
Abstract
A 5-year-old, female neutered Persian cat was admitted to the Small Animal Hospital (Chulalongkorn University, Bangkok, Thailand) with clinical signs of dysuria, haematuria and partial urethral obstruction that had manifested over several months. The animal also had hyperkalaemia and severe azotaemia at the time of presentation. Urinalysis showed haematuria, pyuria and the presence of several transitional cells. In addition, ultrasonography demonstrated an extraluminal mass between the neck of urinary bladder and the colon. Fine-needle aspiration of the mass revealed a fungal form with branching and septate hyphae. Consequently, itraconazole treatment was prescribed and clinical signs of improvement were seen after 7 days. However, 1 month later, the cat died of acute anaemia. Necropsy revealed the presence of extraluminal multifocal fungal granuloma at the neck of the urinary bladder, and contracted kidneys. Histopathological analysis of the fungal granuloma was found to be composed of branching, septate hyphal fungi together with inflammatory cells. Subsequent fungal culture and identification revealed this to be a species of Penicillium.
Case Report
Feline lower urinary tract disease is essentially an inflammatory condition where the clinical signs, which include haematuria, dysuria, pollakiuria and/or urethral obstruction (for the non-inflammatory form the clinical signs are haematuria, dysuria, stranguria and pollakiuria), may present with or without urethral obstruction. 1 The incidence of urinary tract infection (UTI) in cats is around 3–4% of the feline population 2 and can be induced by either bacteria, virus or fungi. 3 However, fungal infection of the urinary tract in cats is very rare, and final diagnosis is often by histopathological evaluation made at the time of post-mortem examination. Nonetheless, there are several reports of fungal cystitis in small animals primarily due to infection by species of Aspergillus, and Candida and Cryptococcus neoformans. 4 Furthermore, in humans, infection by Penicillium species is generally considered as opportunistic and to occur more frequently in immunocompromised patients. 5 However, in domestic animals, infection by Penicillium species is uncommon, with the exception of a few reports in cats where the bacteria were isolated and identified as the cause of clinical signs of rhinitis, 6 rhinitis and sinusitis, 7 and orbital cellulitis, sinusitis and pneumonitis. 8 In this study we report a case of a cat suffering from chronic dysuria, haematuria and partial urethral obstruction induced by extraluminal fungal granuloma at the neck of the urinary bladder.
A 5-year-old, strictly indoor, female neutered Persian cat weighing 2.6 kg was referred to the Small Animal Hospital, Faculty of Veterinary Science, Chulalongkorn University, Bangkok, Thailand, with a history of dysuria, haematuria, partial urethral obstruction and chronic cystitis. The cat was treated with antibiotics for lower UTI and received supportive treatment for a few weeks at a previous clinic, but clinical signs did not improve.
On the first day of presentation, the cat’s body condition score was 2/5 with 7% dehydration and difficulty urinating. The urinary bladder was distended and the urine was mildly turbid. Heart and lung sounds were within normal limits. The oral mucous membrane was pale and the cat’s coat was dull. Venous blood gas results revealed metabolic acidosis with an increase in anion gap and respiratory acidosis (Table 1). The cat also had hyperkalaemia (4.92 mmol/l; normal range 3.4–4.5 mmol/l). Blood chemistry results demonstrated severe azotaemia [blood urea nitrogen (BUN) 151 mg%, normal range 14–28 mg%; creatinine 13.9 mg/dl, normal range 0.6–1.6 mg/dl]. Haematology results were within the normal range (Table 2). Urinalysis obtained by cystocentesis demonstrated isosthenuria, aciduria (pH 6), haematuria [10–20 red blood cells per high-powered field (HPF)], mild pyuria (leukocytes 5–10/HPF) and numerous squamous cells (10–15/HPF) (Table 3). Feline leukaemia virus antigen and feline immunodeficiency virus antibody tests (Snap FIV/FeLV Combo test; Idexx Laboratories), auto-agglutination and the Coomb’s test were all negative. Ultrasonography of the abdomen demonstrated an extraluminal mass (3 × 2.25 × 2.27 cm) between the neck of the urinary bladder and colon, resulting in compression of the neck of urinary bladder and in a marked bladder distention. The urinary bladder wall also showed mild thickening (2.7 mm). The renal pelvis and proximal ureter were dilated. Cytological preparation of this extraluminal mass was made by fine-needle aspiration using ultrasound guidance. The collected sample was stained with Giemsa, and the results showed branching, septate hyphae together with inflammatory cells (Figure 1).
Blood gas results of the cat on days 0, 1 and 67 of the follow-up
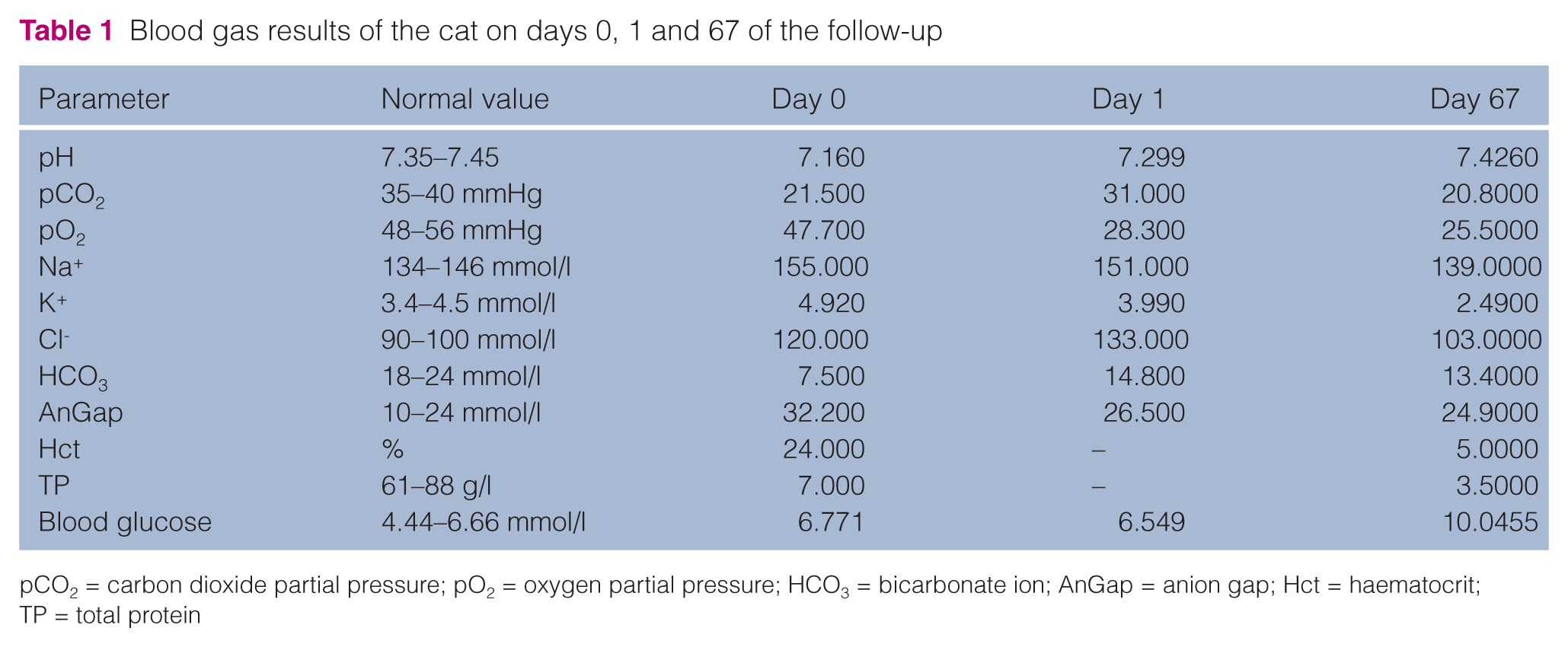
pCO2 = carbon dioxide partial pressure; pO2 = oxygen partial pressure; HCO3 = bicarbonate ion; AnGap = anion gap; Hct = haematocrit; TP = total protein
Haematology and blood chemistry results of the cat on days 0, 11, 22, 62 and 67 of the follow-up

Hct = haematocrit; MCV = mean corpuscular volume; MCHC = mean corpuscular hemoglobin concentration; ALT = alanine transaminase; ALP = alkaline phosphatase; BUN = blood urea nitrogen; Undiff = undifferentiated
Urinalysis results for the cat

WBC = white blood cells; HPF = high-powered field; RBC = red blood cells

Branching, septate hyphal fungi present among the inflammatory cells and red blood cells in (a) the fine-needle aspiration (Giemsa stain) and (b) the urine sample (40×)
The cat was treated with fluid therapy to correct the electrolyte imbalance and was given amoxicillin–clavulanic acid at a dose of 13.75 mg/kg q24h to control the infection. Blood chemistry indicated a lowered BUN and an increase in creatinine levels [BUN: 19 mg%; creatinine: 1.7 mg/dl (Table 2)] after the treatment. Itraconazole (5 mg/kg q24h) was given orally for 1 month and clinical signs of improvement were seen after 7 days. After this time, the cat was brought back to the hospital for re-evaluation. It was alert with normal appetite, but still presented with persistent pollakiuria. Ultrasonography demonstrated a slight decrease in size of the granulomous mass (2.28 × 2.58 × 2.35 cm), a mild irregular urinary bladder wall lining and small polyp (3 mm) at the dorsal wall of urinary bladder (Figures 2 and 3). There was dilation of the renal pelvis and proximal ureter of the right kidney with echogenic sediments in the renal pelvis (Figures 2 and 3). Pyelonephritis was also diagnosed. Marbofloxacin (2 mg/kg q24h) was prescribed according to the urine culture result. In the second month of treatment, the cat was returned to the veterinary hospital with signs of weakness, anorexia, polyuria and pollakiuria. Physical examination revealed pale oral mucous membranes, normal capillary refill time (CRT), dehydration <5% and a small-sized urinary bladder. Haematology results showed severe microcytic hypochromic anaemia, leukopenia (1300 cells/µl) and azotaemia (BUN 55 mg%; creatinine 2.2 mg/dl) (Table 3). Urinalysis demonstrated hypersthenuria (urine specific gravity 1.038) and the presence of fungal hyphae in the urine sample obtained by cystocentesis (Table 3 and Figure 1b). A urine sample was submitted for fungal culture. The cat died of complications and necropsy was subsequently performed.

The ultrasound showed non-remarkable appearance of the mass. It was 2.87 × 2.38 × 2.41 cm in size, located between neck of the urinary bladder (UB) and colon (a); right kidney hydronephrosis with right pelvis dilated (b)

The ultrasound showed a slight decrease in the size of the mass, 2.28 × 2.58 × 2.35 cm (a), and small polyps at the dorsal wall of urinary bladder (b). The right kidney had chronic pyelonephritis, hydronephrosis and hydroureter (c)
Gross pathological analysis revealed a large irregular yellow-brownish firm mass at the neck of the urinary bladder with multiple small yellowish masses protruding around the mucosa of urinary bladder and urethra (Figure 4a,b). Contracted kidneys with dilated pelvis were also diagnosed. The tissue biopsies were fixed in 10% buffered formalin, processed histologically, embedded in paraffin, and cut and stained with haematoxylin and eosin, periodic acid-Schiff (PAS) and Gomori methenamine silver (GMS). Histopathological analysis detected a multifocal fungal granuloma in the mass, urinary bladder and the urethral mucosa. The fungal elements were clearly demonstrated by PAS and GMS staining (Figure 5a,b). Additional histopathological analysis detected severe chronic interstitial nephritis, urethritis, mild periportal hepatitis and moderate erythrophagocytosis in lymph nodes and spleen. The fungal granuloma was cultured in special agar; fungal identification revealed the presence of Penicillium species.

A large, irregular, yellow-brownish soft mass present at the neck of the urinary bladder (arrow) (a) and multiple small masses present at the mucosa of the bladder (arrow) (b). UB = urinary bladder; Ur = urethra; Co = colon

(a) The fungal granuloma was composed of fungal hypha in the centre and was surrounded by macrophages and multinucleated giant cells (haematoxylin and eosin, bar = 50 µm). (b) The branching septate small hyphae are demonstrated clearly by periodic acid-Schiff staining (bar = 20 µm)
Fungal urinary tract infection in cats is very rare and can occur as an ascending infection from the environment to the genital mucosa. 4 Other causes may be from a secondary infection, or disseminated or systemic infection of the kidneys resulting in the shedding of the organism into the urine. 4 Many risk factors are postulated to result in fungal infection in cats, including immune suppression, and the long-term use of broad-spectrum antibiotics. 9 In this case, the primary route of fungal infection into urinary bladder was likely to be through eating a grass seed or through external penetrating trauma. Fungal causes of UTI have been reported in dogs and cats. The most common form isolated from dogs and cats is Candida albicans. 10
Penicillium species fungal granuloma invading into the urinary bladder in cats has never been reported, even though this fungus is found to be widely distributed in soil, grain, food and live stock feed. 11 However, in humans, Penicillium species has been isolated from patients diagnosed with pneumonia, keratitis, endophthalmitis, otomycosis, necrotising esophagitis, endocarditis, peritonitis, and UTIs. 11 In animals, penicillosis is an opportunistic infection commonly infecting the respiratory tract, skin, urinary tract and fight wounds. 12 Fluconazole has been proposed to be the treatment of choice for fungal cystitis, largely because it is readily eliminated by the kidneys; as a result sufficient bladder concentration can be achieved to effectively treat fungal infections of the bladder. 13 Fluconazole is excreted more readily into the urine than both itraconazole and ketoconazole. 4 Although fluconazole is proposed to have the highest efficacy against yeasts, it has been reported not to be a good choice for the treatment of filamentous fungi, such as Penicillium species, in cats. 14 Posaconazole, a triazole antifungal agent with a broad spectrum of activity, has been used successfully to treat invasive orbital aspergillosis in a cat 15 and Mucor species infection of the nose in one cat. 16 Removal of the granuloma and instillation of intralesional agents (amphotericin B or voriconazole) at the time of surgery in concert with follow-up antifungal therapy systemically with posaconazole may have been effective in an attempt to resolve this infection.
In the present study, the Penicillium species fungal granuloma caused chronic cystitis induced by partial urethral obstruction. Initially, the granuloma was located extraluminally on the neck of urinary bladder, but was later found to have invaded into urinary bladder wall, partially obstructing the urine outflow. Although the granuloma decreased in size over time with itraconazole treatment, ultrasonography showed a small polyp at the urinary bladder wall and urinalysis revealed the presence of fungal hyphae in the urine sample. These findings indicated that itraconazole treatment alone could not completely eliminate the Pencillium species fungal infection. In humans with AIDS-related complications, disseminated penicilliosis are generally treated with amphotericin B induction therapy (2 weeks) followed by itraconazole at the maintenance dose, which can achieve a response rate of more than 95%. 17 However, in the present study, the cat died of severe pancytopenia caused by chronic renal failure and internal haemorrhage from the granuloma. Furthermore, an informed decision was made not to treat the cat with amphotericin B, essentially becauase of its inherent toxicity. Instead, itraconazole alone was given as less than 1% is eliminated by the kidneys. 18 The cat died of severe complications of anaemia largely because itraconazole alone could not eliminate the Penicillium species infection resulting in the development of the granuloma.
Conclusions
Cats with extraluminal fungal granuloma of the urinary tract should be treated with surgical removal of the granuloma and given antifungal agents systemically to prevent complications.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.