
Abstract
An 11-year-old spayed female domestic shorthair cat was presented for polydipsia, hyperactivity and bilateral thyroid gland enlargement. Total T4 (TT4) was in the upper interval range; therefore, an early hyperthyroidism was suspected. A treatment trial with methimazole was started, as the owner refused further tests. Six months later the owner stopped the treatment. One year later, clinical signs persisted and TT4 was still in the upper interval range. Methimazole was re-introduced but 48 h later the cat presented non-pruritic alopecia with erythema, scales and perilesional yellowish crusts. Pyogranulomatous mural folliculitis was diagnosed by histopatological examination of the skin biopsies. Methimazole was withdrawn and macroscopic lesions healed and disappeared histologically in 15 days. An idiosyncratic drug reaction to methimazole was suspected. To the best of our knowledge, this is the first report of feline pyogranulomatous mural folliculitis likely secondary to an adverse drug reaction to methimazole administration.
Case Report
An 11-year-old spayed female domestic shorthair cat was referred with polydipsia and hyperactivity over the last few months. Previous history was unremarkable. On presentation, the cat was alert, bright and in good body condition (body condition score 5/9). All vital parameters were normal, including systolic pressure (137 mmHg), but heart rate was increased (202 ppm). A bilateral thyroid enlargement nodule was palpable on physical examination. Complete blood count (CBC), serum chemistry profile (SCP) and urinalysis results were within reference intervals (RIs). Feline leukaemia virus antigen and feline immunodeficiency virus antibody tests were negative. A total T4 (TT4) determination was performed and the result was 3.0 µg/dl (RI: 1.1–3.2 µg/dl). Early hyperthyroidism was suspected, but the owner refused further tests. Therefore, a trial treatment with methimazole (Tirodril; Aldo-Union) was started at 2.5 mg per cat daily. The cat was re-examined 2 weeks later. CBC and SCP were within the normal limits; TT4 was 1.7 µg/dl, so treatment was continued and follow-up was scheduled in 1 month. One year later, the cat was presented for re-examination. Polydipsia and hyperactivity persisted and the thyroid enlargement was still present. The owner had withdrawn methimazole at her own discretion 6 months before. TT4 was repeated and was 3.2 µg/dl (RI: 1.1–3.2 µg/dl). Further tests were refused again by the owner and methimazole (Tirodril; Aldo-Union) at 2.5 mg per cat daily was re-introduced. Forty-eight hours later, after two doses of methimazole, the cat returned to the hospital with mild asthenia and alopecia with erythema, scales and perilesional yellowish crusts on the dorsal cervical, suprascapular and supraorbital areas (Figure 1a, b). Lesions were non-pruritic. No other medications, vaccines or topical ectoparasiticides had been administered in the previous weeks.
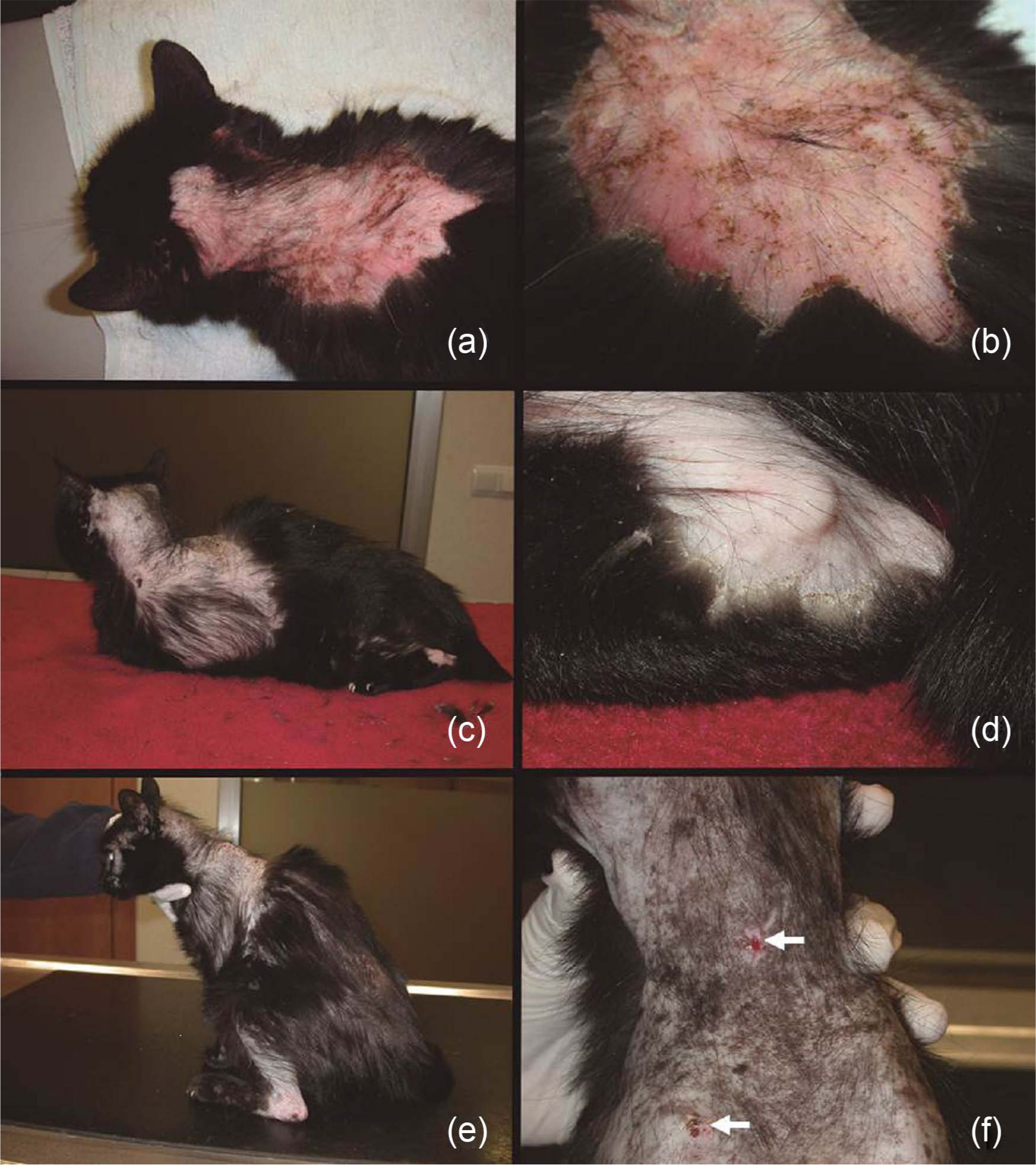
(a,b) Clinical lesions on presentation: non-pruritic alopecia and erythema with scales and yellowish crusts are noticed on the dorsal cervical and interscapular areas. (c,d) Clinical lesions presented 1 week later: although alopecia has spread, there is improvement of lesions, with mild scaling and disappearance of erythema. (e,f) Clinical lesions 2 weeks after initial presentation: regrowth of hair is noticed and there are no signs of cutaneous inflammation. (f) The two lesions observed (white arrows) are the places in which punch biopsy had been performed 2 weeks previously
A cutaneous adverse drug reaction to methimazole was suspected. Trichoscopic examination, Wood’s lamp examination and skin scrapings showed no pathogens on skin surface. Cytologies of the skin showed degenerated neutrophils without bacteria. Samples for fungal culture and two 6 mm diameter punch skin biopsies specimens were obtained. While waiting for the results, methimazole treatment was withdrawn and no treatment was prescribed.
Skin biopsy samples were processed; 3 µm sections were obtained and stained with haematoxylin and eosin following standard procedures. Histopathological examination revealed irregular epidermal hyperplasia with spongiosis. There was lymphocyte and neutrophil exocytosis into the epidermis with the formation of serocelullar crusts. A mixed perivascular infiltrate with mast cells, lymphocytes, and fewer neutrophils and eosinophils was present in the superficial dermis. A pyogranulomatous inflammation with neutrophils, macrophages and, focally, plasma cells with Russel bodies in the perifollicular dermis at the level of isthmus was observed in about 40% of follicles. The infiltrate did not involve the sebaceous glands. There was a paucity of anagen hair follicles and exocitosis of neutrophils and macrophages to the follicular epithelium forming mural pyogranulomas (Figure 2a,b). Ziehl-Neelsen and periodic acid-Schiff stains and immunohistochemistry to detect Leishmania amastigotes were negative. Fungal culture yielded a negative result.

Microscopic pictures of skin biopsies. (a) Irregular epidermal hyperplasia, superficial perivascular infiltrate and paucity of anagen hair follicles are observed on the first skin biopsy. Haematoxylin and eosin (H&E), bar = 500 μm. (b) Exocytosis of macrophages and neutrophils to the follicular epithelium forming a mural pyogranuloma (black arrow) is observed on the first skin biopsy. H&E, bar = 100 μm. (c) Disappearance of epidermal hyperplasia and dermal inflammation are observed with normal appearing microscopic skin and numerous hair follicles in anagen phase on the biopsy retrieved 15 days later. H&E, bar = 500 μm
The patient was visited 1 week later. There was no apathy and the lesions had spread over the ventral trunk, abdomen and limbs (humeral and hock areas). However, during the previous 72 h, an improvement had been noted and the erythema had disappeared. There was alopecia and mild scaling (Figure 1c,d). One week later, a more marked improvement was noticed. The hair was re-growing and there were no signs of cutaneous inflammation (Figure 1e, f). With the owner’s consent, a second biopsy was obtained to understand the histological evolution of lesions. Histopathological examination revealed only a mild focal perifollicular granulomatous inflammation, and most hair follicles were in anagen phase (Figure 2c). Two months later the lesions had resolved. Methimazole was not reintroduced. After 3 years of follow up, clinical signs of polydipsia and hyperactivity had disappeared; the cat’s fur was totally normal and the TT4 level was within the updated normal RI (1.3–3.7 µg/dl) of our laboratory.
Granulomatous mural folliculitis is a rare cutaneous reaction that may be associated with different aetiologies in veterinary medicine, mainly to adverse drug reactions (ADR) and, in rare cases, to viral infections.1–5 The aetiopathogenesis is currently unknown, but the histopathological lesions with granulomatous-to-pyogranulomatous inflammation and good response to immunomodulatory drugs in some of the cases described suggest an immune-mediated reaction.1,2
L-thyroxin, amitraz, cefadroxil and some topical agents have been reported to induce these microscopic lesions in dogs, and multiple systemic and/or some topical drugs in horses.1–3 This cat had not received any other medication than methimazole. However, these histopathological lesions in humans and deer have been associated with herpesvirus infection.4,5 There is one case of pyogranulomatous mural folliculitis reported in a cat, but distribution and chronicity of lesions were different to the ones of the cat described herein. 6 Moreover, there was no history of drug administration prior to the onset of the lesions. 6 That cat was treated with cyclosporine because an immune-mediated follicular disease was suspected and partial response was observed. 6 Contrary to this reported case, the cat described in the present report presented spontaneous resolution without the need for any immunomodulatory treatment.
Macroscopic cutaneous lesions of the pyogranulomatous mural folliculitis are different between species. In dogs, deer and in the cat reported by Noli and Toma different degrees of alopecia, erythema, scaling, crusting, hyperkeratosis and/or erosive-ulcerative lesions with exudation are described.1,2,5,6 However, in humans and horses, papules or plaques, which in horses may be crusted, are the macroscopic lesions associated with granulomatous or pyogranulomatous mural folliculitis.3,4 The cutaneous lesions of the cat described herein are similar to the ones described in dogs, deer and one cat.1,2,5,6
Other feline mural folliculitis reported are degenerative mucinotic mural folliculitis (DMMF) and infiltrative lymphocytic mural folliculitis (ILMF).1,7,8 The DMMF is presumptively an immunological idiopathic skin disease and the ILMF is mainly associated with allergic dermatoses.1,7,8 Furthermore, dermatological and histopathological features are different to this case report.1,7,8
Oral methimazole may cause ADRs in 18.3% of cats. 9 The ADRs associated with this drug may include gastrointestinal signs, hepatopathy, facial pruritus, bleeding diathesis and mild haematological disorders. 9 The most common cutaneous lesions reported as ADR in 2.3% of cats receiving methimazole consist of severely pruritic neck and face excoriations.9,10 This cat did not show pruritus and skin lesions, and distribution was different. Unfortunately, there are no reports on the histopathological features associated with the facial excoriations, making it impossible to compare histologically both clinical presentations. Other unusual ADRs reported are pemphigus foliaceus, acquired myasthenia gravis and generalised lymphoadenomegaly.10–13
Type B (bizarre) or idiosyncratic drug reactions (IDR) are rare, unpredictable, dose-independent and unrelated to the drug’s pharmacological effect. 14 They are related to the individual’s immunological response, or to genetic differences in susceptibility of patients, and are frequently allergic, intolerant or aberrant reactions.14–19 In human medicine, IDRs associated with methimazole are similar to those reported in cats, for example skin reactions (skin rash and itching), agranulocytosis, leukopenia, thrombocytopenia, aplastic anaemia, hepatitis and cholestasis, but the basic mechanisms of these reactions remain elusive.9,14,20 Pyogranulomatous mural folliculitis have not been previously associated with methimazole in any species.
The aetiopathogenesis in our case is uncertain. Pyogranulomatous mural folliculitis has been associated with immunopathological reactions in all cases reported, but specific mechanisms have not been elucidated.1–3 Moreover, the mechanism whereby anti-thyroid medications may induce adverse immunological reactions in vivo remains largely unknown.14,19 Although most of the drug reactions observed in type B reactions are type I or IV reactions, a delayed hypersensitivity reaction might not explain the reaction in this case.17,18 Delayed reactions appear 48 h to 4 weeks after antigen exposure, and our patient received methimazole over a long period the first time, but an IDR might have been elicited by some unknown mechanism when it was reintroduced 1 year later.16,17
According to the cases reported, pyogranulomatous mural folliculitis associated with ADRs should be managed by withdrawing the drug and by treating with immunosuppressive drugs (corticosteroids or cyclophosphamide) if needed. 2 In our case, methimazole was withdrawn and a rapid improvement and resolution of the lesions was observed. Therefore, a mural pyogranulomatous folliculitis possibly secondary to the administration of methimazole was considered. For ethical reasons, a re-challenge with methimazole to confirm an ADR was not considered.
Conclusions
To the best of our knowledge, this is the first report of feline pyogranulomatous mural folliculitis likely secondary to an ADR, suspected to be caused by methimazole administration.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.