
Abstract
An 8-year-old intact male Persian cat was presented for investigation of chronic haematuria. The cat had episodes of haematuria on several occasions that were non-responsive to antimicrobial therapy. Abdominal ultrasound examination revealed dilation of the renal pelvis and ureters of both kidneys. The urinary bladder wall was thickened, a mass of heterogeneous echogenicity filled the lumen of the bladder, and two parallel thin hyperechoic lines were identified within the lumen, which suggested a urethral catheter. Differential diagnoses for the urinary bladder mass included cystitis and neoplasia. The mass was surgically removed from the urinary bladder, and a urethral catheter was found embedded in the mass. Histopathological findings were consistent with cystitis glandularis of a typical type. Periodic bladder ultrasonographic studies were performed; at the time of writing, over 2 years later, recurrence had not been detected.
Case Report
An 8-year-old intact male Persian cat was presented to the University of Murcia Veterinary Teaching Hospital, Murcia, Spain, for investigation of chronic haematuria. The cat had been previously diagnosed as having lower urinary tract disease; within the last 2 years the cat had episodes of haematuria on several occasions. The patient was treated with amoxicillin–clavulanate (20 mg/kg, PO, q12h for 15 days, repeatedly) by the referring veterinary surgeon without apparent improvement. On physical examination, the animal showed a good body condition (6/9), with normal hydration and vital parameters. The results of the haematological analysis were unremarkable. On serum biochemistry blood urea nitrogen was slightly increased (55 mg/dl; reference interval 20–50 mg/dl) and a mild increase in alanine transaminase activity (127 U/l; reference interval 31–88 U/l) was also noted. Urinalysis revealed appropriate urine concentrating ability (urine specific gravity >1.050) with haematuria (>100 red blood cells per high power field).
Abdominal radiographs showed no remarkable findings. Abdominal ultrasound examination revealed dilation of the right (9 mm) and left (3 mm) renal pelvis and ureters. The bladder wall was thickened (6 mm) and a mass of heterogeneous echogenicity with anechoic areas that filled the lumen of the bladder was observed (Figure 1a). Power Doppler mapping was used to assess vascularity of the mass that was increased. Differential diagnoses for the urinary bladder mass included neoplasia and polypoid inflammatory tissue. Two parallel thin hyperechoic lines were identified within the lumen, which suggested a urethral catheter (Figure 1a).
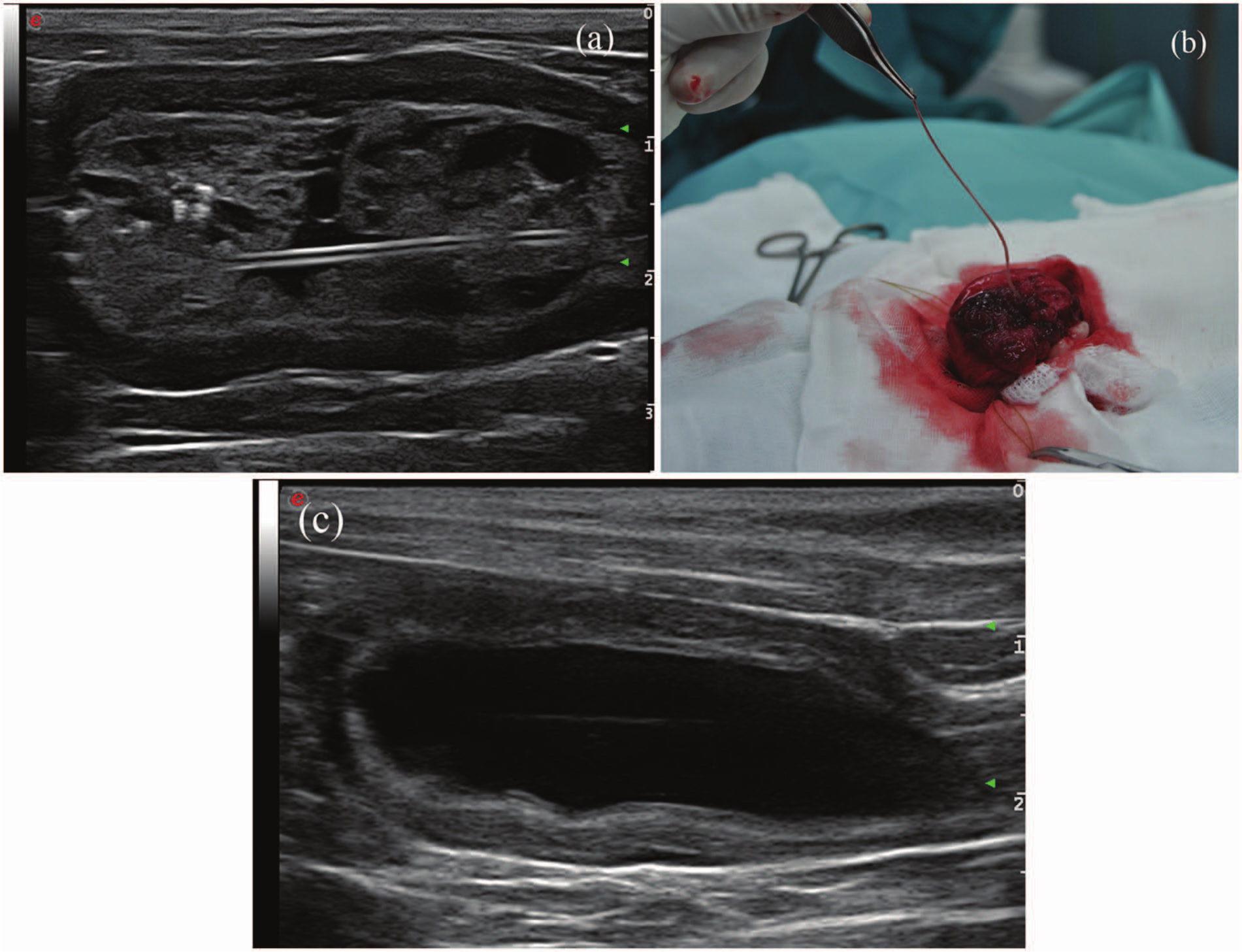
(a) Longitudinal ultrasonographical image of the urinary bladder. The bladder wall is thickened and a mass of heterogeneous echogenicity with anechoic areas that filled the lumen of the bladder is observed. Two thin parallel hyperechoic lines are observed within the lumen, which suggested a urethral catheter. (b) Intraoperative photograph. The mass arising from the whole bladder wall was surgically removed from the urinary bladder. A urethral catheter was found embedded in the mass. (c) Longitudinal ultrasonographical image of the urinary bladder, 2 months after surgery. The ultrasonographical appearance of the bladder wall is thickened
A laparotomy was performed under general anaesthesia. The cystotomy revealed a large mass arising from the whole bladder wall extending along the bladder neck and covering both ureteric orifices. The mass was surgically removed from the urinary bladder, and a urethral catheter was found embedded in the mass (Figure 1b). A sample of the mass was submitted for histological evaluation and bacteriological culture. Histopathological findings were consistent with cystitis glandularis (CG) of a typical type with severe chronic inflammation of the lamina propia. No evidence of malignancy was observed (Figure 2). Results of bacteriological culture of the urinary bladder biopsy samples indicated growth of Staphylococcus species, which was susceptible to marbofloxacin.
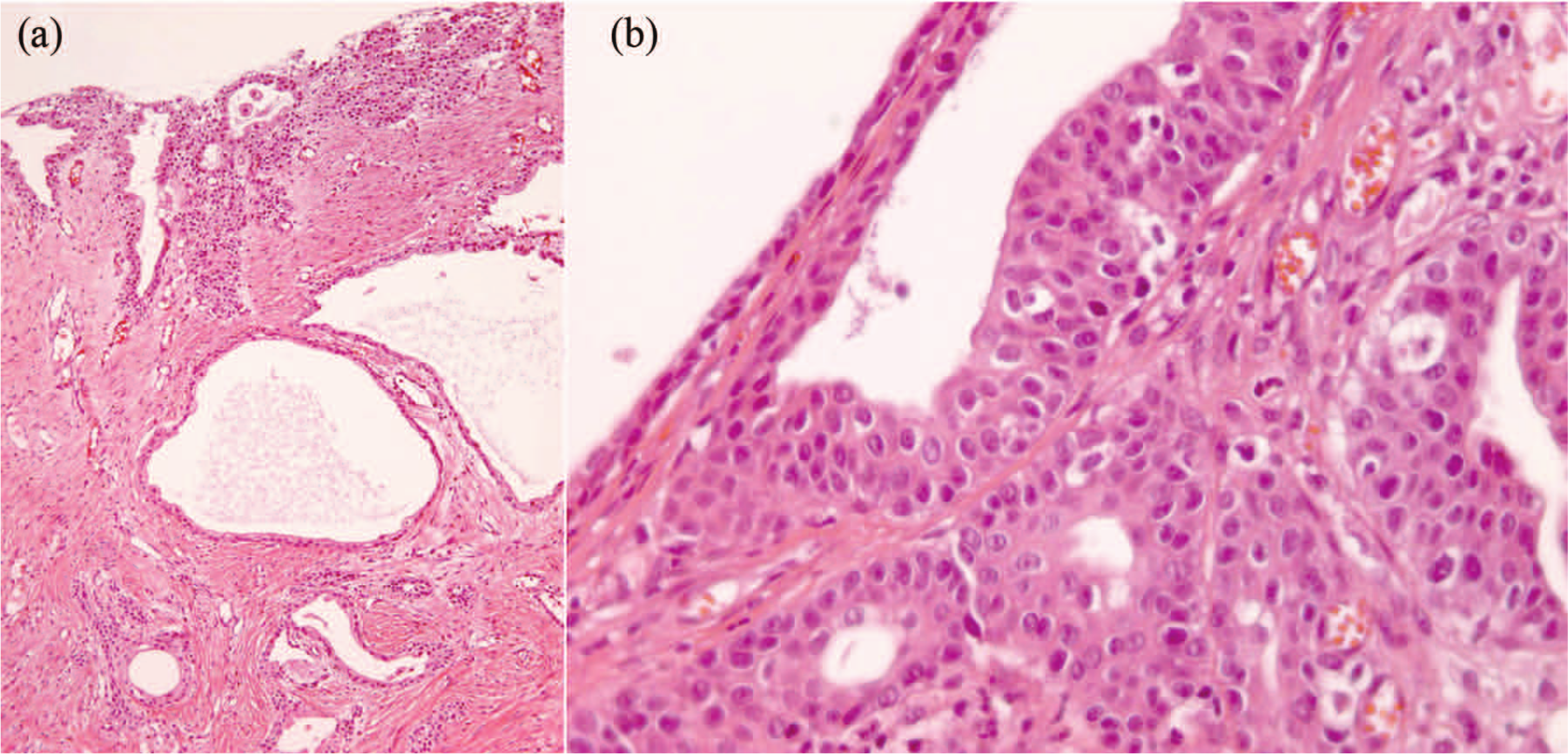
(a) Histopathology of the mass removed from the urinary bladder (haematoxylin and eosin stain, 10×). The lining is composed of columnar epithelial cells, associated with cysts of various sizes. (b) Close-up (40×) of the appearance of the cyst. No cytological atypia is noted. There is no evidence of intestinal metaplasia
The cat recovered uneventfully from the anaesthesia and surgery, and it was discharged from hospital 2 days later. Marbofloxacin (2 mg/kg, PO, q24h) (Marbocyl; Vetóquinol) was prescribed for the following 10 days. Ultrasound scans were performed periodically and a gradual improvement of the appearance of the bladder wall with a progressive decrease of both pelvis renal dilatations was observed. Two months after surgery, the cat had ultrasonographically normal kidneys and moderate thickening of the bladder wall (Figure 1c). Two years later, no new growths of the mass or malignant changes have been observed.
This case report documents a typical glandular cystitis, causing obstruction of both uretervesicle junctions leading to hydronephrosis in a cat. CG is a benign inflammation of the bladder, characterized by von Brunn’s nests that grow into the lamina propria forming cysts and/or metaplastically changing into globet cells. 1 CG has been rarely reported in small animals.2,3 To our knowledge, only one case of CG has been previously reported in a cat. 2 However, this report is the first description of CG leading to bilateral hydronephrosis in a cat.
The aetiology of CG is unknown, but chronic bladder infection and inflammation are postulated to be the main risk factors for the development of CG, 4 and chronic bladder irritation is the most common complaint in patients with this condition. 5 In the present report, the origin of the CG was the urethral catheter found into the bladder, which was presumably placed when the cat had a lower urinary tract disease 2 years previously. The catheter developed a chronic irritation and inflammation of the bladder mucosa, leading to the over-productive changes in the mucosal cells and glandular metaplasia of transitional epithelial cells. 5 The lesions involved the whole bladder wall, the urinary bladder neck and both uretervesicle junctions. The masses obstructed the bladder neck and infiltrated the ureters leading to hydroureters and hydronephrosis. However, the lesions of CG are more frequently localized at the bladder neck or on the trigone, and less common on the lateral bladder walls or in the urethra, pelvis and ureter. 6
In agreement with our observations, the most common clinical signs of CG are chronic haematuria2,3 and signs of chronic bladder irritation, such as frequency and dysuria. 6 In rare cases, CG may cause obstructive urinary signs,4,7 as in the present case.
The ultrasonographical appearance of CG is observed as masses arising from the bladder wall. However, these lesions cannot be distinguished from other conditions, such as simple inflammatory and neoplastic lesions, and biopsy is necessary in order to achieve the definitive diagnosis. 5
The treatment of CG consists of removing the source of irritation and eradication of urinary infection with long-term antibiotic administration, 5 although surgical treatment may be indicated in symptomatic patients, such as this cat. 7 Recurrence and progression from CG to adenocarcinoma of the bladder, 8 particularly the intestinal type, 5 have been reported. In our case, periodic bladder ultrasonography was performed and after 2 years recurrence has not been detected.
Conclusion
CG is a rare condition in cats. The ultrasonographical appearance resembles a bladder malignancy lesion, and the diagnosis is achieved by histology.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.