
Abstract
Cavernous sinus syndrome is characterised by internal and external ophthalmoplegia and sensory deficits over the head due to combined deficits of the three cranial nerves (CNs) responsible for the eye movements and pupil function (CN III, IV, VI) and at least one branch of the trigeminal nerve (CN V). It has rarely been described in cats and may occur secondarily to inflammatory, infectious or neoplastic lesions within the region of the cavernous sinus on the ventral aspect of the calvarium. This report describes the clinical and magnetic resonance imaging findings in a 14-year-old domestic shorthair cat with neurological deficits compatible with cavernous sinus syndrome caused by presumptive extranodal lymphoma. Treatment with chemotherapy resulted in clinical and imaging remission. Identification of the neurological deficits in cavernous sinus syndrome allows accurate neuroanatomical localisation in order to target diagnostic imaging studies.
Case Report
A 14-year old, female neutered, domestic shorthair cat was presented to the referring veterinary surgery with a history of altered behaviour, reduced appetite, mild polydipsia and anisocoria, with the right pupil larger than the left pupil. Vaccination and worming status were current and the cat was housed indoors with free access to the outdoors. There was no history of trauma. Complete blood count (CBC) and biochemistry panel revealed a mild increase in serum creatinine (237 μmol/l, laboratory reference <212 μmol/l), but was otherwise within normal limits. On referral, complete physical examination demonstrated mild bilateral renomegaly on abdominal palpation. The remainder of the physical examination was normal apart from the findings of the neurological examination. Neurological examination revealed the cat to be slightly obtunded with a normal menace response and dazzle reflex in both eyes; however, marked anisocoria was present, with mydriasis in the right eye (Figure 1). Direct (stimulation of the right eye) and consensual (stimulation of the left eye) pupillary light reflexes were absent in the right eye, pupil function was normal in the left eye to light stimulation of the left or right eyes, indicating a lesion affecting the parasympathetic portion of the right oculomotor nerve [cranial nerve (CN) III]. Examination of both fundi revealed no abnormalities. Evaluation of physiological nystagmus (vestibulo-ocular reflex) revealed absence of normal eye movements in all directions in the right eye, with normal eye movements in the left eye, indicating a lesion affecting the general somatic efferent of the right oculomotor nerve (CN III), trochlear nerve (CN IV) and abducens nerve (CN VI) (Figure 1). Loss of iris and ciliary function is usually referred to as internal ophthalmoplegia, while paralysis of all the extraocular muscles is usually referred to as external ophthalmoplegia. This combination of internal and external ophthalmoplegia is also termed complete ophthalmoplegia or panophthalmoplegia. Testing of sensation over the face revealed absent corneal sensation in the right eye, indicating a lesion affecting the ophthalmic branch of the right trigeminal nerve (CN V). The remainder of the neurological examination was within normal limits.
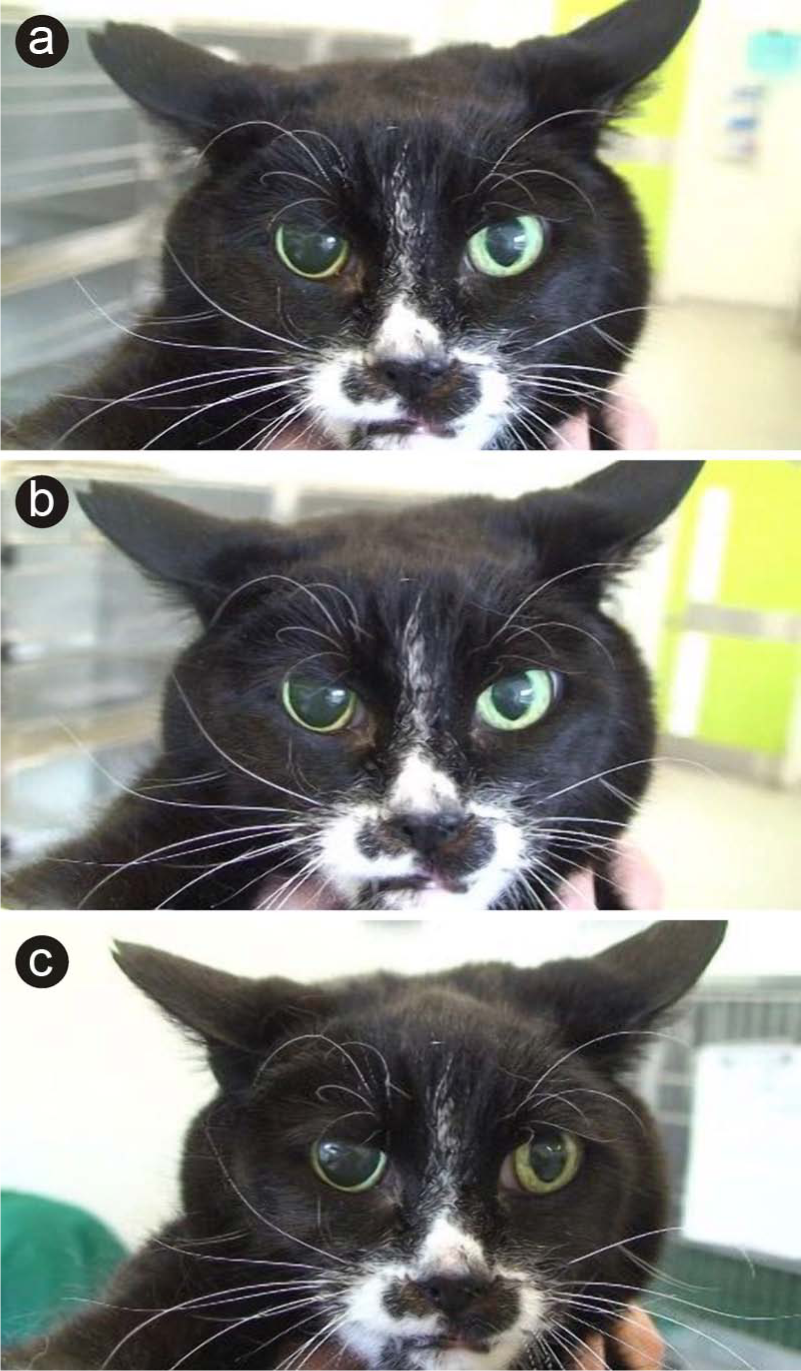
Anisocoria in a 14-year-old domestic shorthair cat, with mydriasis in the right eye. In addition to the lesion affecting the right pupil, the affected right eye also demonstrated external ophthalmoplegia (paralysis of the extraocular muscles). The normal left eye was able to look straight ahead (a), deviate the gaze to the right (b) and deviate the gaze to the left (c), but in all instances the cat was unable to deviate the affected right eye
Differential diagnoses for unilateral mydriasis include unilateral glaucoma, iris muscle lesion (eg, iris muscle atrophy or pharmacological blockade), Pourfour du Petit syndrome or oculomotor nerve lesion. Apart from a unilateral oculomotor nerve lesion and pharmacological blockade, all other differential diagnoses can be excluded by a thorough ophthalmic examination. However, when the mydriasis is considered in combination with the other neurological deficits affecting the eye then this constellation of cranial nerve deficits is consistent with a lesion affecting the right ventral cranial cavity in the region of the right cavernous sinus. This neuroanatomical localisation would also provide an explanation for the obtunded mentation. Differential diagnoses for a lesion in this specific location include infection (toxoplasmosis, cryptococcus and feline infectious peritonitis), trauma, vascular (malformation) and neoplasia (primary, metastatic, multicentric). 1 The minimum database in this case included a repeated CBC and biochemistry panel, and urine analysis and abdominal ultrasound to investigate the renomegaly. The blood results were normal apart from a consistently elevated creatinine value (272 μmol/l, laboratory reference <212 μmol/l). Urinalysis demonstrated a urine specific gravity of 1.028 (which was viewed to be inappropriately dilute given the serum creatinine concentration). There was no evidence of proteinuria, and sediment examination was inactive. Serial blood pressure measurements were within normal limits. Thoracic computed tomography to complete staging was unremarkable. Abdominal ultrasound confirmed bilateral renomegaly with an irregular outline and subcapsular hypoechoic rim (which is a common finding with renal lymphoma). 2 Intra-abdominal lymphadenopathy was also noted (mesenteric and renal lymph nodes). The main differential diagnoses for the renal changes in this patient included primary renal neoplasia (eg, renal lymphoma), metastatic neoplasia or metabolic disease/toxin ingestion. Cytology from ultrasound-guided fine-needle aspirates of the kidneys was consistent with lymphoma. Magnetic resonance imaging (MRI) of the brain was performed to investigate the right cavernous sinus syndrome using a 1.5-Tesla unit (Siemens, Magnetom). An intracranial mass lesion was evident on the ventral aspect of the cranial cavity in the region, adjacent to the cavernous sinuses and pituitary gland. The mass lesion was ill defined with irregular margins and located dorsal to the pituitary gland. The mass was isointense to grey matter in T1-weighted images and hyperintense to grey matter in T2-weighted images, and showed marked contrast enhancement after intravenous gadopentetate dimeglumine (94 mg/kg; Magnevist, Bayer Health Care Pharmaceuticals) administration (Figure 2a, b). There was the suggestion of a contrast tail (dural tail) on the post-contrast studies adjacent to the pituitary gland, which may be indicative of meningioma or lymphoma. 3 The remainder of the MRI study was within normal limits. Cerebrospinal fluid (CSF) analysis, obtained from the lumbar cistern, revealed mild protein elevation (490 mg/l, laboratory reference <400 mg/l) with a normal white cell count (three white cells per microlitre, laboratory reference <5/µl). The MRI changes were consistent with intracranial neoplasia, most likely lymphoma.

Post-contrast T1-weighted MR images before (a,b) and 6 weeks after (c,d) initiation of treatment with the University of Wisconsin–Madison lymphoma chemotherapy protocol in the sagittal (a,c) and transverse (b,d) planes. There is a contrast-enhancing mass lesion in the region of the pituitary gland (arrowed) in (a) and (b). In the post-treatment images (c,d) there is resolution of the mass lesion
The combination of neurological deficits demonstrated by this cat [panophthalmoplegia (CNs III, IV and VI), a lesion of the ophthalmic branch of CN V and intact vision] are part of a syndrome known as cavernous sinus syndrome. In human patients, involvement of CN III and CN VI is observed in almost all cases, whereas CN IV is involved in only a third of patients. 4 The most frequent aetiologies include trauma and neoplasia. 4 In veterinary patients the identification of cavernous sinus syndrome depends upon demonstration of paralysis of CNs III, IV, VI and at least one branch of CN V. 5 The CN V lesion may present as sensory deficits over the face or cornea and/or as ipsilateral masticatory muscle. Located on the floor of the calvarium, adjacent to the pituitary gland, the cavernous sinuses are paired venous structures that represent a convenient location for intracranial mass lesions to expand into. The evidence of renal lymphoma in this case is highly suggestive of extranodal lymphoma, and is consistent with the MRI findings of an intracranial mass that is isointense on T1-weighted images and hyperintense on T2-weighted images relative to grey matter, with marked contrast enhancement. Extension of renal lymphoma to include the central nervous system (CNS) is commonly found and accompanies this extranodal form of the neoplasia. 6 The response of renal lymphoma to chemotherapy is less than for other forms of the disease and long-term remission and survival are difficult to achieve. 6 This cat was managed with the Wisconsin–Madison chemotherapy protocol and at the time of the report was in clinical remission 6 weeks after the initial diagnosis (Figure 2c, d). No significant difference has been reported when comparing survival between cyclophosphamide, vincristine and prednisolone (COP)- based protocols and the University of Wisconsin–Madison protocol for the treatment of renal lymphoma. 7 In the same study, CNS lymphoma had the shortest median survival time. 7 Lymphoma involving a similar region of the cranial fossa has previously been reported, with Chang et al 8 describing two cats with CNS and nasopharyngeal lymphoma, and cranial fossa syndrome (including ophthalmoplegia) and stertor. Similar MRI characteristics have also previously been reported in cats with CNS lymphoma, including the presence of an apparent dural tail, which may represent meningeal spread of the disease, as previously demonstrated.3,9 The clinical utility of CSF analysis in CNS lymphoma is variable and may be normal in some cats.9,10
Conclusions
This case demonstrates the clinical appearance of cavernous sinus syndrome in a cat secondary to presumptive feline extranodal lymphoma and its clinical and imaging remission with chemotherapy. The presence of pupil dysfunction in conjunction with external ophthalmoplegia should alert the clinician to the potential of a lesion within the region of the cavernous sinuses.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.