
Abstract
Two cats had chronic respiratory signs associated with pulmonary carcinoma. In each case, computed tomography demonstrated similar pulmonary masses, pleural fluid and osteolytic expansile rib lesions as a result of local costal spread. This is the first report of feline primary pulmonary adenocarcinoma with local spread to the ribs, causing osteolysis. Although pleural involvement is common with this neoplasm, local spread to ribs is rarely reported.
Case Report
An 8.5-year-old male neutered Norwegian Forrest cat had diarrhoea and inappetence, bilateral nasal discharge, sneezing and tachypnoea. The cat was treated symptomatically for suspected bronchopneumonia with broad-spectrum antibiotics; however, dyspnoea gradually became more marked and the cat was referred 7 weeks after initial presentation. On referral, the cat was dependent on supplemental oxygenation. Thoracic computed tomography (CT) under general anaesthesia revealed marked diffuse thickening of the pleura, pleural fluid and soft tissue masses adjacent to the left second and third ribs (Figure 1). Both ribs had localised osteolysis and an irregular interrupted periosteal reaction just dorsal to the costochondral junctions. The proximal parts of the left second and third ribs, and the right third, fourth and fifth ribs were thickened by a continuous periosteal reaction. The right caudal lung contained a soft tissue mass with heterogeneous enhancement after intravenous contrast administration (Figure 2). The remaining lung lobes were partially collapsed, likely as a result of pleural fluid. Radiographs taken after the CT, to confirm placement of thoracic drains (Figure 3), show subtle rounded soft tissue and mineral opacities associated with the left second and third ribs, most noticeable on the dorsoventral view.

Transverse image (modified bone window) post-contrast administration of cat 1 showing pleural fluid (*) and soft tissue attenuating mass (between arrows) surrounding the left third rib. This rib is partially resorbed and has an irregular periosteal reaction
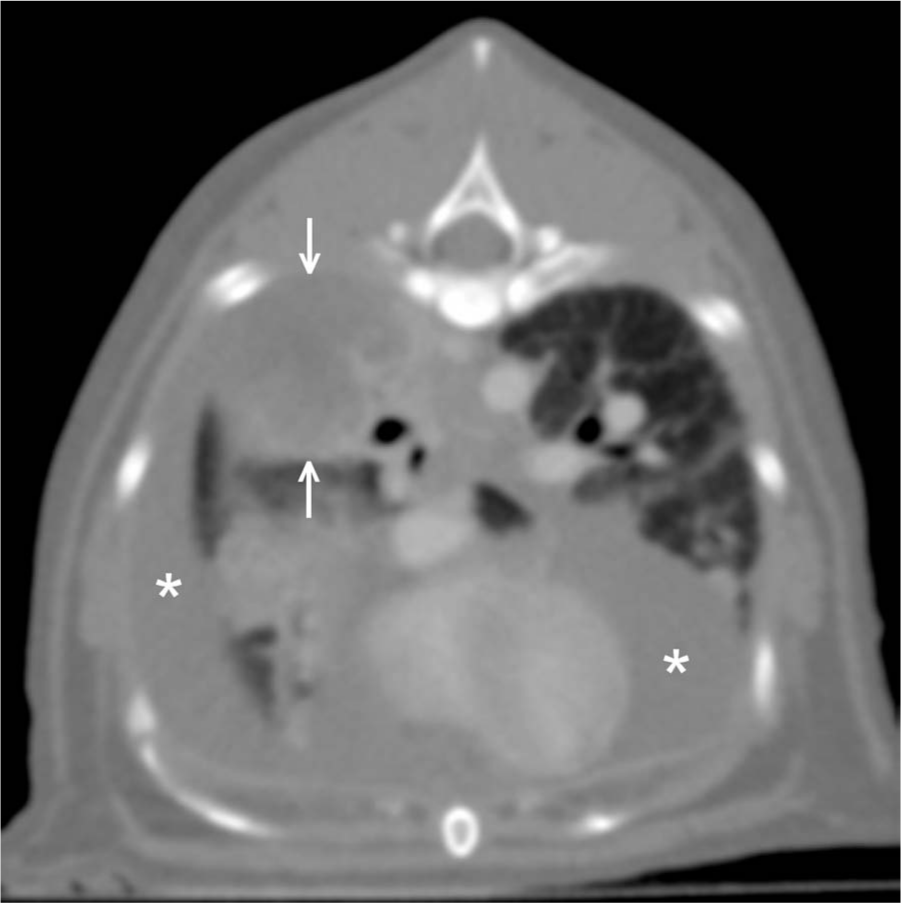
Transverse image (modified bone window) post-contrast administration of cat 1 showing pleural fluid (*) and soft tissue mass within the right caudal lung lobe (between arrows). The mass has faint heterogeneous enhancement

Left lateral (A) and dorsoventral (B) thoracic radiographs of cat 1 taken after computed tomography to confirm placement of thoracic drains. There are subtle rounded soft tissue and mineral opacities associated with the left second and third ribs
Cytology of the pleural fluid was consistent with an exudate with a total nucleated cell count of 5.3 × 109/l (72% neutrophils) and total protein of 25.4 g/l. Cytology following fine needle aspiration of the ribs was consistent with carcinoma. Pulmonary biopsy was compatible with adenocarcinoma. The cat was subsequently euthanased. Necropsy findings were compatible with pulmonary adenocarcinoma with intrapulmonary and pleural metastases and probable direct costal spread, secondary to apposition of the affected pleura.
A 13-year-old, female neutered domestic shorthair had a 3-week history of inappetence and weight loss. There was a leukocytosis and mature neutrophilia. The cat was treated with amoxicillin/clavulinic acid, but failed to improve and represented with dyspnoea and tachypnoea 3 weeks later. The cranial thorax was not deformable on palpation and a cranial mediastinal mass was suspected. Thoracic radiographs showed a right-sided pleural effusion and pulmonary consolidation. Approximately 150 ml of clear yellow pleural fluid was removed via thoracocentesis. After transient clinical improvement, the cat became progressively dyspnoeic and tachypnoeic again, and was referred for further investigation the following day.
Thoracic CT under general anaesthesia revealed osteolysis and irregular interrupted periosteal reaction affecting the ventral half of the right second rib and the left third rib. Surrounding these ribs were rounded soft tissue masses that extended mainly laterally into the axillary region. These masses had moderate irregular peripheral enhancement after intravenous contrast administration (Figure 4). The left fifth rib was thickened by a spiculated periosteal reaction and was also surrounded by a soft tissue mass with peripheral enhancement. A soft tissue mass 2 cm in diameter containing multiple small gas foci was identified in the right caudal lung lobe (Figure 5). In the abdomen, mesenteric lymph nodes were enlarged (0.7 mm thick) and there was a hypoattenuating nodule 4 mm in diameter within the liver that did not enhance after intravenous contrast administration.

Transverse image (bone window) post-contrast administration of cat 2 showing soft tissue masses (m) with peripheral enhancement surrounding the right second rib (2) and the left third rib (3). These ribs show marked lysis and spiculated to amorphous periosteal new bone (arrow)

Transverse image (modified bone window) post-contrast administration of cat 2 showing a mixed soft tissue and gas-attenuating mass within the right caudal lung lobe (between arrows) with heterogeneous contrast enhancement. Pleural fluid (*) is present within the ventral aspect of the thorax and surrounding the mass
Cytology of the pleural fluid was consistent with a neutrophilic exudate with a total nucleated cell count of 12.1 × 109/l and a total protein of 22.6 g/l. Biopsy of the right third rib lesion was compatible with adenocarcinoma. The cat was euthanased. Following necropsy a primary pulmonary bronchogenic adenocarcinoma was identified with metastases to the liver, pericardium and thoracic wall, as well direct spread to the ribs (Figure 6).

Histological preparation from cat 2 showing islands and nests of neoplastic epithelial cells (arrows) infiltrating the rib with marked chondroid and osseous destruction, and remodelling
Feline primary pulmonary carcinoma accounts for <1% of feline neoplasms presenting to veterinary hospitals.1,2 The average age at diagnosis of cats with pulmonary carcinoma is 11–13 years. 1 The most common type of pulmonary neoplasia in cats is adenocarcinoma 3 with squamous cell carcinoma, adenosquamous cell carcinoma, sarcomas and benign tumours being less common.2,4,5 The radiographic features of feline pulmonary carcinoma are very variable.4,6 Tumours may appear as homogenous lobar consolidation, a diffuse infiltrate with a patchy alveolar or diffuse peribronchial or nodular pattern, or both. There may be a single or multiple well-circumscribed masses, sometimes with evidence of calcification or cavitation.4,6,7 Cavitation has been associated with adenocarcinoma and may represent a necrotic centre. 7 The most common extrapulmonary radiographic feature is pleural fluid. Less frequently, thoracic radiographs show signs of pericardial effusion or enlarged tracheobronchial lymph nodes.6,7
Cats with pulmonary carcinoma may present with respiratory signs, such as dyspnoea, coughing, tachypnoea and haemoptysis, or non-respiratory signs, such as anorexia, vomiting, diarrhoea, weight loss, ataxia and lameness. 8 In a series of 17 cats with primary pulmonary neoplasia, only 36% presented with respiratory signs. 4
The association between lameness and pulmonary carcinoma, or lung–digit syndrome, is well recognised.9,10 In a retrospective study of 19 cats with metastatic pulmonary carcinoma to the digits, all presented with lameness or digital pain. 9 In another retrospective study of 64 cats with digital carcinoma, 88% of these lesions were metastases of primary pulmonary carcinoma. 10 It is uncertain why there is a propensity for pulmonary carcinoma to metastasise to the digits. It may be related to the angio-invasive properties of pulmonary carcinomas and high digital blood flow. 11 Feline pulmonary carcinomas occasionally metastasise to other sites, such as long bones, vertebrae, 12 skin13,14 or skeletal muscle. 15
Most cats with primary pulmonary neoplasia have metastases to the pleura, mediastinum or diaphragm at the time of diagnosis.1,4 Pleural fluid is a frequent finding; however, neoplastic cells are identified inconsistently in pleural fluid. No association was found between the type of cells within the fluid and the histological diagnosis. 4 In a recent study of 39 cats, intrapulmonary metastasis was most frequently observed, followed by direct spread to the pleural cavity and regional lymph nodes, and metastasis to distant organs. 1
Conclusions
Both cats in the present report had similar rib lesions as those associated with pleural metastases of pulmonary adenocarcinoma. Despite the frequency of pleural involvement in feline pulmonary carcinoma, previous reports have not included examples of direct spread to adjacent ribs. Local spread of pulmonary neoplasia from the pleural space to the ribs is recognised in humans. 16 It is possible that this pattern of local spread to the ribs has been under-diagnosed in cats. Lesions affecting the left second and third ribs were visible on the radiographs of cat 1; however, the severity and extent of these lesions, as demonstrated by the CT, were not appreciated. Similarly, the less advanced lesions affecting the right ribs could not be identified on the radiographs. This suggests that lesions affecting the ribs may not been seen in cats with less marked changes or earlier in the disease process. Increased use of CT, which enables more accurate assessment of the ribs than radiography, may lead to increased recognition of this feature.
Footnotes
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.