
Abstract
Trans-iliac pin, bolt or screw stabilisation was performed on six cats with sacroiliac (SI) luxation and separation. For the purpose of this study, SI luxation is defined as the separation of the iliac wing from the sacrum without fracture of the sacral or iliac wing; SI separation is defined as the separation of the iliac wing from the sacrum secondary to fracture of the sacrum and/or the iliac wing. Complications, surgical time and medium-to-long-term outcome were assessed by a retrospective review of the clinical records and owner questionnaires. Postoperative reduction of the SI joint was good-to-excellent in all cases and the outcome was considered good-excellent in all cats apart from one, where the trans-iliac bolt migrated dorsally from the iliac wing. This cat had bilateral SI luxations. Based on our results, trans-iliac fixation of SI luxation/separation is associated with good clinical outcome and should be considered as a treatment option in unilateral SI luxation in cats. Caution should be exercised in the use of trans-iliac pin/bolt as the sole method of stabilisation in bilateral SI luxations.
Introduction
Sacroiliac (SI) luxation is the second most common pelvic injury in cats, occurring in 16–59% of cats with pelvic injuries.1,2 Unilateral SI luxations are always accompanied by other pelvic fractures or symphyseal separations. 3 Pelvic floor fracture and contralateral iliac body fracture are the most common fractures accompanying SI luxations. 2 Bilateral SI luxations can happen without other pelvic injury.2,4,5 The treatment of SI luxations can be broadly categorised into two groups: conservative treatment and surgical reduction and stabilisation. Conservative treatment involves analgesia, cage rest with soft padded bedding, and monitoring of urination and defecation. 6 Marked pain, inability to ambulate, unstable or marked displacement of hemipelvises (>50%), narrowing of the pelvic canals, neurological deficits attributed to SI luxations, concurrent orthopaedic injuries and failure to ambulate after 3 days of strict rest are some of the indications for surgical stabilisation of the SI luxation/separation.2,5,7–9 Recently, Meeson and Corr 9 also advocated surgical treatment of pelvic fractures that involve weight-bearing axis in cats, and these include SI luxations.
Conservative treatment is often the treatment of choice or believed to be an adequate option for pelvic fractures in cats.1,9–11 This decision is likely to be influenced by the belief that feline patients cope well with this type of injury (particularly when compared with dogs) and the fact that the traditional repair method for SI luxation — the SI lag screw — is perceived to be technically challenging and risky. 10 In a retrospective study, Bennett 1 reported good functional outcome with most cases after conservative management; no obvious lameness was reported at the end of 4 weeks. Reported complications of conservative treatment include displacement of the pelvic fragment, pelvic canal stenosis, and constipation or obstipation. 12 According to Langley-Hobbs, 13 although cats seem to recover well after conservative treatment, many will develop ankylosis of one or both SI joints, as well as degenerative changes in the lumbosacral joint. This is thought to be due to altered force transmission and compensatory overload. 11 Surgical stabilisation has been advocated for SI luxations as it enables early return to function and increases patient comfort. 14 These factors are particularly important as 58.6% of cats with pelvic fractures have concurrent musculoskeletal injuries. 11 Long-term studies examining the quality of life of cats with SI luxations that are managed conservatively versus managed surgically are lacking at this stage. 9
Reported surgical techniques for stabilisation of SI luxations in cats include an open approach with lateral SI lag screw placement, 15 single trans-sacral screw placement across the iliac wings and sacrum for bilateral SI luxations, 4 ventral abdominal approach and transarticular placement of a positional screw across the sacral and iliac wings,6,16 and SI pinning with tension band suture across the iliac wings. 10 Of these methods, lateral SI lag screw placement has been described as the traditional and the most popular method of surgical stabilisation of the SI luxations. 9
Clinical cases of trans-iliac stabilisation of SI luxation/separation have been reported in dogs,17,18 but to our knowledge, clinical cases where a trans-iliac pin/bolt has been used as the sole method of stabilisation in cats have not been documented.
Materials and methods
Data
Clinical records of cats admitted to the Small Animal Hospital, University of Glasgow, Fitzpatrick Referrals, Surrey, and Adelaide Veterinary Specialist and Referral Centre, Australia, with SI luxations/separations (March 2011 to March 2013) were reviewed retrospectively. Cats with SI luxation/separation that were stabilised solely by trans-iliac implants were included in the study. Information collected included signalment, concurrent orthopaedic and neurological injuries, treatment and surgical procedures performed, surgical time, and peri-operative and follow-up radiographs.
Client questionnaires were sent to each client to assess the medium (>4 months and <12 months) to long-term outcome (>12 months) of the surgeries; a minimum period of 4 months was required between surgery and questionnaire completion. The questionnaires were adapted from a previous study in feline pancarpal arthrodesis. 19 The questionnaires enquire about information regarding lifestyle changes and the ability to perform normal feline activities (see Supplementary data). Owners were asked to score how the activities were affected during the postoperative period and more recently utilising a simple, descriptive, discontinuous scoring system scale. In questions regarding lifestyle, owners were asked to assess the outcomes as dichotomous variables (‘yes’ or ‘no’) (see Supplementary data). A good outcome was defined as having a total disability score of ≤8; affected cats have a slight, but frequent, difficulty in performing normal activities. An excellent outcome was defined as having a total disability score ≤4; these cats do not have or have slight and occasional difficulty in performing normal activities.
Surgery
Surgeries were performed by four surgeons working independently at three referral centres. During surgery, each cat was placed in ventral recumbency with the hind limbs slightly extended caudally. The caudal lumbar and lateral thigh regions were prepared aseptically before surgery. A dorsal approach to the iliac wings was performed bilaterally in five cats. In one cat (cat 6), a dorsal midline approach to both iliac wings was performed. The middle gluteal and sacrospinalis muscles were elevated from the periosteal origins laterally and medially to expose the craniodorsal aspect of the iliac wings. The SI luxation was reduced by traction and manipulation of the iliac wing and the ischial tuberosity (via a separate small approach caudally) on the luxated hemipelvis. The degree of reduction was assessed by comparing the symmetry of the iliac crests, while the reduction of the SI joint was maintained with a point-to-point reduction forceps across the SI joints. A trans-iliac implant was placed from the iliac wing on the luxated side, across the dorsal aspect of L7 and into the contralateral iliac wing. When a trans-iliac pin was used, the iliac wings were not predrilled. The ends of the pins were bent laterally against the iliac wings bilaterally to prevent pin migration and to maintain reduction (Figure 1). In three cats (cats 3, 5 and 6), a trans-iliac bolt or screw was used. After the reduction of the SI joint, the iliac wings were predrilled and the trans-iliac bolt or screw was inserted from the luxated hemipelvis to the contralateral hemipelvis. The middle gluteal and sacrospinalis muscles were apposed and sutured to the iliac periosteum. The subcutaneous tissue and the skin were closed in routine fashion. Postoperative radiographs were taken to assess the reduction of the SI joints, and the implant position and placement. All animals received postoperative opiod analgesia and anti-inflammatory medications. The types of medications were chosen at the discretion of individual surgeon. All cats were discharged with instructions on strict activity restriction (cage or small room confinement with no jumping and running) for 6–8 weeks.

(a) Pre-operative radiograph showing left sacroiliac (SI) luxation, and pubic and ischial fractures in cat 2. There was a focal increase in mineral opacity at the level of 1/3 proximal diaphysis. This was a fragment of the ischial fracture, which was also visible on the postoperative radiographs. (b) The SI luxation was stabilised with a trans-iliac pin, which is shown on the immediate postoperative radiograph. The pin ends were bent against the iliac wings to prevent pin migration. The fragment of the ischial fracture was visible caudolateral to the left hemipelvis. (c) Lateral view of the postoperative radiograph showing the pin positioning and the ischial fracture fragment
Postoperative radiographs of the pelvis were taken to assess the reduction of the SI joint, the size of the pelvic canal and the implant positioning (Figure 2). SI joint reduction was assessed as described in Raffan et al 10 and in DeCamp and Braden; 20 it is defined as a percentage of the cranial to caudal length of the iliac joint surface that is in contact with the sacral articular surface. The pre- and postoperative pelvic canal diameter ratios (PCDR) were also measured to assess the improvement of the pelvic canal postoperatively. It was measured as described by Tonks et al 21 and Averill et al: 22 pelvic canal width at the cranial aspect of the acetabulum divided by caudal width of the sacrum (Figure 3). The hemipelvic canal ratio was obtained in each case postoperatively to detect lateralisation or medialisation of the luxated hemipelvis. 22 This was defined as the ratio of hemipelvic canal width on the SI luxation side divided by the opposite hemipelvic width. 22
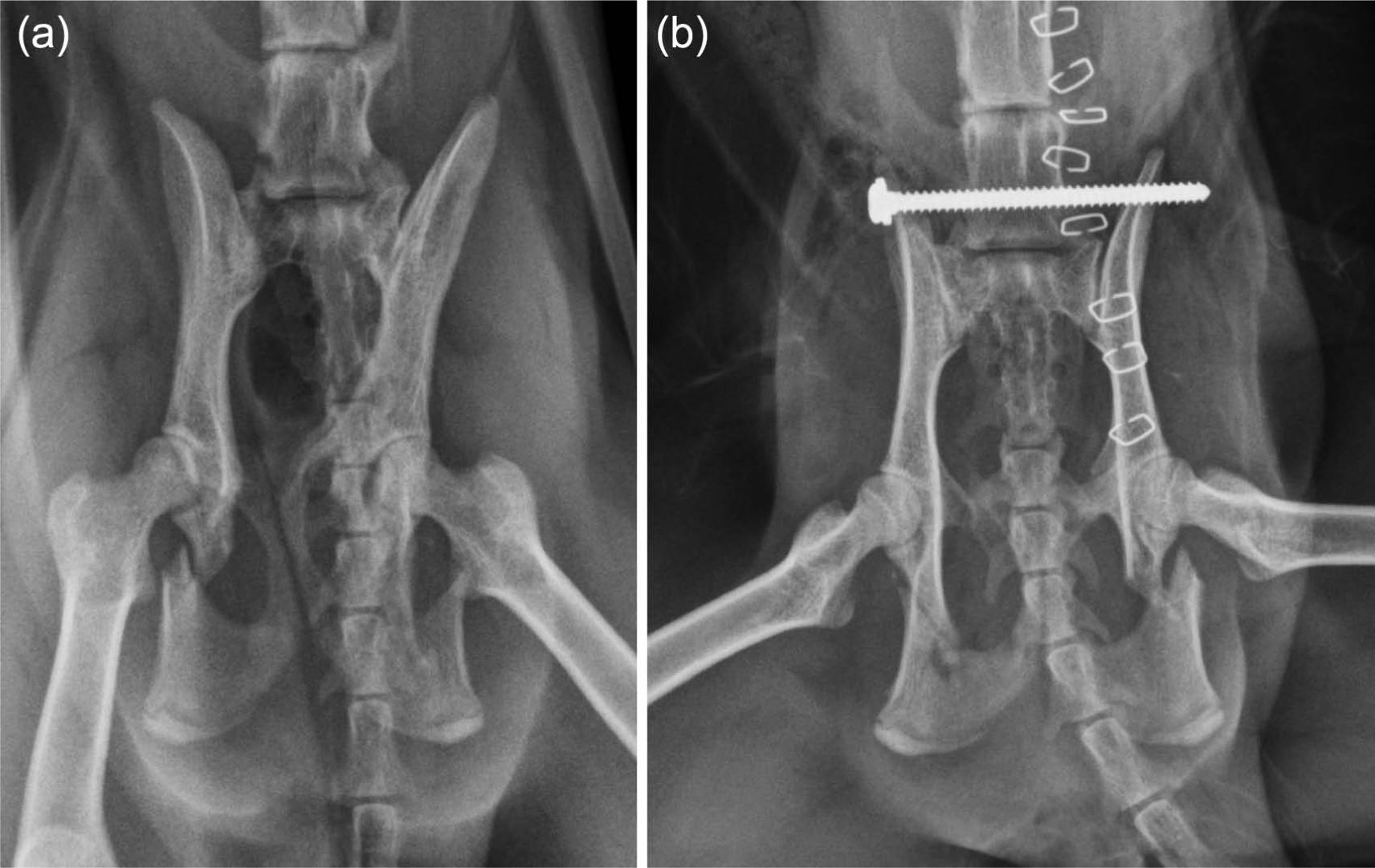
(a) Pre-operative radiograph showing sacroiliac (SI) luxation, bilateral ischial fractures and pelvic canal narrowing in cat 6. (b) The SI luxation was stabilised with a cortical screw applied as a trans-iliac screw. The screw end was secured with a nylon nut (which is radiolucent) to prevent screw loosening
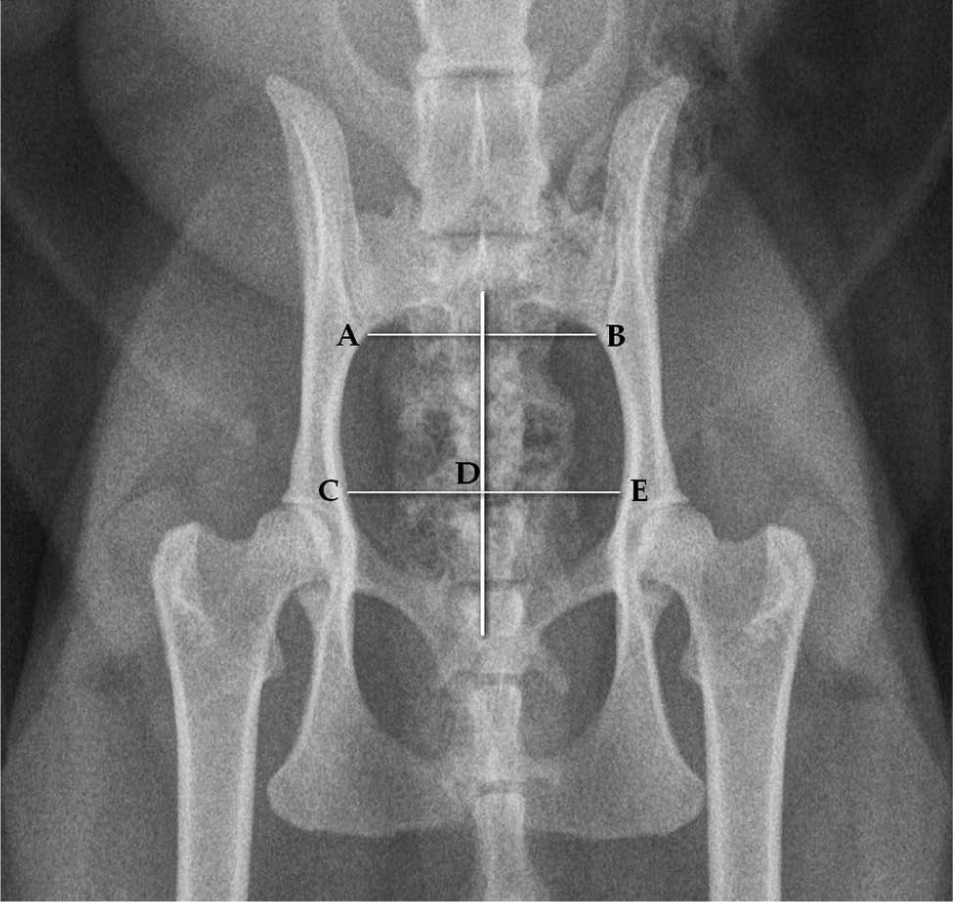
Pelvic canal ratio is the ratio of C to E distance over A to B distance. Hemipelvic canal ratio is the ratio of C to D distance over D to E distance (assuming C to D distance is on the luxated hemipelvis)
All cats were closely monitored for voluntary urination and defecation, improvement or deterioration of any neurological deficits, and use of the affected leg postoperatively when compared with pre-operative presentation. Complications were assessed through veterinary examination and/or follow-up radiographs.
Results
Background
Five domestic shorthair cats and one oriental cat (Bengal) were included in this study. There were three males and three females. The mean age at the time of surgery was 5 years 5 months (range, 1 year 2 months–11 years). Sex, breed, age, injuries, surgical time, implants used, follow-up time and complications were recorded (Table 1).
Owner questionnaire
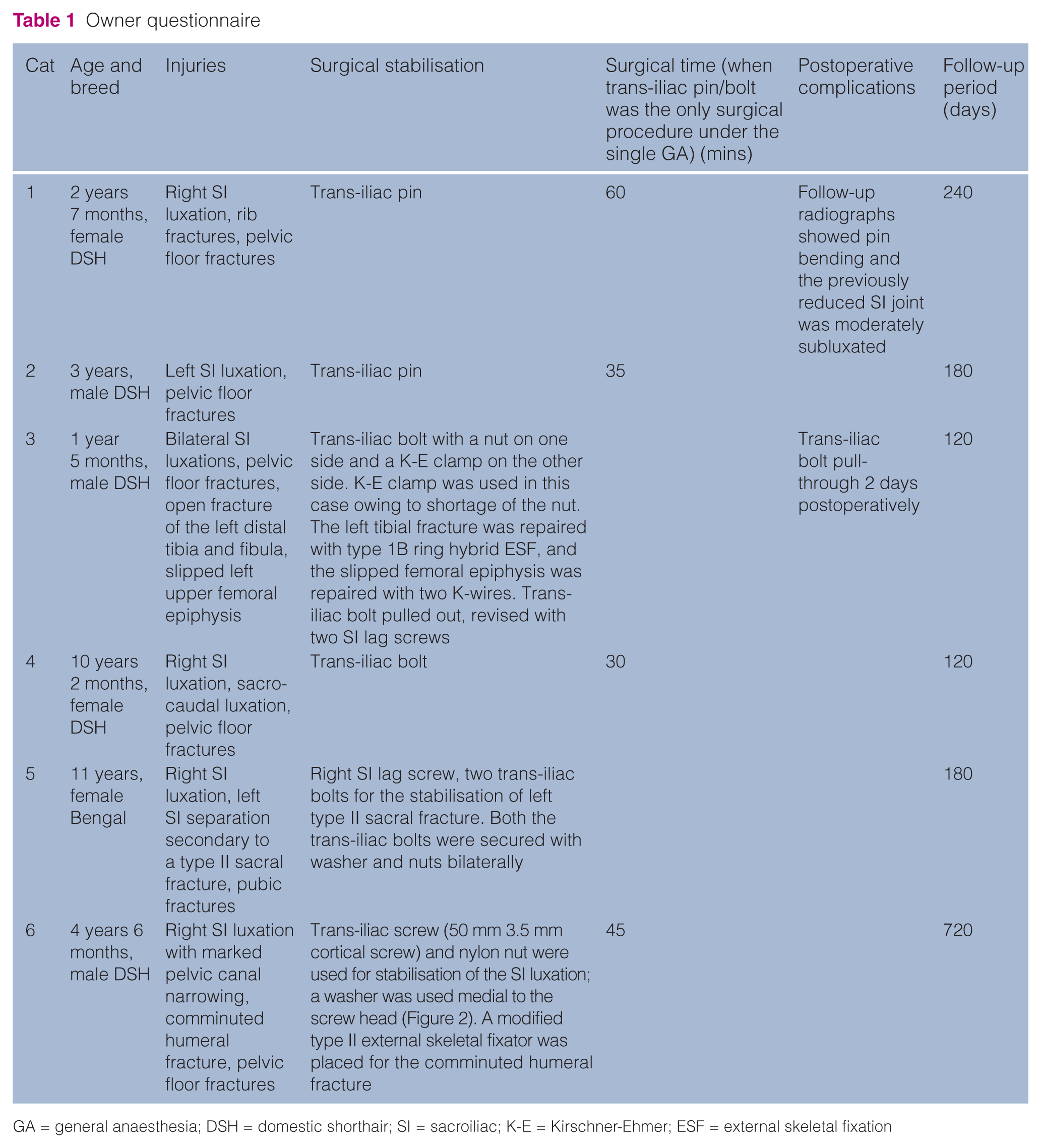
GA = general anaesthesia; DSH = domestic shorthair; SI = sacroiliac; K-E = Kirschner-Ehmer; ESF = external skeletal fixation
The surgical stabilisation had failed 2 days postoperatively in cat 3. As a result, it was not included in the pre- and postoperative objective measurements. Objective measurements used in this study included SI joint contact, PCDR and hemipelvic ratio, which are presented in Table 2.
Objective measurements of the radiographic assessment pre- and postoperatively

SI = sacroiliac; PCDR = pelvic canal diameter ratio
Cat 3 was removed from the objective assessment owing to the implant failure and subsequent stabilisation of the SI luxations with SI lag screws
Pre- and postoperative ambulation
Pre-operatively, cat 1 was non-ambulatory on the hind limb ipsilateral to the SI luxation; cats 3 and 5 had bilateral SI luxation/separation and were able to stand when supported. All cats were weight-bearing on the affected hind limbs within 1 day postoperatively, except for cat 3. Cat 3 had a tibial fracture and slipped femoral capital epiphysis in addition to bilateral SI luxations.
Neurological deficits
Urinary function was questionable at the time of surgery in two cats (cats 3 and 5). Cat 3 urinated voluntarily on day 1 postoperatively; the urinary catheter was removed the day after the surgery in cat 5, and voluntary urination was observed the same day. Cat 4 did not have voluntary urination pre-operatively, but regained voluntary urination on day 3 postoperatively. Two cats (cats 1 and 4) had reduced sensation or flaccid tail tone. Anal tone was not recorded for cat 1, but was present in cat 4. This was improved on postoperative recheck on day 32 for cat 2 and day 42 for cat 4.
Surgical time
The surgical time for cats 1, 2, 4 and 6 were used to calculate the surgical time for trans-iliac pin/bolt placement; these cats were selected because the trans-iliac stabilisation was the only procedure performed under the single general anaesthetic. Cat 3 had tibial fracture repair and cat 5 had a SI lag screw placement for the contralateral SI luxation under the single general anaesthetic. The mean surgical time for the included cats was 42.5 mins (30–60 mins).
Complications
Trans-iliac pin bending (cat 1) and fracture of the iliac wing with subsequent trans-iliac bolt migration (cat 3) were observed in two cats. The trans-iliac bolt in cat 3 had failed 2 days after the surgery and migrated dorsally through the fracture of the left iliac wing dorsal to the trans-iliac bolt. The bilateral SI luxations were subsequently stabilised with bilateral SI lag screws.
Follow-up
All of the owner questionnaires were returned and all clients were satisfied with the clinical outcomes of the cats. Cat 3 was removed from the follow-up because the SI luxations were re-stabilised with bilateral SI lag screws. Bilateral SI lag screws were chosen in the revision surgery in this cat owing to concern of further iliac wing fracture and subsequent implant migration if another trans-iliac device was used. The mean follow-up period was 288 days (120–720 days).
All the cats showed normal walking and running during medium-term (cats 1, 2, 4 and 5) or long-term (cat 6) follow-up. Three cats had an excellent outcome and two cats (cats 5 and 6) had a good outcome. According to the owners, none of the cats required long-term analgesia.
Cat 5 had regular gait abnormality in the hind limbs during walking and running, and there was a reduced jump height. Cat 6 had a slight difficulty in all the listed activities (running, climbing, walking and jumping). The slight difficulty was only noted occasionally in cat 6 during running and walking; it was more frequently noted in climbing and jumping.
All other cats were reported to be walking, running, climbing and jumping normally, except for cat 4, where a slight, occasional difficulty in climbing and jumping was noted.
Cats 1, 2, 4 and 5 had outdoor access and the voluntary outdoor activity was observed at a frequency similar to pre-injury in cats 1, 2 and 4. Cat 5 was observed to have a reduced frequency of outdoor activity.
Discussion
Trans-iliac pins or bolts have been used as a sole stabilisation technique for SI luxation and separation in dogs.18,23 Although it has been suggested as a sole treatment option in cats, 24 there are no published reports of the use of this technique in cats. Kudnig and Fitch 17 recommended the use of a trans-iliac brace as an adjuvant treatment in injuries where an additional method of stabilisation may be beneficial, such as comminuted sacral fractures where the landmarks for lag screw fixation are obscured.
Trans-iliac SI stabilisation is considered a simple technique for SI stabilisation with a low risk of entering the vertebral canal placement when compared with SI lag screw placement. 18 With the placement of SI lag screw, the implant has to travel through a narrow safe drill corridor to remain intra-osseous. 3 In cats, the safe drill corridor is small, often <0.5 cm2 and the appropriate drill angles are difficult to achieve.3,25 According to Burger et al, 3 there is a tendency to position the drill bit at a perpendicular angle to the articular surface, which will result in a cranial exit of the drill bit into the lumbosacral disc space or a ventral exit to the sacral body. The close proximity of this narrow path to important neurovascular structures also makes it a challenging procedure without the guidance of fluoroscopy. 3 In a retrospective study in dogs, incorrect placement of SI lag screw was noted in 67% of the dogs treated. 26 Incorrect placement of the screw may result in injury to the cauda equina, damage of the median sacral vessels and/or increase risk of screw loosening due to suboptimal purchase with the sacral body.20,25,27,28 Laceration of the median sacral vessels has not been reported as a complication of SI stabilisation. In comparison, the application of a trans-iliac pin/bolt may be safer as it is not in close proximity to major neural or vascular structures. Adjustments in implant direction are also relatively easy with trans-iliac implant owing to the bigger safe drill corridor. 10 Another potential advantage of trans-iliac implant over the SI lag screw is the reduced risk of sciatic and femoral nerves injury from pressure potentially exerted on the nerve when the ilium is levered below the sacrum to expose the sacral articular surface. 29
The surgical time for the trans-iliac pin/bolt placement in this retrospective study was a mean of 42.5 mins (range 30–60 mins) from first skin incision to skin closure, which, in our experience, is shorter than the time taken for SI lag screw placement. Correct placement of the SI lag screw in the sacrum can be technically challenging as the pilot hole in the sacrum cannot be visualised after the SI joint has been reduced. Long surgical and anaesthesia times increase the risk of anaesthetic complications such as hypothermia and cardiac arrhythmia, and increase the postoperative infection rate.30,31
Raffan et al 10 described a technique of SI pinning with supplemented tension band suture across the iliac wings. This technique was described as a simpler and safer alternative to SI lag screw placement. 10 In this technique, the compression and reduction of the SI joint were maintained by simultaneous pressure on the SI joint from the coxofemoral joint caudally and the tension band ligature cranially and the friction of the luxated surfaces of the SI joint. 10 In our opinion, when a trans-iliac pin/bolt is used as a sole stabilisation, it provides similar stabilisation forces during weight bearing. Based on the findings of our study an additional sacroiliac pin or screw was not needed for additional stability in the trans-iliac pin/bolt technique. We speculate that the friction generated at the sacroiliac junction by stabilisation and compression of the iliac wings is sufficient to prevent significant cranio-caudal and dorsoventral displacements of the luxated hemipelvis. However, strict confinement for a period of at least 6 weeks was recommended.
Previous studies have shown that 27–46% of the SI luxation cases are bilateral.2,4,25 Trans-iliac pinning has been reported as a sole method of stabilisation for bilateral SI luxations in dogs, 18 but similar reports in cats are lacking. According to Kaderly, 4 the placement of bilateral SI lag screws of appropriate size in bilateral SI luxations cases can be challenging, especially in cats, owing to the small size of the first sacral body. If shorter screws are chosen to accommodate for the bilateral insertion of lag screws in the sacrum, the risk of screw loosening increases significantly; up to 38% of screws with less than 60% purchase of the sacral body were found to be loosened on retrospective study. 26 In these cases, a unilateral lag screw with a trans-iliac pin/bolt (cat 5) or a single trans-sacral screw are viable treatment options. Further study is needed to compare the clinical outcome of unilateral lag screw with a trans-iliac pin/bolt and a single trans-sacral screw for the stabilisation of SI luxation in cats.
The PCDR improved significantly in postoperative radiograph in cat 6. If conservative treatment was chosen in cat 6, the potential complications include future displacement of the pelvic fragments, constipation, obstipation and megacolon. The postoperative PCDR in cats 4 and 5 was less than the pre-operative PCDR. We hypothesise that the pre-operative PCDR was slightly increased owing to the mild bilateral or unilateral lateralisation of the hemipelvises (increased C to D distance value in Figure 3). The CD value and the PCDR reduced postoperatively after compression across the SI joints.
The hemipelvic canal width ratio on the postoperative radiographs was calculated to detect lateralisation or medialisation of the luxated hemipelvis after the surgery. 22 The mean hemipelvic canal width ratio was 0.96 (range, 0.89–1.04); this indicates that there was minimal lateralisation or medialisation of the hemipelvises in the studied cats after the trans-iliac pin/bolt stabilisation.
Reported neurological deficits associated with SI luxations/separations include femoral and sciatic nerve deficits with associated knuckling or dragging of the foot, inability to urinate and to defecate, reduced or absence of anal tone, reduced sensation of the perineal area, and a flaccid or paralysed tail.6,10,32,33 Damage to the L6 and L7 nerve roots secondary to cranial displacement of the ilium in SI luxations have also been reported.6,7 Neurological deficits were present in 2/6 cats in this study; these include the inability to urinate, reduced sensation to the tail and flaccid tail tone. Inability to urinate resolved within 3 days postoperatively, and the tail tone and sensation were regained within 42 days postoperatively. The neurological deficits could be attributed to neuropraxia and/or axonotmesis of the cauda equina contributing to the coccygeal, pelvic and pudendal nerves. Both neuropraxia and axonotmesis could result from trauma and local compression of nerve. 34 Recovery from neuropraxia usually occurs within 1–2 weeks, but may take longer (up to 5–6 weeks). The recovery from axonotmesis can vary depending on the severity of the injury, but usually at 1 mm/day. 34
Pin migration was not observed in our study, despite it being a reported complication. 18 The pin migration was likely to be prevented by bending the pin ends against the iliac wings bilaterally if a smooth pin was used. Trans-iliac pin-bending (cat 1) and trans-iliac bolt migration (cat 3) were observed in two cats. In cat 1, the pin was bent and the previously reduced SI joint was moderately subluxated. Despite this, the cat was doing clinically well, and could walk without obvious gait abnormality and could jump. In cat 3, the left iliac wing had fractured dorsally to the trans-iliac bolt, which had migrated dorsally. This cat had bilateral SI luxations and a revision surgery with bilateral SI lag screws was performed. The iliac wing fracture and implant migration were likely to be caused by a combination of factors: large size of implant, the trans-iliac bolt entering the iliac wing too dorsally and the increased motion at the implant-bone interface due to the bilateral nature of the injuries. This cat was one of the two cats that had bilateral SI luxations/separations. Caution should be exercised in the use of a trans-iliac pin/bolt as the sole fixation in these cases.
Behavioural changes associated with joint pain in cats can be subtle and easily missed. 35 As a result, questionnaire-based outcome measures can guide owners in assessing their cat’s mobility, especially those that are altered by degenerative joint disease-associated pain, such as jumping, running, climbing and reduced height of jump. 35 All the questionnaires were returned and all the owners were satisfied with the clinical outcomes of the cats. Three of the five cats (cat 3 excluded) had an excellent outcome; they did not show, or only occasionally showed, signs associated with the injuries. Two cats had a good outcome (cats 5 and 6); the total disability scores for these cats was 6. The main signs of difficulty were a slight, but frequent, difficulty or abnormal gait in walking, running, jumping and climbing, and reduced height of jump. The abnormal gait and reduced height of jump in cat 5 could be attributed to the bilateral nature of the SI injuries and old age (11 years of age). Cat 6 sustained a comminuted humeral fracture, as well as the SI luxation and pelvic floor fracture. The multi-limb injuries could have contributed to the increase disability score. Similar to cat 5, the reduced height of jump noted in cat 4 might be attributed to the pelvic injuries, as well as degenerative joint disease, given the age of the cat (10 years and 3 months). According to the owners, none of the cats required long-term analgesia.
The limitation of this study arises from its small number of studied animals and its retrospective nature. The small number of recruited cases is likely to reflect the preference of surgeons to either manage these cases conservatively or to treat them with other surgical stabilisation, such as SI lag screws. Owing to the retrospective nature of the study, important information, such as pre- and postoperative pain scores, was not recorded in all cases. Another limitation of the study is the fact that the injuries in the studied cats were different and the management was not standardised. This could affect the clinical outcome of the cats. The third limitation of this study is the lack of veterinary examination in our long-term assessment. Veterinarians may pick up subtle lameness from thorough orthopaedic examination, which may be overlooked by the owners. Instead of a veterinary examination, we included an owner questionnaire for each case to assess medium to long-term outcome. Lifestyle changes, such as willingness to jump, have been shown to be a good indicator of lameness in cats. 36 Assessment of pain in cats can be difficult as they appear to be less demonstrative than dogs. 36 As a result, the requirement for analgesia in the studied cats might be underestimated.
Conclusions
Trans-iliac pin, bolt or screw is a safe and simple surgical treatment for SI luxation or separation in cats. In most cases, the functional outcome was excellent with this technique and postoperative complications were minimal. According to the owner questionnaires, all the cats have a good clinical outcome and quality of life.
Supplemental Material
Click here for Supplementary Material
Questionnaire scoring activity
Footnotes
Supplementary data
Questionnaire scoring activity.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case series.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.