
Abstract
Practical relevance:
For many years, endoscopy and minimally invasive surgery have been considered ‘standard’ in human healthcare. With the expansion of the used medical equipment market, and the falling cost of new equipment, veterinary practitioners are now starting to appreciate first-hand the benefits of performing endoscopic procedures: for example, vastly improved visualisation of the surgical site, reduced tissue trauma, minimal postoperative pain and faster recovery times, especially in feline patients. In addition, clients almost always choose a less invasive procedure if the capabilities are present, and will often consent to these procedures sooner than they would to conventional surgery.
Aim:
This article aims to guide the general feline practitioner towards a basic understanding of endoscopic and ancillary equipment, and in the direction of appropriate training required to perform routine endoscopic procedures.
Evidence base:
The authors draw on information provided in a combination of published texts, articles, reviews and their own clinical experience to provide a practical information guide for the clinician interested in feline endoscopy.
The decision to buy: key investments
The decision to offer an endoscopy service will usually depend, among other things, on practice demographics, staffing, practitioner interest, and relative proximity to practices offering similar services. Two further key considerations concern the required investments in training and in equipment.
Investment in training
Once the decision has been reached to purchase an endoscope, either flexible or rigid, every effort should be made to become proficient in its use. Initially, the learning curve can be relatively steep and at times frustrating, especially in smaller feline patients in a private practice setting. Endoscopy courses will often be advertised through veterinary teaching hospitals, private continuing education companies, conferences and endoscope companies. The authors advise looking for courses that offer at least several consecutive days of formal practical training. Although single-day courses may provide adequate introductory level experience, there is simply not enough time to gain the necessary endoscope handling skills needed for feline endoscopy.
For flexible endoscopy, practical training should include proper handling techniques, learning how to ‘drive the scope’ through the upper gastrointestinal tract smoothly and efficiently, subtle techniques needed for traversing the pyloric canal and intubating the pylorus, colonoscopy and ileoscopy, biopsy techniques, and foreign body retrieval. For rigid endoscopy, training should include instruction on the safe handling of instrumentation and techniques for atraumatic entry into the nose, bladder, abdomen and thorax. Anaesthetic considerations and the use of ancillary aids such as electrosurgery should also be covered and practical exercises in instrument handling using a laparoscopic trainer form the basis of the manual skills necessary to perform any endoscopic procedure.
With training, practice and persistence, these skills will become easier, more time-efficient and profitable for the clinic. In the beginning, new endoscopists should allow for long procedure times, and avoid booking too many other cases on chosen endoscopy days. This will provide a more forgiving setting in which to become comfortable and proficient in performing basic endoscopic examinations and procedures. In addition, initial case selection for the beginner endoscopist should favour a successful outcome and thus increase operator confidence. For example, gaining confidence with uncomplicated gastric foreign body removal in a large dog is advisable before attempting ileocolic intubation in a juvenile cat with chronic small bowel disease.
The most important part of the learning curve in endoscopy is the ability to recognise normal from abnormal. This often requires many years of experience. As is the case with successfully mastering any technical procedure, if proper skills and sample procurement are underdeveloped, even the most sophisticated endoscopes will offer very little value and diagnostic reward. With practice and dedication, however, most committed practitioners can become skilled in routine endoscopy in a relatively short period of time.
Investment in equipment
For the feline practitioner, the selection of appropriate equipment will depend on its intended use, durability and financial outlay. Beyond expense, consideration must be given to the probability and frequency of usage, and versatility of the equipment.
All too often, a lower purchase price is ranked above quality and intended use when making purchasing decisions! This can result in an empty investment, as even the most skilled endoscopists would find performing a complete and diagnostically accurate examination difficult using an inappropriately sized or poor quality endoscope. For example, in gastrointestinal endoscopy, careful thought must be given to the insertion tube diameter and length of the gastroscope. A cheap 12.8 mm x 100 cm human colonoscope would be relatively useless for feline upper and lower gastrointestinal procedures due to the high risk of serious iatrogenic damage to the oesophagus, stomach/pylorus and colon. Great care must be exercised at all times when traversing a cat’s narrow pylorus, as possible perforation is a real risk. Therefore, veterinarians purchasing their first endoscope should consider a single, high-quality endoscope that may be used for both upper and lower gastrointestinal endoscopy in cats and small dogs (see later).
The decision as to whether to purchase new or secondhand and, if the latter, what to be aware of, is discussed later. Advice should always be sought from an experienced endoscopist or veterinary endoscopy company as to the minimum range of equipment that will be required for the procedures that the practitioner anticipates performing in the practice.
Types of endoscopes
Flexible endoscopes
Flexible endoscopes are often used for examining hollow, tubular structures with convoluted and tortuous paths (ie, gastrointestinal system, respiratory tract and male urinary tract). Flexible endoscopes may be subdivided into fibreoptic endoscopes and video endoscopes.1–4 The two types differ in the method of sensing and transmitting images.

Flexible fibreoptic endoscope handpiece. Note the eyepiece on the control panel

Video gastroscope handpiece. Note the absence of an eyepiece on the control panel

3.0 mm flexible video-uretero-renoscope. ©2013 Courtesy of KARL STORZ GmbH & Co KG
Although fibreoptic endoscopes are less expensive than video endoscopes, the latter have recently become financially attainable for those in general practice. The main technical factor limiting the widespread use of true videoscopes has been the difficulty in achieving insertion tube diameters of <6 mm to allow their use in smaller veterinary patients. Technology is constantly evolving, however, and with the miniaturisation of CCDs, and the introduction of complementary metal oxide semi-conductor (CMOS) sensor technology, flexible high- definition video endoscopes with insertion tube diameters as small as 2.5 mm are becoming available on the human market. Currently, this technology is likely to be beyond the pocket of most veterinary surgeons but it will inevitably become more affordable in the future.
Rigid endoscopes
Rigid endoscopes do not bend, which limits their usefulness in the gastrointestinal and respiratory tracts. However, they vary in their distal tip viewing angle, commonly from 0° to 30° in veterinary endoscopes (Figure 4). A 30° endoscope allows the operator to see around corners and, by rotating the insertion tube along its long axis, visualise a wider area in a restricted space such as the trigone of the bladder.
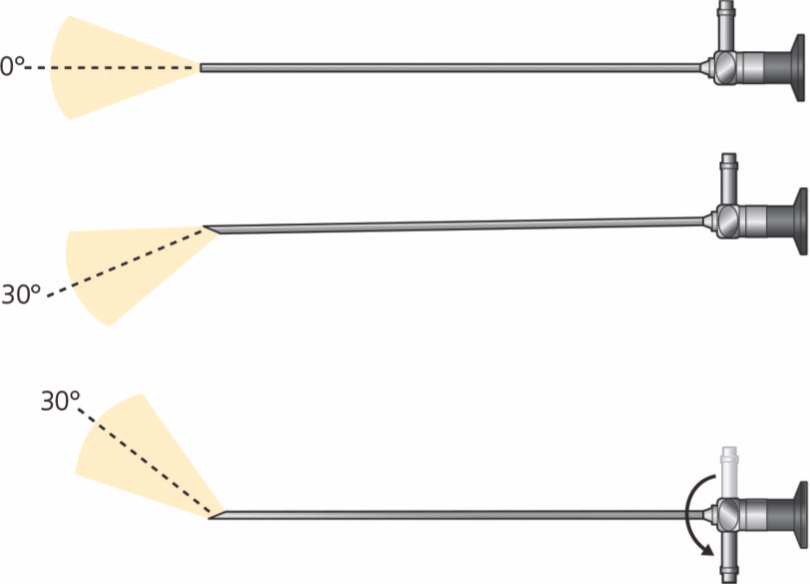
Viewing angle of 0° and 30°
The procedures for which rigid endoscopes are most suitable are conventionally named according to the anatomic region in which they are used:
Laparoscopy
Thoracoscopy
Rhinoscopy
Sinusoscopy
Urethrocystoscopy
Otoscopy
Arthroscopy
Fistuloscopy
Many of these procedures will be discussed in accompanying articles in this Special Issue series.
Basic endoscope anatomy
Flexible endoscopes
The basic flexible endoscope (Figure 5) consists of three main components: insertion tube, handpiece and umbilical cord.

Flexible endoscope anatomy
Insertion tube
This is a long flexible tube that is inserted into the patient. It contains:
Coherent glass fibreoptic bundles (fibrescopes) or electronics (videoscopes, Figure 6) to transmit the images to the handpiece.
Non-coherent fibreoptic bundles to provide illumination at the tip.
Control cables to allow manoeuvering of the tip.
An irrigation channel.
A biopsy channel.
A suction channel.

Tip of video endoscope insertion tube. (a) Working channel, (b) light source, (c) viewing lens/CCD chip and (d) air/water channel
Handpiece
The handpiece controls the endoscope functions and movement of the insertion tube.
There are one or two buttons on the top that are colour-coded: red = suction, blue = air and water control.
On gastroduodenoscopes, there are control wheels:
– A larger inner wheel for upward and downward tip deflection;
– A smaller outer wheel for movement of the tip left and right.
Bronchoscopes have a single lever that controls two-way deflection (Figure 7).
A friction brake lever may be used to fix the tip deflection in any given direction.
An instrument channel, located on top of the handpiece, accommodates a variety of instruments including biopsy forceps, basket retrievers and cytology brushes, and can also serve as a suction channel.
An eyepiece is for direct viewing or attachment of a camera linked to a monitor (fibrescopes).
Programmable buttons are for white balance control and for capturing images/video (videoscopes).

Fibreoptic bronchoscope with two-way tip deflection
Umbilical cord
The umbilical cord plugs into the light source or video processor. It contains:
Fittings for insufflation, irrigation and suction.
A pressure compensation valve for pressure testing, air transport and gas sterilisation.
In the case of videoscopes, a video cable connector on the distal end of the umbilical cord, which connects to a video processor to transmit the image to a monitor.
It should be noted that some fibrescopes, such as ureteroscopes and bronchoscopes (Figure 7), do not have an umbilical cord. They often require a light-guide cable (Figure 8) that attaches to the light post of the handpiece. In these endoscopes the pressure compensation valve will be positioned on the handpiece.
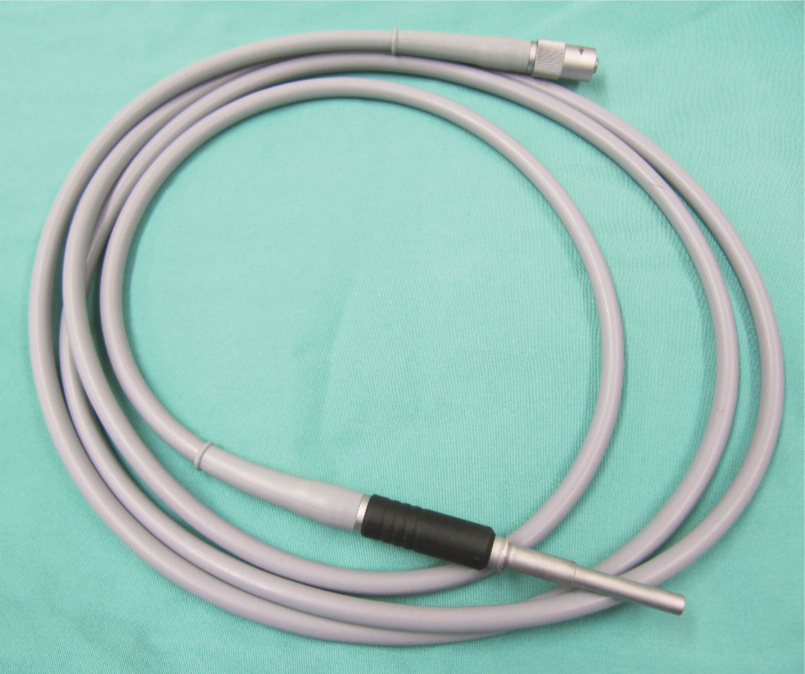
Fibreoptic light-transmitting cable used to connect to the light post of the bronchoscope handpiece
Looking at the endoscope’s tip, the working channel, fibreoptic light guides, air/water nozzle, and video chip or viewing lens can be seen (Figure 6). The tip of a bronchoscope is connected by two cables to the lever that allow two-directional tip angulation. A gastroduodenoscope has four cables that enable four-way deflection of the tip when the control knobs are turned.
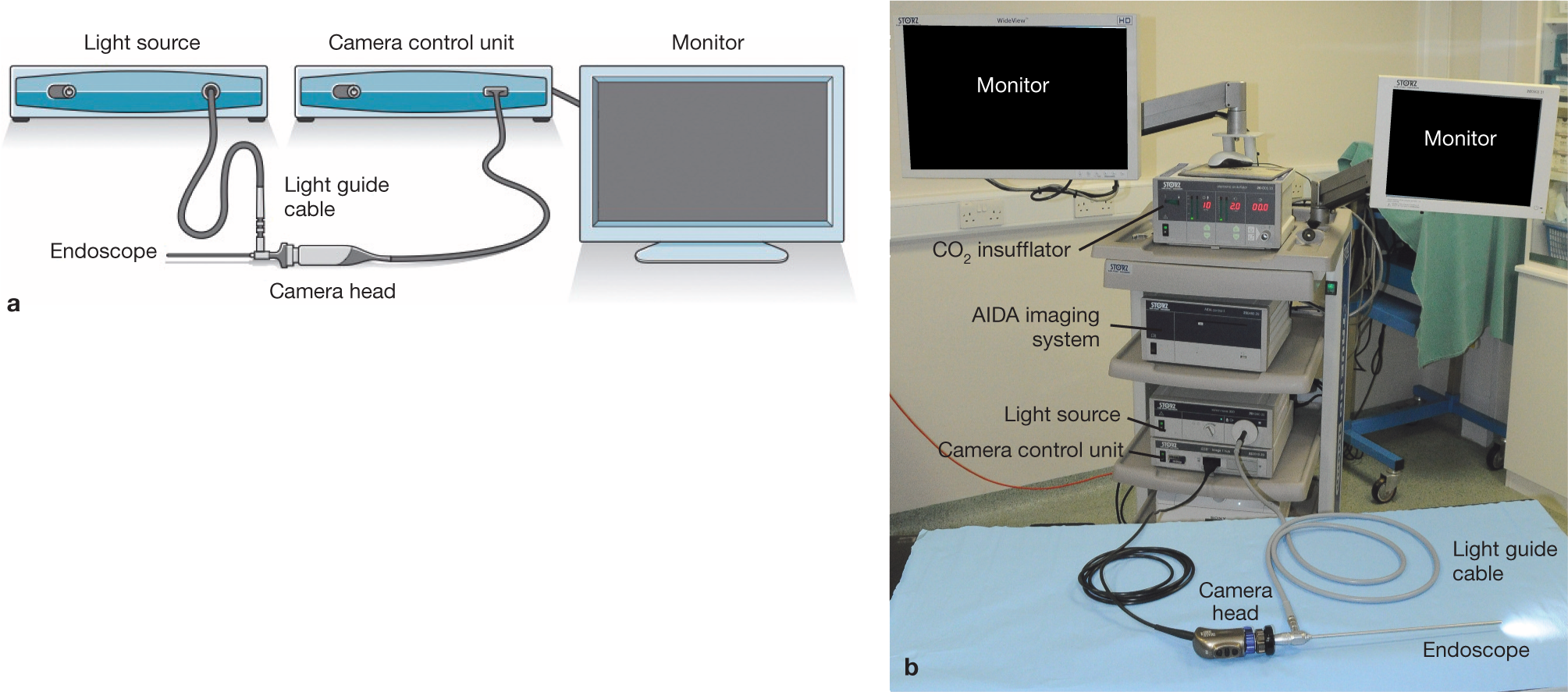
(a,b) The video imaging chain

A single camera control unit (top) and xenon light source (bottom) with connector for a fibreoptic light cable

Rigid endoscopes
A rigid endoscope consists of a stainless steel insertion tube containing solid glass rod lenses surrounded by light guide fibres, an oculus or eyepiece, and a light guide connector. A flexible fibreoptic light guide cable connects the light guide connector to the light source.
Rigid endoscopes vary in length, diameter of the insertion tube and viewing angle. In feline endoscopy the most commonly used rigid endoscopes will have a diameter of 2.7 mm or less and a viewing angle of 0º to 30º. These endoscopes are delicate and will always be used in a supporting sheath such as a cystoscope sheath or examination sheath. A camera is invariably used, especially in operative surgery, and clips onto the oculus to give a high quality image.
Choosing the appropriate endoscope
There are a variety of different makes, sizes, diameters and functions available when shopping for an endoscope. Unfortunately, there is no ‘one size fits all’ endoscope that will perform all procedures (eg, gastrointestinal endoscopy, bronchoscopy, rhinoscopy, cystoscopy) in all veterinary patients sufficiently well. Nonetheless, in feline practice, versatility is certainly an important factor when considering equipment investment – and, therefore, the selected endoscope should be able to perform as many functions as possible.
The key factors in selecting an endoscope are listed on page 972. Given that it is not possible for a single endoscope to be used for all endoscopic procedures in small animal practice, separate endoscopes for examination of the respiratory tract, gastrointestinal tract and peritoneal cavity (laparoscopy) are usually needed.

Camera head for a basic endoscopic video camera system

The Telepack Vet X is a portable endoscopy system. It is compatible with flexible fibreoptic endoscopes, video endoscopes and rigid endoscopes. ©2013 Courtesy of KARL STORZ GmbH & Co KG


For gastrointestinal endoscopy, a good ‘universal’ size flexible endoscope for most small/medium dogs and larger cats would have an outside insertion tube diameter ?7.9 mm, a biopsy channel of 2 mm or more (the larger the channel, the larger and more diagnostic the biopsy samples that can be retrieved), four-way tip control, a working length of approximately 100–140 cm, air insufflation and water spray capabilities, and excellent optics. In fibreoptic endoscopes, smaller insertion tubes may result in compromised image quality due to decreased numbers of both coherent and non-coherent fibreoptic bundles required for image transmission and illumination, respectively. In addition, the smaller the biopsy channel, the more limited the range of accessories (especially balloon dilators and some foreign body retrieval forceps) that can be used (see later). However, smaller diameter endoscopes (eg, paediatric gastroscopes) are easier to pass through the pylorus into the duodenum. For upper and lower gastrointestinal endoscopy, the authors recommend an insertion tube of ?7.9 mm x 100–140 cm working length endoscope for most feline patients, but a smaller 5.5 mm x 100 cm paediatric gastroscope can be useful in those patients requiring ileoscopy.
The most common rigid endoscope used in feline practice is the 2.7 mm x 18 cm 30º endoscope (Figure 13). This endoscope is used in a variety of sheaths depending on the procedure. An examination sheath is used for laparoscopy and thoracoscopy, and a cystoscopy sheath (Figure 13) is used for rhinoscopy, urethrocystoscopy and otoscopy. An arthroscopy sheath may be substituted for the cystoscopy sheath in these latter procedures as it has a smaller cross-sectional area; but there is one major disadvantage – it lacks an instrument channel.

From top: rigid 2.7 mm x 10 cm 30° oblique endoscope, cystoscopy sheath and arthroscopy sheath
An alternative is the 9.5 Fr operating telescope, which is a 1.9 mm telescope permanently built into a cystoscopy sheath. It has a length of 14 cm and a 3 Fr instrument channel, making it ideal for urethrocystoscopy, rhinoscopy and otoscopy in most cats (Figure 14).

1.9 mm telescope with integrated sheath
Factors to consider when sourcing endoscopic equipment, including the relative advantages of purchasing new over secondhand instruments, are discussed in the box on page 973.
Ancillary instrumentation
Accessories for flexible endoscopes
Accessories for flexible endoscopes include biopsy forceps, a variety of foreign body retrieval forceps, sheathed cytology brushes, aspiration tubes and balloon dilating catheters. These accessories assist in and enhance functionality, adding versatility for both diagnostic and therapeutic interventions.
There are a number of tissue biopsy forceps available including standard oval cup, fenestrated oval cup (Figure 15) and alligator forceps (Figure 16). The fenestrated cup forceps do not cause as much crush artefact and tend to yield larger samples. The alligator-type forceps with a serrated edge generally grip the mucosa better than smooth edged forceps. Fenestrated oval cupped alligator forceps provide a good combination of grip, sample size and reduced artefact. Both fenestrated and non-fenestrated cupped biopsy forceps are available with a central needle or spike that tends to anchor the forceps into the mucosa, preventing them from sliding down the tissue. Opinion varies from operator to operator as to which type of forceps is the best, cupped (fenestrated versus non-fenestrated) or alligator.

Fenestrated cupped biopsy forceps with (left) and without (right) central spike

Alligator forceps with non-serrated edge

Biopsy forceps are designed to be used in the biopsy channel of the endoscope. The outer diameter of the forceps should be slightly smaller than the endoscope’s biopsy channel. For example, for a biopsy channel measuring 2.0 mm, the forceps should be 1.8 mm diameter and be about 50 cm longer than the channel. Biopsy forceps should never be used for foreign body retrieval.
Several types of grasping forceps and retrieval baskets are available for foreign body removal. There are three basic types of graspers: three- or four-pronged wire forceps (Figure 17), ‘rat tooth’ forceps and ‘duckbill’ forceps. The pronged forceps are useful for large irregular objects, the rat tooth forceps for grasping fabric or other soft material and the duckbill forceps for flat objects like coins. Single loop wire snares and three- or four-loop wire baskets (Figure 18) are required to remove large or smooth objects like stones. It is recommended to have at least two, and preferably three, different foreign body retrieval instruments. A single loop snare, three- or four-pronged grasper and a wire basket are good options. With these three instruments, most foreign bodies can be retrieved.

Three-pronged grasping forceps

Wire basket foreign body retriever
Guarded cytology brushes and aspiration catheters are also available. Balloon dilators of 6–8 cm lengths and 15–20 mm inflatable diameter (Figure 19) are recommended for gastrointestinal tract strictures and are usually used with a pressure gauge to prevent overdistension and rupture of the balloon.

Balloon dilator catheters
Accessories for rigid endoscopy
Instrumentation for rigid endoscopy will depend on the procedures undertaken. For rhinoscopy and cystoscopy, semi-flexible biopsy forceps and grasping forceps appropriate to the size of the instrument channel in the cystoscope are used (5 Fr for the larger 14.5 Fr cystoscope and 3 Fr for the smaller 9.5 Fr operating cystoscope) (Figure 20a). A pair of larger rigid biopsy forceps with a 3 mm cup and 1.5 mm shaft (Karl Storz 69133) (Figure 20b) is extremely useful for obtaining larger biopsies during rhinoscopy and can be used alongside the endoscope or placed blind following localisation of the lesion with the endoscope.

(a) Semi-flexible forceps that can be placed through the biopsy channel of a cystoscopy sheath. Alternatively, larger rigid forceps (b) can be used, under visual guidance, parallel to a endoscopic sheath for larger samples. ©2013 Courtesy of KARL STORZ GmbH & Co KG
A selection of three or more laparoscopic cannulae will be required for operative surgery. For feline laparoscopy, a 3 mm examination sheath is used with a 2.8 mm x 18 cm 30º endoscope and this is placed through a 3.9 mm Ternamian EndoTip cannula (Karl Storz, Germany) or 3.9 mm operating cannula with a sharp trocar (Figure 21). Commonly 5 mm hand instruments are used and require one or two 6 mm threaded positive-profile cannulae (either Ternamian tipped or with sharp trocar). Alternatively, 3 mm paediatic instruments may be used with appropriate trocars.

3.9 mm threaded cannula and trocar
A range of hand instruments, including those listed in the box below, will be required for routine procedures. More specialist instrumentation may be required for advanced procedures.

Cabinet with hanging facilities for endoscope storage

Suitable storage for rigid endoscopes


Care and cleaning of endoscopic equipment/accessories
While detailed information about cleaning and maintenance of equipment goes beyond the scope of this article, the authors’ general advice is always to follow the manufacturer’s recommendations for cleaning, disinfecting and storing endoscopes, accessories and the various components. This will significantly prolong the life of the equipment and lower the risk of iatrogenic infections to the patient and contamination of samples. Although most modern endoscopes are marked as safe for immersion, the manufacturer’s instructions should always be consulted before a piece of equipment is fully immersed in fluids. Fibreoptic endoscopes are generally paired with a leak-tester which is used to detect small air leaks before they cause major damage to the endoscope. A leak test should always be performed before a flexible endoscope is immersed in fluid and the endoscope should remain pressurised all the time it is immersed.
User-related damage is usually caused by inappropriate cleaning practices. It is, therefore, advisable to select specific staff members to be well trained on cleaning procedures for both flexible and rigid endoscopic equipment. Biopsy and retrieval instruments are extremely delicate and prone to damage, and deserve the same meticulous care as endoscopes. Biopsy forceps should be carefully cleaned with an enzymatic solution to dissolve proteinaceous materials, then disinfected and well lubricated.
For specific cleaning protocols compatible with your purchased equipment contact the relevant manufacturer(s). Company representatives are very helpful with offering advice and may even come to the practice to train staff members on endoscope care and maintenance. It can be useful to laminate a cleaning guide and supply list specific to the model of endoscope used in the practice to expedite the procedure in the busy clinic environment.
Key points
Veterinary practitioners are starting to appreciate the benefits of minimally invasive procedures and are incorporating endoscopic techniques into everyday practice.
In addition to the benefits of reduced tissue trauma, minimal postoperative pain and faster recovery times, especially in feline patients, the endoscopist enjoys vastly improved visualisation of the surgical site through excellent illumination and a high quality magnified image – often of sites that are impossible or difficult to access in any other way.
This, together with clients’ awareness, and sometimes personal experience, of minimally invasive procedures has created an expectation and demand for these services in the veterinary sector.
Endoscopes are now more widely available outside of the referral setting, and financially accessible to those in general practice. With purchase of suitable equipment, and appropriate investment in training, a committed practitioner can readily learn basic endoscopic techniques.
The budding endoscopist should strongly consider participating in hands-on ‘wet-lab’ courses and ongoing training provided by experienced endoscopists to rapidly achieve a level of competence that justifies the high initial investment in providing this type of service.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.