
Abstract
An 8-year-old, male neutered, domestic longhair cat was referred for investigation of insulin-resistant diabetes mellitus. Routine haematology, serum biochemistry, urinalysis (including culture), total T4 and urine creatinine:cortisol ratio were unremarkable, but markedly increased insulin-like growth factor-1 concentration was identified and a pituitary mass was subsequently documented. The cat was treated conservatively with the dopamine agonist L-deprenyl and was re-presented 16 months later for worsening polyuria, polydipsia, polyphagia, marked lumbar muscle atrophy, development of a pendulous abdomen and marked thinning of the abdominal skin. Hyperadrenocorticism was diagnosed based on abdominal ultrasonography, dexamethasone suppression testing and endogenous adrenocorticotropic hormone (ACTH). The cat was treated with trilostane (30 mg q24h PO) and showed some clinical improvement, but developed an opportunistic fungal infection and skin fragility syndrome 4.5 months after commencing treatment, and was euthanased. A double-pituitary adenoma comprising a discrete somatotroph adenoma and a separate plurihormonal adenoma (positive immunoreactivity for ACTH, melanocyte-stimulating hormone and follicle-stimulating hormone) was identified on post-mortem examination. These two pituitary adenomas were suspected to have arisen as independent neoplastic entities with the plurihormonal tumour either being clinically silent at the initial presentation or having developed over the subsequent 16 months.
Case Report
Insulin-resistant diabetes mellitus can result from various concurrent metabolic, inflammatory, infectious and neoplastic diseases. Hypercortisolaemia and hypersomatrophism (otherwise termed acromegaly) are both considered relatively uncommon causes of insulin resistance in cats, but may be caused by pituitary adenomas resulting in either excessive adrenocorticotropic hormone (ACTH) or growth hormone secretion, respectively. While pituitary tumours are reportedly the third most common intracranial tumour in cats they still only comprise a small percentage of all intracranial neoplasms (8.8%) compared with dogs (25%), and are often considered incidental.1,2
This report details a cat with documented insulin-resistant diabetes mellitus due to a pituitary tumour causing hypersomatotrophism that presented 16 months after the original diagnosis, with clinical signs consistent with concurrent hypercortisolaemia. Pituitary-dependent hyperadrenocorticism was subsequently confirmed and treated medically. A double-pituitary tumour, comprising a somatotroph adenoma and a separate plurihormonal adenoma, was confirmed at post mortem following euthanasia for complications associated with skin fragility syndrome.
An 8-year-old, MN, domestic longhair cat was referred to Murdoch University with a 4-month history of diabetes mellitus and poor glycaemic control despite increasing insulin requirements. Therapy at the time of referral consisted of 15 IU (2.3 IU/kg) of glargine insulin (Lantus; Sanofi-Aventis) twice daily with repeated blood glucose curves and fructosamine evaluation (489 μmol/l; reference < 365 μmol/l) indicating poor control. The cat’s weight was stable at the time of referral and the cat was in good body condition (body condition score 6/9). Routine haematology, serum biochemistry and urinalysis (including urine culture) and urine creatinine cortisol ratio (UCCR) prior to referral had been unremarkable.
On physical examination at the time of referral the cat was alert and responsive, but had moderate stertor and an unkempt coat. Mild prognathia inferior was evident and the cat appeared to have prominent facial features. The remainder of the physical examination was unremarkable.
Serum total T4 was within the reference interval (RI) (30.4 nmol/l; RI 15–43 nmol/l), but insulin-like growth factor-1 (IGF-1), measured via a chemiluminescent assay, was markedly increased (3251 ng/ml; reference <1000 ng/ml). 3 Although measurement of IGF-1 via a validated radioimmunoassay (RIA) would have been preferred, the degree of elevation in conjunction with subsequent confirmation of a pituitary mass on evaluation with computed tomography of the brain (Figure 1) was considered most consistent with hypersomatotrophism.

Pre- (a) and post-contrast (b), soft tissue window computed tomography images at the time of the original presentation showing moderate enlargement of the pituitary gland
The owner elected to pursue conservative treatment with a dopamine agonist, L-deprenyl (5 mg q24h, then 10 mg q24h), in addition to insulin therapy (15 IU/kg q12h). Clinically, the cat remained stable with improved demeanour and reduced appetite; however, no appreciable difference with regard to glycaemic control or fructosamine values occurred. Periodic evaluation showed stable clinicopathological parameters aside from continued poor glycaemic control. Four months after initial referral, abdominal ultrasound and echocardiography were performed to evaluate progressive organomegaly and a grade II/VI left parasternal murmur, respectively. Renomegaly, hepatomegaly with hyperechoic parenchyma and myocardial hypertrophy (LVFWd 6.5 mm; normal: <5 mm) without chamber enlargement were identified.
Sixteen months after the initial diagnosis, worsening polyuria, polydipsia and polyphagia were reported, along with mild weight loss, abdominal distension and lethargy. At this time, physical examination detected marked atrophy of the thoracolumbar musculature, a distended abdomen and marked thinning of the abdominal skin. Hypercortisolaemia was primarily suspected based on physical examination.
Routine haematology, serum biochemistry and total T4 were unremarkable aside from hyperglycaemia. Urinalysis demonstrated glycosuria only, with a negative culture. UCCR measured via RIA remained within established RIs (13 × 10-6; RI 2–36 x 10-6). 4 Abdominal ultrasound identified bilateral adrenomegaly (left adrenal 6.0 mm; right adrenal 7.0 mm). 5
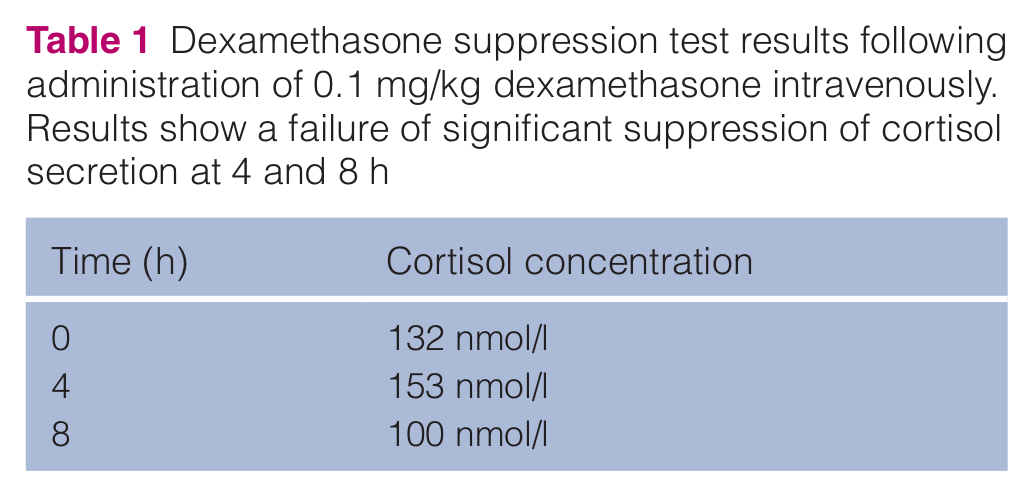
The results of dexamethasone suppression testing (0.1 mg/kg IV; Table 1) demonstrated an inability to significantly suppress cortisol secretion (0.1 mg/kg IV), and endogenous ACTH concentration was concurrently elevated (167 pg/ml; RI 10–60 pg/ml). 6 ACTH stimulation testing following intravenous administration of 125 µg of tetracosatrin (Synacthen; Novartis Pharmaceuticals) was performed with blood collection at 0, 60, 90 and 180 mins (Table 2). Combined clinicopathological findings were considered consistent with pituitary-dependent hypercortisolaemia.
Dexamethasone suppression test results following administration of 0.1 mg/kg dexamethasone intravenously. Results show a failure of significant suppression of cortisol secretion at 4 and 8 h
Adrenocorticotropic hormone (ACTH) stimulation test results following administration of 125 µg of tetracosatrin intravenously (Synacthen; Novartis Pharmaceuticals). Results at diagnosis showed an appropriate, but not exaggerated, increase in cortisol post-ACTH stimulation, as seen in 40–50% of cats with hyperadrenocorticism.26–30 Results at day 44 post-trilostane therapy commencing (30 mg q24h PO) showed a significant reduction in serum cortisol concentrations

Medical management with trilostane (30 mg q24h PO) improved glycaemic control to the extent that hypoglycaemia occurred 13 days after therapy had commenced (2.8 mmol/l; RI 3.8–6.1 mmol/l). Fructosamine evaluation at this time also indicated probable prolonged hypoglycaemia (207 µmol/l; RI <365 µmol/l) and insulin dosage was therefore reduced (11 IU q12h SC; 1.5 IU/kg) which provided adequate glycaemic control. ACTH stimulation testing could not be repeated until day 44, at which time it showed a reduction in pre- and post-ACTH cortisol concentrations compared with baseline (Table 2). The cat remained clinically well with a good appetite and body condition, but there was no change in physical condition.
The cat was euthanased 4.5 months after the diagnosis of hyperadrenocorticism due to skin fragility syndrome that resulted in an 8 cm skin tear across the right caudal abdomen. Concurrently, the cat had also developed a facial abscess from which Trichophyton mentagrophytes was cultured.
Post-mortem examination identified a markedly enlarged pituitary gland (12 × 10 × 9 mm). A well-demarcated, 4 mm diameter, white nodule confluent with the subjacent pituitary gland was identified within the hypothalamus causing associated focal compression of the third ventricle (Figure 2a). A second, larger nodule (10 × 7 × 4 mm) occupied the majority of the enlarged pituitary gland and caused ventrolateral deviation and compression of the remaining pituitary tissue and dorsolateral compression of the hypothalamus (Figure 3a). Additional findings included generalised skeletal muscle atrophy and organomegaly, including hepatomegaly, renomegaly and cardiomegaly with left ventricular hypertrophy.

Somatotroph adenoma. (a) Brain and pituitary gland, transverse section. A white nodule (asterisk), 4 mm in diameter, is present within the hypothalamus to the right of midline, causing medial deviation of the hypothalamus and compression of the third ventricle (arrow). (b) Pituitary adenoma (haematoxylin and eosin). Neoplastic cells have abundant acidophilic cytoplasm, and form sheets and packets separated by a fine fibrovascular stroma. (c) Pituitary adenoma. Neoplastic cells demonstrate strong cytoplasmic immunoreactivity for growth hormone. (d) Neoplastic cells are negative for adrenocorticotropic hormone. Positive cytoplasmic immunolabelling is present in a proportion of cells in the adjacent, compressed normal pituitary gland. (e) Scattered cells label positively for follicle-stimulating hormone. (f) Neoplastic cells are negative for melanocyte-stimulating hormone. A proportion of cells in the compressed normal pituitary gland exhibit positive immunolabelling

Plurihormonal adenoma. (a) Brain and pituitary gland, transverse section. A second nodule (asterisk) expands the pituitary gland, causing ventromedial deviation of the pituitary tissue and dorsolateral compression of the hypothalamus. (b) Pituitary adenoma. The neoplasm is composed of round-to-polygonal chromophobic cells, arranged in packets and cords separated by a fine fibrovascular stroma (haematoxylin and eosin). (c) Neoplastic cells demonstrate strong cytoplasmic immunoreactivity for adrenocorticotropic hormone. (d) Neoplastic cells exhibit positive cytoplasmic immunolabelling for follicle-stimulating hormone. (e) Neoplastic cells exhibit positive cytoplasmic immunolabelling for melanocyte-stimulating hormone. (f) Neoplastic cells are negative for growth hormone. A proportion of cells in the compressed normal pituitary gland have positive immunolabelling
Microscopic examination confirmed the nodules as two distinct neoplasms. The smaller pituitary nodule (Figure 2b) comprised an unencapsulated proliferation of polygonal cells forming sheets and packets within a fine fibrovascular stroma. Neoplastic cells had abundant, acidophilic cytoplasm, distinct cellular borders and round-to-oval nuclei with stippled chromatin and prominent nucleoli. The larger nodule (Figure 3b) consisted of a well demarcated, unencapsulated and expansile neoplasm composed of chromophobic cells arranged in sheets separated by a delicate fibrovascular stroma. Neoplastic cells were round-to-polygonal and rarely elongated, with distinct cellular borders and a moderate amount of amphophilic cytoplasm. Nuclei were round-to-oval with finely stippled chromatin and 1–2 variably prominent nucleoli. The second nodule also contained areas of necrosis and scattered inflammatory cells, including neutrophils, macrophages, lymphocytes and plasma cells.
Immunohistochemical labelling was performed on sections from both tumours for growth hormone (GH), ACTH, melanocyte-stimulating hormone (MSH), follicle stimulating hormone (FSH), thyroid-stimulating hormone (TSH) and β-endorphin following previously published protocols.7,8
The acidophilic cells comprising the smaller tumour demonstrated strong, diffuse cytoplasmic positivity for GH, and were negative for ACTH and MSH. Scattered neoplastic cells were positive for β-endorphin, while, at the periphery of the tumour, rare intercalated cells were positive for FSH and TSH (Figure 2c–f). This immunolabelling pattern was consistent with a somatotroph pituitary adenoma. The chromophobic cells comprising the larger tumour displayed strong positive cytoplasmic labelling for ACTH, MSH, FSH and β-endorphin, but were negative for GH and TSH, consistent with a plurihormonal pituitary tumour (Figure 3c–f).
Double or multiple pituitary adenomas, comprising more than one discrete tumour type, are reported occasionally in humans, with the majority comprising separate prolactin (PRL) secreting and non-functional, null-cell adenomas.9–11 Plurihormonal adenomas, consisting of a single tumour demonstrating immunoreactivity for and/or systemically secreting at least two functionally unrelated hormones are rare.9,10,12 Where identified, plurihormonality of pituitary tumours is most frequent in adenomas predominantly secreting GH.13–15 Plurihormonal type I adenomas are described as secreting combinations of GH, PRL and glycoprotein hormones, while secretion of FSH, LH, and TSH or GH is identified in plurihormonal type II adenomas.9,11 Other combinations are exceptionally rare.16,17
Excessive ACTH immunopositivity is uncommon for single, double or plurihormonal adenomas in humans and, for the latter, often does not contribute to clinical disease.10,11 Where plurihormonal ACTH tumours do occur, concurrent PRL secretion is, again, most common.9–11 Concomitant expression of other hormones, such as FSH or GH, has been described, but positive immunoreactivity for these hormones is often considered insignificant and/or clinically silent.10,15 For plurihormonal type I and II tumours, the patterns of hormonal expression suggest cytogenesis from common cellular lineages.16,18–20 Cytogenesis of mixed-lineage pituitary tumours, however, remains unresolved, but is postulated to result from aberrant expression of transcription factors leading to abnormal cytodifferentiation and/or altered hormonal production.15,21
Double, multiple and plurihormonal pituitary adenomas are exceedingly rare in animals.22–24 Two previous reports document cats with double or plurihormonal pituitary tumours. In the first, a double pituitary lesion comprising separate ACTH and GH adenomas was identified. 22 Concurrent systemic elevations in GH and IGF-I were identified. The second documented a plurihormonal adenoma with positive immunoreactivity to ACTH, GH and MSH. Evaluation for concurrent systemic elevations of these hormones was not performed. 24 In both cases, clinical signs of insulin-resistant diabetes mellitus and hyperadrenocorticism were evident at presentation.
In comparison, the cat described here had two distinct clinical presentations over 16 months. Separate somatotrophic and plurihormonal adenomas were identified which, based upon these two distinct clinical presentations, were suspected to have arisen separately. The possibility of concurrent hyperadrenocorticism contributing to insulin resistance at the initial presentation cannot be excluded completely, but is unlikely based upon the clinicopathological data at that time. At the second presentation ACTH stimulation testing (Table 2) was normal but other clinicopathologic findings were considered compatible with hyperadrenocorticism. Chronic L-deprenyl therapy may have attenuated an expected response, although this is not seen in dogs with hyperadreoncorticsm. 25 What is probably more likely is that ACTH stimulation testing exhibits poor sensitivity in this species, and, based upon previous reports, exaggerated responses to ACTH stimulation may only be expected in 50–60% of cats with hyperadrenocorticism.26–30
The plurihormonal adenoma showed positive immunohistochemical labelling for ACTH, FSH and MSH, representing an unusual mixed-lineage pituitary tumour, likely due to aberrant cytodifferentiation and/or altered hormone transcription secondary to neoplastic transformation, as proposed in humans. Concomitant systemic increases in circulating concentrations of FSH and MSH were, unfortunately, not confirmed; therefore, their clinical significance is undetermined. Concurrent α-MSH secretion and/or immunopositivity for α-MSH appears relatively common in cats with ACTH secreting pituitary adenomas.24,31 This could suggest tumour cytodifferentiation arises from the pars intermedia in the majority of cases.
Medical management of both acromegaly and hyperadrenocorticism had limited success in this case. L-deprenyl had no demonstrable effect on the control of diabetes mellitus. However, whether or not chronic administration contributed to development of the second plurihormonal adenoma remains unknown. Excessive circulating corticotropin-releasing hormone (CRH) arising from either ectopic production or loss of negative feedback on the hypothalamus has certainly been documented to result in pituitary corticotroph hyperplasia in humans.32–35 Excessive CRH production or altered CRH receptor expression are therefore potential mechanisms by which pituitary tumour development may be promoted.34,35 In this cat L-deprenyl could, theoretically, have contributed to pituitary tumorigenesis by limiting negative feedback on the hypothalamus by ACTH and cortisol, consequently enhancing CRH secretion. This does not, however, appear to be a common clinical scenario in humans undergoing chronic dopamine agonist therapy. After the diagnosis of hyperadrenocorticism, trilostane improved glycaemic control and serum cortisol concentrations decreased. Other clinical findings remained unchanged, however, and the cat succumbed to complications of excessive cortisol secretion. Whether a longer treatment period might have resolved these signs remains unclear. Previous reports of cats treated medically for hyperadrenocorticism commonly show improvement in attitude and activity, while physical parameters remain unchanged unless long-term therapy is successful.28,36 Bilateral adrenalectomy, radiotherapy and hypophysectomy have also been described as therapies for pituitary hyperadrenocorticism in cats.29–31,37–44 Radiotherapy may temporarily resolve or control DM; however, acromegalic and hyperadrenocorticoid changes frequently persist.40–43,45,46
This is the second report of a cat with two discrete, morphologically distinct pituitary lesions consisting of a somatotrophic adenoma and a separate plurihormonal adenoma with positive immunohistochemistry for ACTH, FSH and MSH. These two pituitary adenomas were considered likely to have arisen from separate cytodifferentiation. Pituitary tumours that comprise more than one distinct adenoma type or that concurrently produce more than one pituitary hormone are likely rare in cats, but could be a potential cause of insulin resistance.
Footnotes
Acknowledgements
We wish to thank Dr Philip Nicholls and Dr Melissa Sanchez for their assistance with the pathology, and Dr Caroline Mansfield for assistance with the manuscript.
Funding
The authors received no specific grant from any funding agency in the public, commercial or not-for-profit sectors for the preparation of this case report.
Conflict of interest
The authors do not have any potential conflicts of interest to declare.