) The thread of the catheter is attached to the thread exiting the mouth. (e) The PEG tube is secured to the body wall using Chinese finger-trap sutures
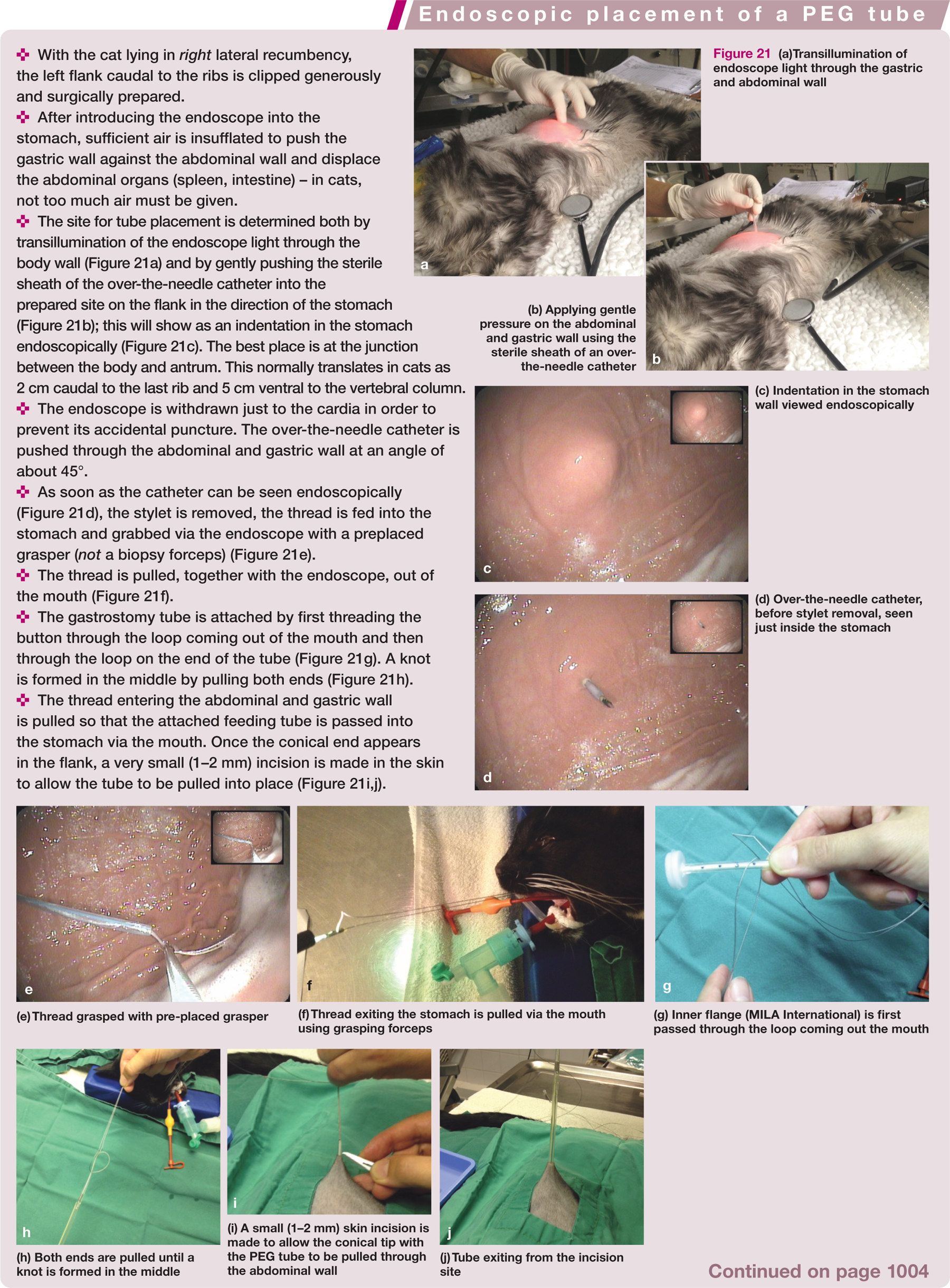

(a)Transillumination of endoscope light through the gastric and abdominal wall
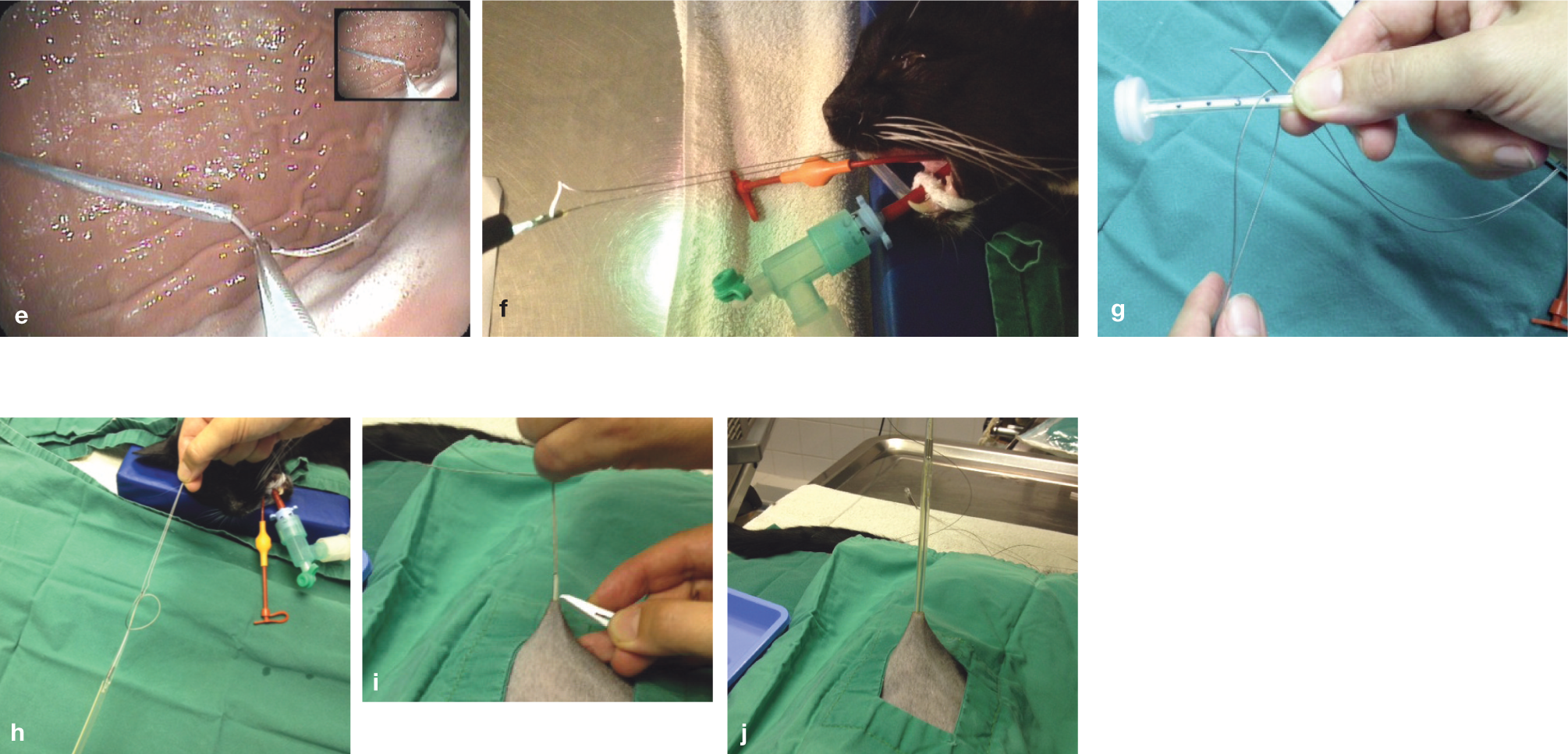
(e) Thread grasped with pre-placed grasper
(f) Thread exiting the stomach is pulled via the mouth using grasping forceps
(g) Inner flange (MILA International) is first passed through the loop coming out the mouth
(h) Both ends are pulled until a knot is formed in the middle
(i) A small (1–2 mm) skin incision is made to allow the conical tip with the PEG tube to be pulled through the abdominal wall
(j) Tube exiting from the incision site

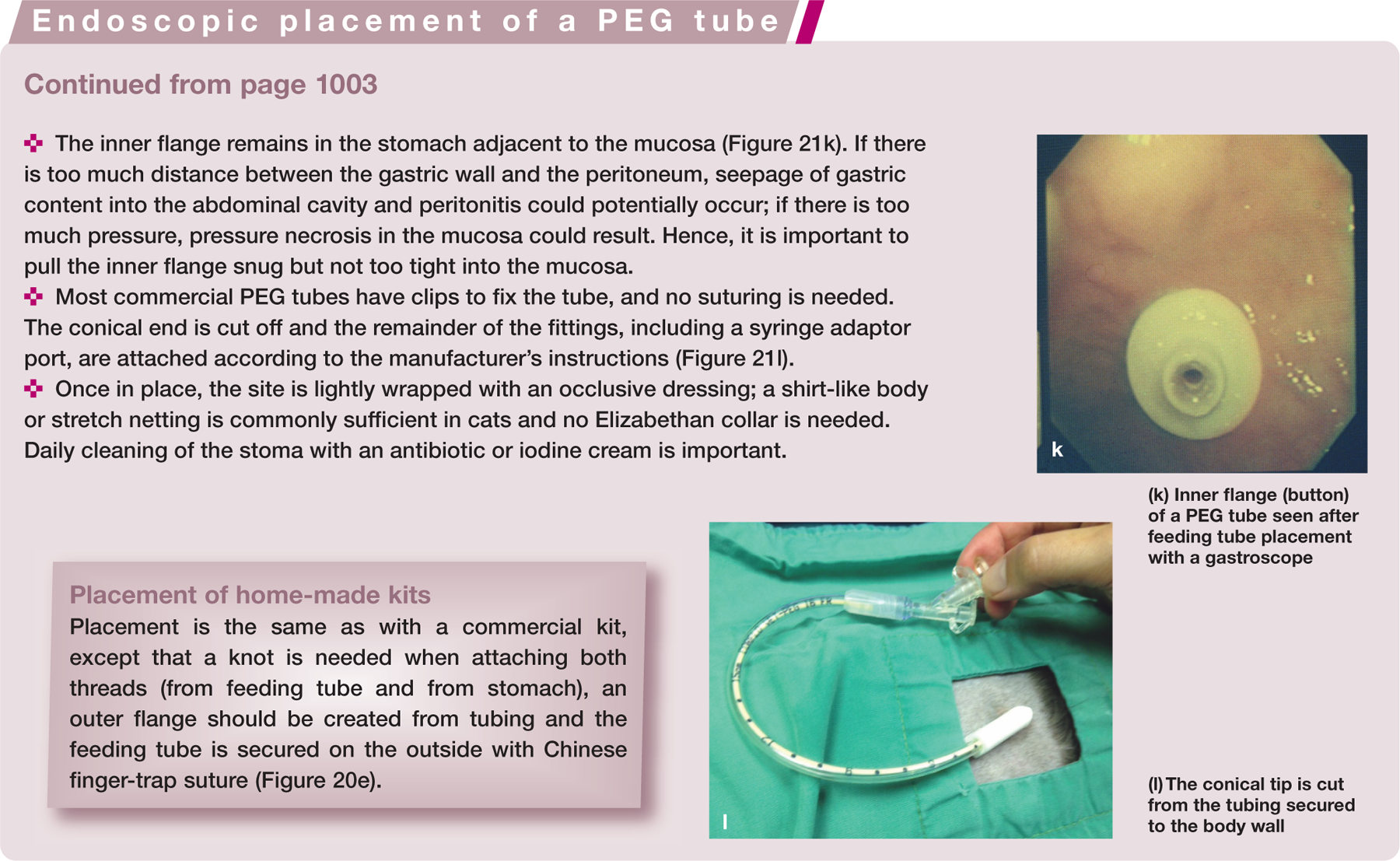
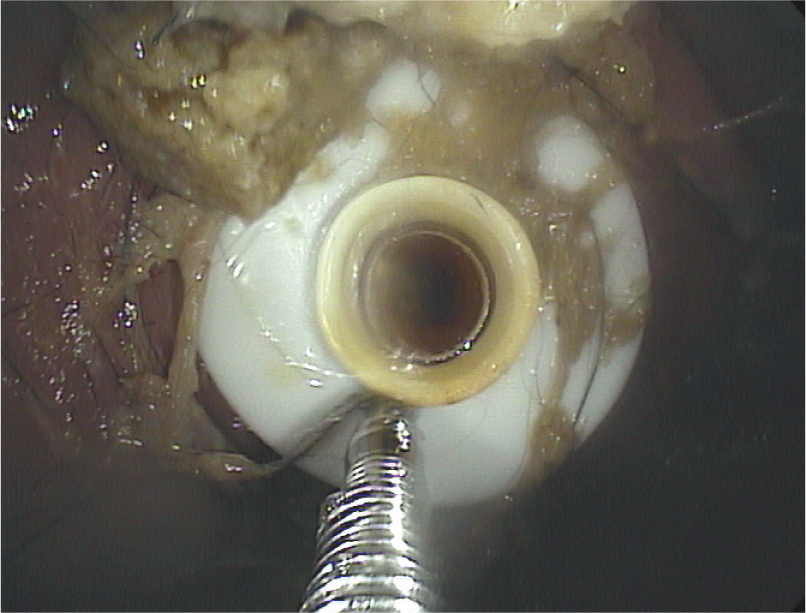
(k) Inner flange (button) of a PEG tube seen after feeding tube placement with a gastroscope
PEG placement
With both types of kit, placement is approached in the same way – a thread or suture material is pushed via a needle through the abdominal and gastric wall into the gastric lumen, grabbed endoscopically and pulled via the oesophagus through the mouth. The PEG tube is then attached and pulled via the thread into place. The procedure is described on page 1003 and above.
If biopsies are needed, these should be taken before PEG tube placement.
PEG tube feeding
Feeding can commence 24 h after tube placement, initially with one-half of the daily calorie requirements. After 1 day, the full amount can be given. In the first few days the cat is given five or six meals daily, but as early as day 4 or 5 feeding can be reduced to three meals daily. While problems with PEG tube feeding are rare, they can arise and should be dealt with according to established guidelines. 15
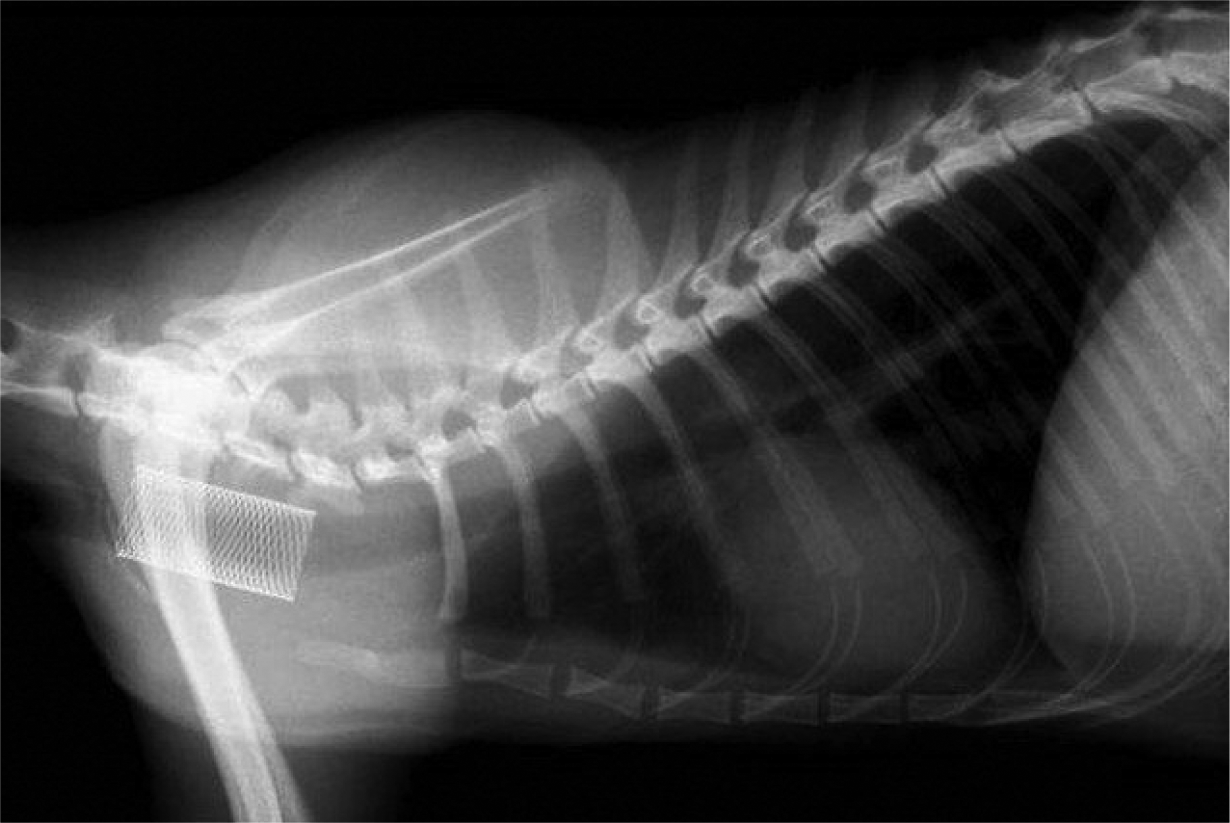
PEG tubes can stay in place for many months, even lifelong. Replacement with low-profile devices (buttons) can be considered. It is important, however, to leave a new PEG tube in place for a minimum of 7 days, and in animals with wound healing disorders, even longer (up to 21 days) in order for proper stoma formation. Tube removal in cats should always be carried out endoscopically as the inside flange of commercial kits is too big to pass naturally when the tube is cut on the outside (Figure 22).
PEG tube removal endoscopically once the cat is eating again. The tube is clipped on the outside once it is safely grabbed with foreign body retrieval instruments on the inside
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.