
Abstract
Overview:
Phaeohyphomycoses and hyalohyphomycoses are rare opportunistic infections acquired from the environment. More cases have been reported in recent years in humans and cats.
Disease signs:
Single or multiple nodules or ulcerated plaques (which may be pigmented) in the skin are the typical lesions. In some cases the infection disseminates or involves the central nervous system (CNS).
Diagnosis:
Diagnosis is based on fungal detection by cytology and/or histology. Culture provides definitive diagnosis and species identification.
Treatment:
Treatment involves surgical excision in cases of localised skin disease followed by systemic antifungal therapy, with itraconazole as the agent of first choice. Relapses after treatment are common. Itraconazole and other systemic antifungal agents have been used to treat systemic or neurological cases, but the response is unpredictable. The prognosis is guarded to poor in cats with multiple lesions and systemic or neurological involvement.
Zoonotic risk:
There is no zoonotic risk associated with contact with infected cats.
Fungal properties and epidemiology
Phaeohyphomycoses are rare opportunistic fungal infections caused by numerous genera of fungal moulds that characteristically produce melanin-pigmented ‘dematiaceous’ (dark-coloured) hyphal elements in tissues and in culture (Figures 1 and 2); yeast-like forms have also been found in some cases. 1 Hyalohyphomycoses are caused by several genera of fungi that are non-pigmented, being transparent or hyaline in tissues. 1

Dark-coloured, periodic acid-Schiff-positive, fungal structures in a tissue sample. Courtesy of Alessandra Fondati
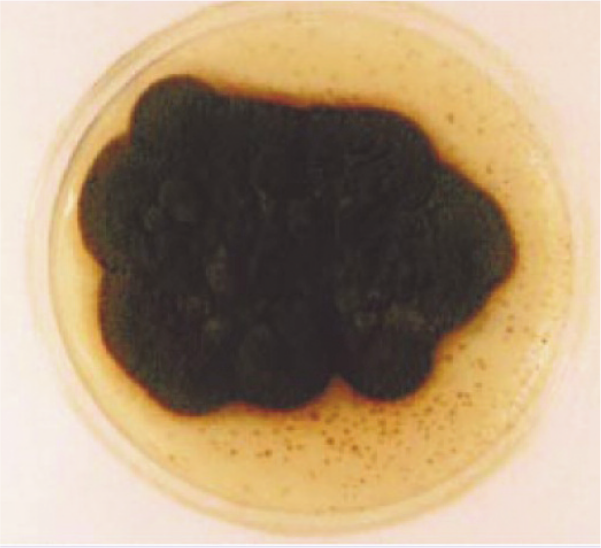
‘Dematiaceous’ (dark-coloured) colony. Courtesy of Alessandra Fondati
Both are ubiquitous saprophytic agents. The number of reports of infections is increasing in humans and animals, often associated with immunosuppressive treatment or an immunosuppressive condition. In human medicine, they are currently considered emerging fungal infections.2,3

Infections are acquired from traumatic implantation from the environment (soil and decomposed plants). Direct transmission between hosts does not occur. 1
The taxonomy of the aetiological agents is complicated, and names have often been changed. More than 100 species classified within 60 genera have been described as agents of phaeohyphomycosis in animals and humans. Pathogens for dogs and cats include species from Alternaria, Bipolaris, Cladophialophora and Curvularia. Genera with species causing disease in cats, but not in dogs, are Exophiala, Fonsecaea, Macrophomina, Microsphaerosis, Moniliella, Phialophora, Phoma, Scolecobasidium and Stemphylium.
Genera with species causing hyalohyphomycosis in dogs and cats include Fusarium, Acremonium, Paecilomyces, Pseudallescheria, Sagemonella, Phialosimplex and Scedosporium.
Feline phaeohyphomycosis probably has a worldwide distribution as sporadic cases have been reported from North America, Spain, 4 Italy,5,6 Australia, 7 Canada, 8 the UK9,10 and Japan. 11
A retrospective study from the UK evaluating 77 cats with nodular granulomatous skin lesions caused by fungal infection found that the most frequent cause was hyalohyphomycosis. Phaeohyphomycosis and deep pseudomycetomas were less frequently diagnosed. 9
Pathogenesis
Infection occurs mainly through contact or skin puncture, especially through trauma involving wood. 1 Respiratory tract colonisation is suspected to occur in systemic cases. In the rare cases of CNS infection, the route of exposure has not been elucidated, but an extension from sinuses, the orbit and middle ear has been suggested.1,12 Local infections are rarely associated with systemic diseases or immunosuppression. 1 The infrequent cases of systemic disseminated infection may or may not be associated with immunosuppression.
Clinical presentation
Nodules or masses in the skin or nasal mucosa are the most common clinical problem. Ulcerated, crusting or fistulating nodules, non-ulcerated subcutaneous nodules and/or plaques, which can be focal or multifocal and locally invasive, are typical lesions.4–11 The lesions may appear pigmented, 1 but are otherwise not different from chronic bacterial infection or cystic skin lesions. In most cases they are found in the facial region, and on the distal part of the extremities or the tail. A typical presentation is a nodule on the bridge of the nose. 4 A case of a focal pulmonary granuloma caused by Cladophialophora bantiana has been reported in a cat. 13
A few cases in the literature concern fungal infections that were responsible for multifocal neurological signs due to encephalitis or brain abscesses 12 or for disseminated disease,14,15 especially in association with immunosuppression. In these cases the causative organism has been identified as Cladosporium species. Most cases have been diagnosed post mortem.
Diagnosis
Diagnosis is based on visualisation of the fungal organism on cytology and/or histology, which usually shows a nodular to diffuse pyogranulomatous inflammation pattern. In tissue, the presence of pigmented fungal structures in the centre of the pyogranulomatous reaction is highly suggestive of phaeohyphomycosis (Figure 3).1,4–11 Special fungal stains such as Gomori methenamine silver or periodic acid-Schiff can enhance the diagnostic sensitivity.

Pigmented fungal structures in a tissue sample. Courtesy of Lluís Ferrer
Definitive diagnosis relies on fungal culture and identification of the fungal species based on morphology and pigmentation features by specialised laboratories. 1
Molecular techniques have only seldom been used to identify pathogenic fungal species. 11
Treatment
No prospective studies exist on the treatment of feline phaeohyphomycosis or hyalohyphomycosis. Recommendations are based on case reports.

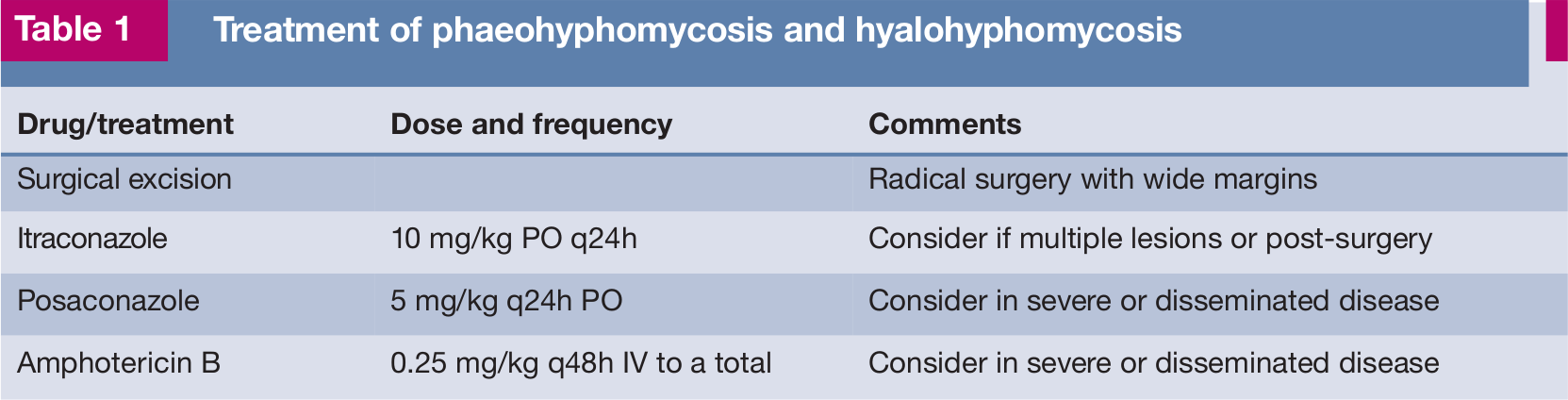
The approach for local lesions is aggressive surgical excision, as these rarely respond to antifungal treatment. After surgery of a single lesion, if multiple lesions exist or in cases of disseminated infection, itraconazole is the treatment of choice [
Table 1 lists the treatment options for these infections.
Treatment of phaeohyphomycosis and hyalohyphomycosis
There are no vaccines available.

Footnotes
Key Points
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this article. The ABCD is supported by Merial, but is a scientifically independent body.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.